
Abstract
Abstract
Counter, S. Allen, Leo H. Buchanan, Fernando Ortega, Anthony B. Jacobs, and Göran Laurell. Middle ear function and pathophysiology in Andean children living at high altitudes. High Alt Med Biol. 18:163–170, 2017.—The extent of altitude-related middle ear disorders in children native to high altitudes is unclear. This study examined middle ear pathophysiology in two groups of children living in high-altitude Ecuadorian Andean communities by investigating middle ear pressure (MEP), tympanic membrane compliance (TMC), and ear canal volume (ECV) using tympanometry, and by otological examination. Altitude I Group lived at 2850 m, and Altitude II Group resided at around 4000 m. The two high-altitude groups were compared with a reference group of children residing at sea level. Mean MEP was −3.6 daPa (SD: 39.2), 3.5 daPa (SD: 28.7), and 1.3 daPa (SD: 13.6) for Altitude I Group, Altitude II Group, and the Sea Level Group, respectively. The MEP was not significantly different among the three groups. Mean TMC was 0.63 cm3 (SD: 0.51), 0.60 cm3 (SD: 0.43), and 0.60 cm3 (SD: 0.24) for Altitude I Group, Altitude II Group, and the Sea Level Group, respectively. The TMC was not significantly different among the three groups. Mean ECV was 1.1 (SD: 0.26), 1.2 (SD: 0.26), and 1.0 (SD: 0.23) for Altitude I Group, Altitude II Group, and the Sea Level Group, respectively. The difference in ECV between Altitude I Group and Altitude II Group was significant (p = 0.043), as was the difference between Altitude II Group and the Sea Level Group (p = 0.001). ECV did not differ significantly between Altitude I Group and the Sea Level Group. Otological examination revealed a low incidence of ear canal and middle ear pathology. In conclusion, tympanometric and otological findings did not reveal a high incidence of middle ear pathophysiology in children living at altitudes as high as around 4000 m.
Introduction
A
The current study investigated middle ear pathophysiology in children who have lived their entire lives at high altitudes. Lifetime inhabitants of high-altitude environments have developed physiological adaptations to high-altitude living, and, therefore, they may exhibit different effects of hypobaric hypoxia than people living at low elevations (Scheinfeldt and Tishkoff, 2010; Simonson, 2015). The auditory effects of acute hypoxia in children who live at low altitudes and travel to high altitudes have received considerable study. However, the effects of low-oxygen environments on the auditory system of children who have lived their entire lives at high altitudes have received less medical and scientific attention. The purpose of the present study was to investigate middle ear pathophysiology by examining MEP, tympanic membrane compliance (TMC) or acoustic admittance (reciprocal of impedance), and ear canal volume (ECV) by using clinical tympanometric procedures in children living at high altitudes in Andean communities in Ecuador during ongoing medical evaluations. In addition, otoscopic and audiological examinations were conducted to assist in the identification of ear canal and middle ear pathophysiology in the children.
Materials and Methods
Participants and locations
This study consisted of a total of 99 Andean children (54 girls and 45 boys) aged 2–17 years (mean age: 9.9; SD: 3.4; median age: 10 years) who comprised two groups living at high elevations in La Victoria (Altitude I Group) and in the Guangaje Andean communities of Curingue and Tingo Pucará (Altitude II Group) in Ecuador, South America. The children were examined by tympanometry as part of an audiological clinical battery during general medical and otological examinations.
Altitude I Group
The Altitude I Group comprised 52 children who live and conduct their daily activities at around 2800 m above sea level in the west ranges of the Andes in Cotopaxi Province, Ecuador, in the community of La Victoria. The children in this group ranged in age from 3.0 to 17.0 years, with a mean age of 9.9 years (±3.5 years) and a median age of 10.0 years. The children in the Altitude I Group consisted of 24 boys (age range: 3.0 to 17.0; mean age: 10.5; SD: 4.1; median: 10.8 years) and 28 girls (age range: 5.0 to 15.1; mean age: 9.4; SD: 2.8; median: 10.0 years). The participants in the Altitude I Group consisted mainly of children of indigenous Quechua Indian ethnicity and mixed Spanish/indigenous Indian backgrounds who had lived all of their lives at Altitude I.
Altitude II Group
The Altitude II Group consisted of 47 children tested at around 3973 m above sea level in the Andean community of Guangaje (Curingue and Tingo Pucará villages). This largely shepherd population lives and conducts its daily activities between 3500 and 4200 m in the west ranges of the Andes in Cotopaxi Province, Ecuador. The 47 children ranged in age from 2.0 to 17.0 years, with a mean age of 9.9 years (±3.5 years) and a median age of 10.0 years. This higher altitude group consisted of 21 boys (age range: 2.0 to 15.7; mean age: 9.7; SD: 3.8; median: 10.0 years) and 26 girls (age range: 4.6 to 17.0; mean age: 10.1; SD: 3.3; median 9.8 years). The children in the Altitude II Group were of an indigenous Quechua Indian background, and they had lived all of their lives at Altitude II. Previous medical assessments of children and adults in the Curingue and Tingo Pucará areas have indicated widespread malnutrition.
Sea Level Group
The middle ear function data obtained on the high-altitude groups (Altitude I and Altitude II groups) were compared with a Sea Level Group residing at ∼20 m elevation in the United States. The Sea Level reference group consisted of 50 participants who were tested in a conventional clinical setting at sea level by tympanometry during standard audiological evaluations. The participants in the Sea Level Group ranged in age from 6.2 to 17.6 years (mean: 11.8; SD: 3.0; median: 11.6 years), and the group consisted of 31 boys and 19 girls. All children in the Sea Level Group had normal hearing, normal otoscopic exams, and a negative history of tympanic membrane tympanostomy tube placement. The children in the Sea Level Group were of a Caucasian background and had lived all their lives at sea-level elevation.
Informed consent was obtained from the parents or guardians of all children before testing. This study was conducted under the auspices of Universidad San Francisco de Quito in Quito, Ecuador, and was approved by the Human Studies Committee (Comité de Bioética) of Universidad San Francisco de Quito.
Audiological and otological examination procedures
Each participant underwent a conventional audiological evaluation, which included pure-tone air conduction threshold measurement, and bone conduction measurement where indicated. Pathology of the ear canal and middle ear was first determined via otological examination by an experienced otolaryngologist. Otological evaluation included otoscopic examination of the ear canal for ceruminosis, pathology, and epithelial debris; inspection of the tympanic membrane for retraction, tympanosclerosis, perforation, and other abnormalities; and examination of the middle ear via the translucent tympanic membrane for indications of otitis media and other pathology. The pathophysiology of the ear canal and middle ear was examined further by performing tympanometry to assess MEP, TMC, and ECV. Tympanometry is a reliable, noninvasive tool for measuring TMC, MEP, and ECV in determining the pathophysiological status of the middle ear. Tympanometry is based on measurement of the acoustic immittance/impedance of the ear, which determines how much energy of a probe tone is transmitted from the ear canal to the tympanic membrane, or how much of that probe tone energy is reflected back from the tympanic membrane, indicating the status of the ear canal, the tympanic membrane, and the middle ear system.
Tympanograms were recorded with the TympStar immittance system (Grason-Stadler, Eden Prairie, MN) by using a probe tone frequency of 226 Hz. The probe was hermetically sealed at the entrance to the external ear canal in each participant, and tympanometry was performed to examine the status of the ear canal, the tympanic membrane, and the middle ear system. Before deployment in the field in the Andes Mountain of Ecuador, the TympStar system was calibrated in a sea-level U.S. laboratory in accordance with the American National Standards Institute (ANSI, 1987) specifications for acoustic immittance instruments. The instrument was not calibrated for altitude because this is the parameter that the study was investigating. However, daily volume measurements of the TympStar system were obtained with calibrated test cavities of 0.5 and 2.0 cm3 supplied with the instrument to ensure that the instrument displayed stable volume measurements in the challenging field-testing environments at the two high altitudes. In addition, tympanometry was performed daily in the field on normal hearing staff to serve as a biological calibration check and to continually monitor the status of the equipment.
This study was conducted in the field in a nonstandard clinical situation, and it was, thus, subject to the variables of fieldwork. Field investigations, unlike controlled clinical environments, involve uncontrollable conditions and constraints, such as participants' school schedules, time limitations, and availability. Because of some of these constraints, all standard clinical tympanometry and audiological measures, as well as otoscopic examinations could not be performed on every participant in the study groups.
Statistical analysis
For statistical analysis, the means, standard deviations, medians, ranges, and percentiles were calculated for all quantitative variables. Because some of the variables were found to have skewed distributions (≥2 standard errors of skewness), nonparametric statistical tests were used for data analysis and determination of statistical significance. The Mann–Whitney U test was used to assess the difference between the Altitude I Group and the Altitude II Group for MEP, TMC, and ECV. The Mann–Whitney U test was also used to probe for differences between the Altitude I Group and the Sea Level Reference Group, and between the Altitude II Group and the Sea Level Reference Group for MEP, TMC, and ECV. The Spearman rho correlation coefficient was used to probe for associations between MEP and age, between TMC and age, and between ECV and age. All p-values reported for the Spearman rho correlation coefficient are tied p-values. An alpha level of ≤0.05 was accepted as an indication of statistical significance.
Results
Figure 1A–D shows examples of tympanometric recordings illustrating normal as well as pathological conditions of the tympanic membrane and middle ear system for four higher altitude participants from the Altitude II Group in this study. Overall, high-altitude tympanometry measurements and otoscopy revealed a number of external ear canal, tympanic membrane, and middle ear conditions for the study groups.
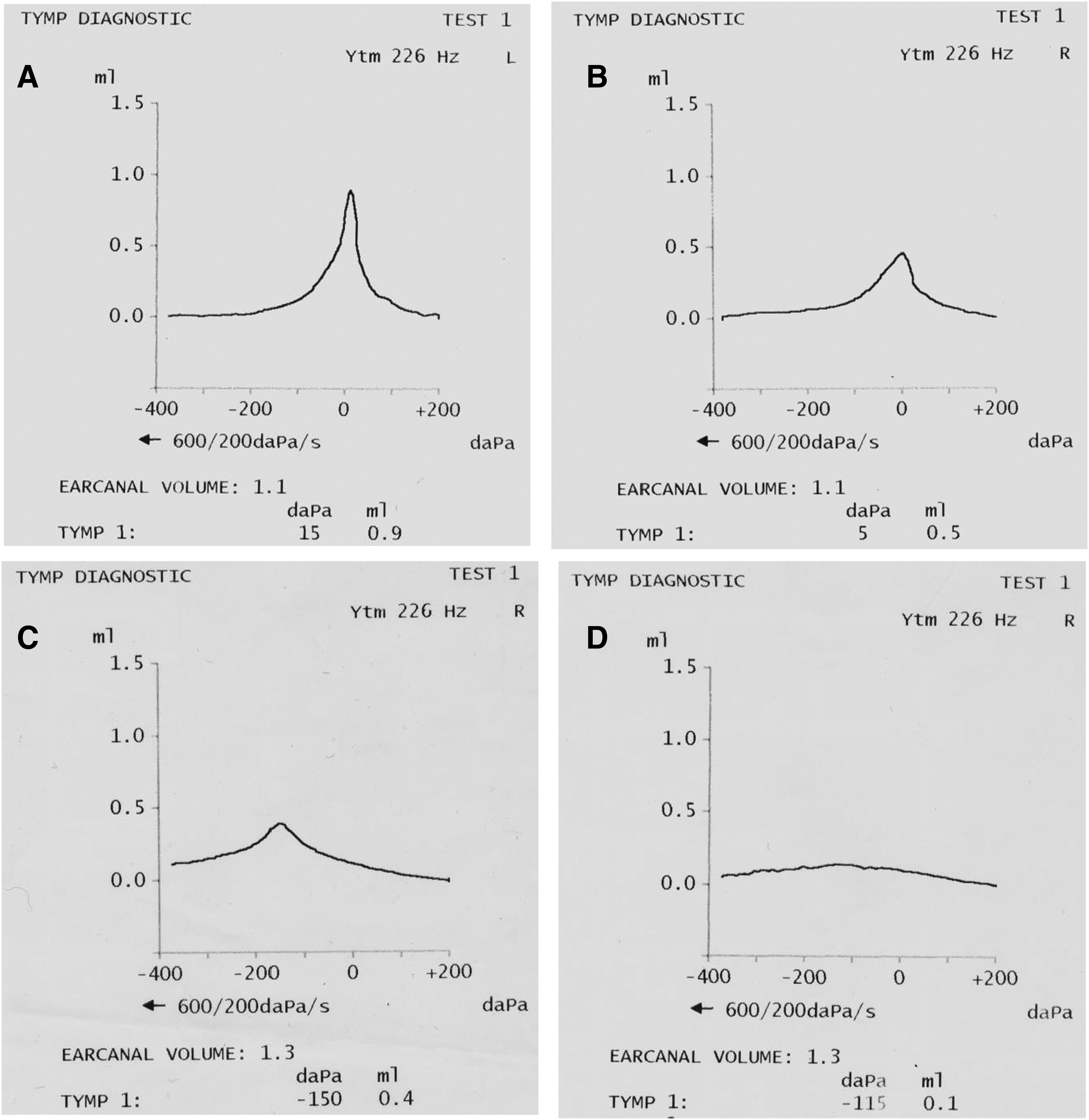
Figure 1A is a recording from the left ear of a 14-year-old boy showing a normal tympanogram depicting normal MEP (15 daPa), normal TMC (0.9 cm3 [mL]), and normal ECV (1.1 cm3). [For normative tympanometry values, refer to Haapaniemi, 1996; Shanks and Shohet, 2009.] Audiological evaluation showed normal hearing in both ears. Otoscopic examination revealed a normal tympanic membrane in the left ear, and excessive cerumen in the right ear.
Figure 1B shows a normal tympanogram recorded from the right ear of an 11-year-old boy with normal hearing. Compared with the normal tympanogram in Figure 1A, this participant shows a less compliant tympanic membrane (0.5 cm3 versus the 0.9 cm3 of Fig. 1A), but still within the normal range. Otoscopic examination revealed normal ear canals, normal tympanic membranes, and a normal-appearing middle ear bilaterally. The tympanogram showed normal MEP (5 daPa), normal TMC (0.5 cm3 [mL]), and normal ECV (1.1 cm3).
Figure 1C shows a tympanogram for the right ear of a 12-year old boy with normal hearing, but with significant negative MEP (the peak of the tympanogram is displaced left to −150 daPa), normal TMC (0.4 cm3 [mL]), and normal ECV (1.3 cm3). Otoscopic examination revealed a retraced tympanic membrane in the right ear, which is in agreement with the negative MEP. These findings are consistent with Eustachian tube dysfunction, and if persistent, could lead to middle ear effusion. Because of the Eustachian dysfunction, it is recommended that the child's ears be checked periodically by a nurse or physician to monitor the status of his tympanic membrane and middle ear for potential development of otitis media.
Figure 1D displays an essentially “flat” recording from the right ear of a 10-year-old girl. The flat curve from this participant showed an abnormally low TMC of 0.1 cm3, indicating a hypomobile tympanic membrane/middle ear system. The ECV of 1.3 cm3 was within the normal range, giving evidence of an intact tympanic membrane without perforation. Audiological testing revealed a mild to moderate conductive hearing loss in the right ear and normal hearing in the left ear. Otological examination revealed a retracted tympanic membrane in the right ear and excessive wax in the left ear. The tympanometric results, specifically the abnormal TMC value, and otoscopic examination suggested that this participant had middle ear effusion. It was recommended that this child be followed by a physician who was experienced in pediatric ear disorders.
Table 1 shows the percentage of children with specified otological and audiological diagnoses, indicating ear canal, tympanic membrane, and middle ear pathology, as well as hearing loss in indigenous Andean children living at Altitude I and Altitude II. Most of the children in both altitude groups showed normal hearing and normal otological examinations. Two children in the Altitude I Group (a 6-year-old boy and a 6-year-old girl), and two children in the Altitude II Group (a 9-year old boy and a 12-year-old girl) were found to have otitis media. The most prevalent otological finding was impacted/excessive dry cerumen in both high-altitude groups. One child in the Altitude I Group had a unilateral ear canal atresia with malformation of the pinna, and one child in the Altitude I Group presented with a cleft palate. Three children in the Altitude I Group were found to have conductive hearing losses related to ear canal atresia, cleft palate, and impacted cerumen. Four children in the Altitude II Group presented with conductive hearing losses due to otitis media and excessive/impacted cerumen.
TM, tympanic membrane.
The box plots of Figure 2 show the distribution of MEP for the Altitude I Group, the Altitude II Group, and the Sea Level Reference Group. The mean MEP was −3.6 daPa (SD: 39.2; median: 10.0; range: −135.0–35.0 daPa), 3.5 daPa (SD: 28.7; median: 10.0; range: −150.0–40.0 daPa), and 1.3 daPa (SD: 13.6; median: 5.0; range: −60.0 to 20.0 daPa) for the Altitude I Group, the Altitude II Group, and the Sea Level Group, respectively. The Altitude II Group tended to show a higher positive MEP than the other two groups, but this difference did not reach statistical significance. The mean MEP was clinically normal for the two high-altitude groups. Approximately 85% of the children in the Altitude I Group and 94% of the children in the Altitude II Group showed MEP values between −25 and +30 daPa, which were within the normal range. The MEP for the boys and girls in the Altitude I Group was significantly different (Mann–Whitney U, p = 0.031), with the boys showing a mean negative pressure of −17.5 daPa, and the girls revealing a mean positive pressure of 8.0 daPa. For the Altitude II Group, the MEP between boys and girls was not significantly different. Analyses using Spearman rho correlation coefficient revealed no significant associations between MEP and age for the two high-altitude groups.
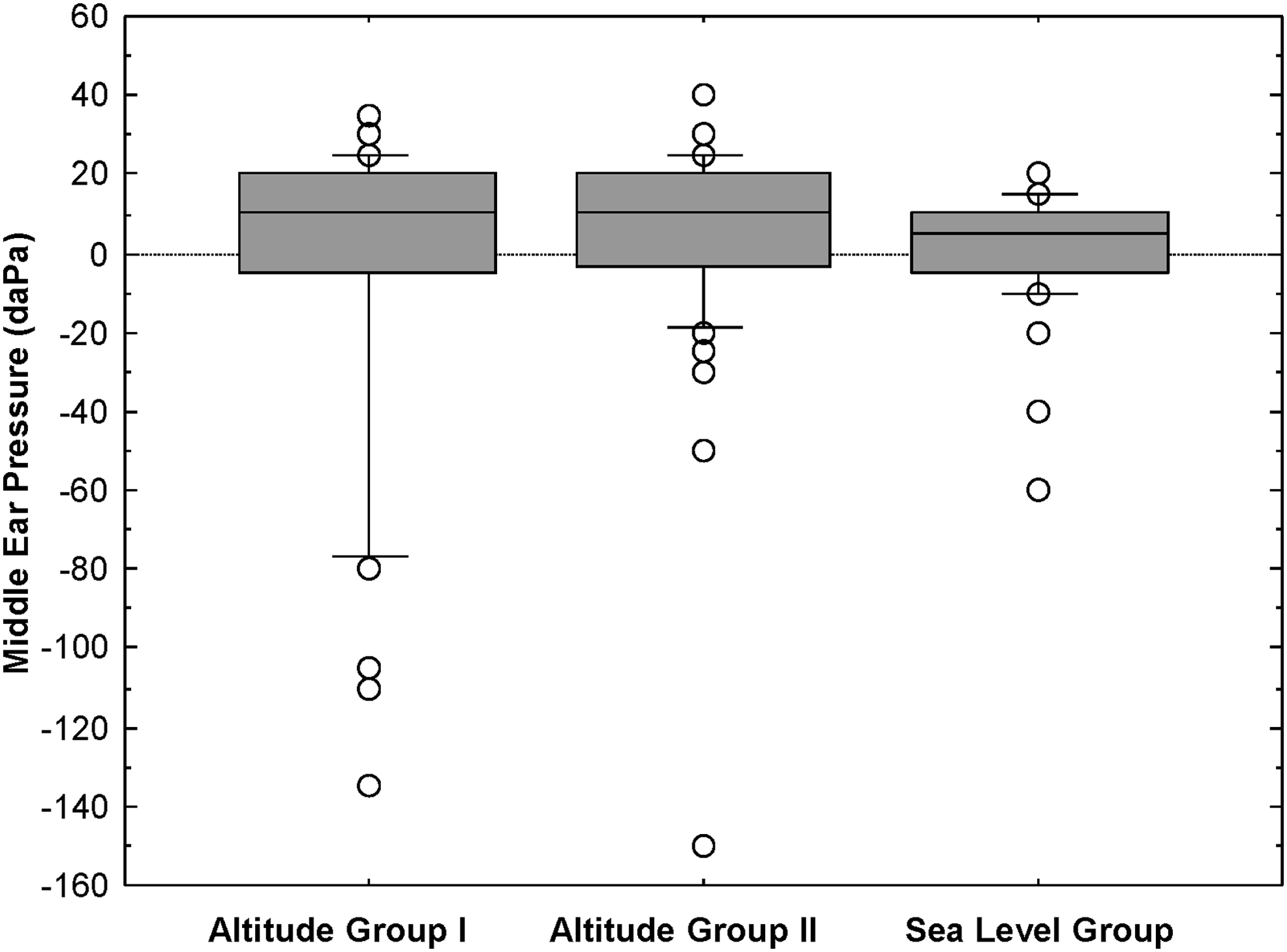
Distribution of MEP for the Altitude I Group (∼2850 m above sea level), the Altitude II Group (∼3973 m above sea level), and the Sea Level Reference Group (∼20 m elevation). The boxes contain individual MEP values between the 25th and 75th percentiles. The horizontal lines inside the boxes represent the 50th percentile. The small horizontal lines above the boxes represent the 90th percentile, and the small horizontal lines below the boxes represent the 10th percentile. The individual data points represent cases above the 90th percentile and below the 10th percentile.
Figure 3 illustrates the TMC for the Altitude I Group, the Altitude II Group, and the Sea Level Reference Group. The mean TMC was 0.63 cm3 (SD: 0.51; median: 0.50; range: 0.10–3.3 cm3), 0.60 cm3 (SD: 0.43; median: 0.50; range: 0.20–2.5 cm3), and 0.60 cm3 (SD: 0.24; median: 0.50; range: 0.30–1.30 cm3) for the Altitude I Group, the Altitude II Group, and the Sea Level Group, respectively. The results showed no significant difference in TMC or tympanic membrane mobility between the Altitude I Group and the Altitude II Group, and the TMC for the two altitude groups was not significantly different from the Sea Level Group. In addition, both high-altitude groups showed clinically normal mean TMC based on sea-level norms. Approximately 88% of the children in the Altitude I Group and 89% of the children in the Altitude II Group showed TMC values between 0.3 and 1.2 cm,3 which were within the normal range. The TMC for the boys and girls was not significantly different for the Altitude I Group and the Altitude II Group. Spearman rho correlation analyses revealed no significant association between TMC and age for the Altitude I Group, but the Altitude II Group showed a significant association between TMC and age (p = 0.013). The association between age and TMC for the Altitude II Group remained significant when two statistical outliers aged 13 years with TMC values of 2.5 and 2.25 cm3 were temporarily removed from the dataset (p = 0.042).
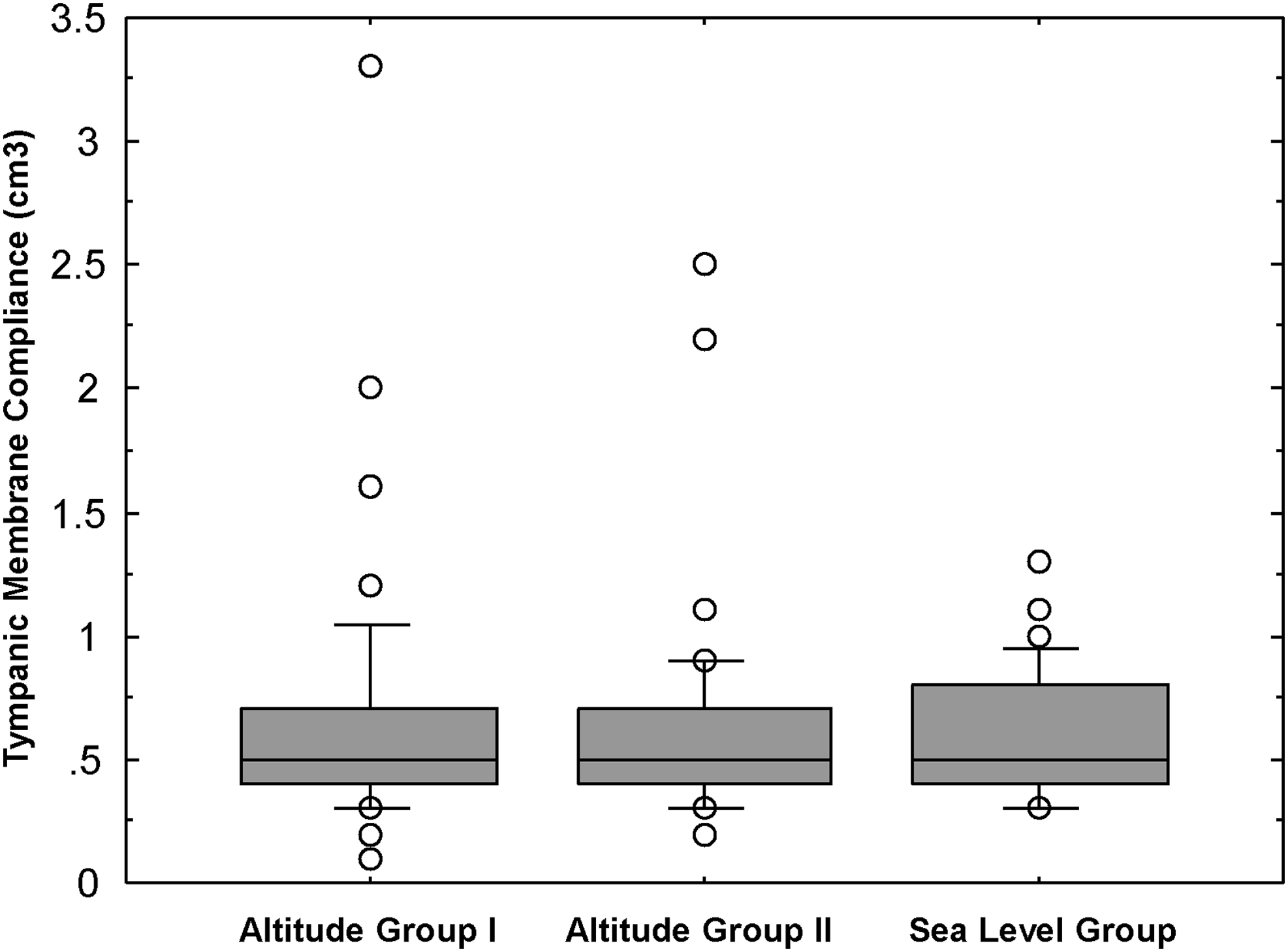
Distribution of TMC for the Altitude I Group, the Altitude II Group, and the Sea Level Reference Group. See Figure 2 legend for a description of the box plots. The results showed no significant differences in TMC among the three groups.
The box plots of Figure 4 show the results of ECV for the Altitude I Group, the Altitude II Group, and the Sea Level Group. The mean ECV was 1.1 cm3 (SD: 0.26; median: 1.1; range: 0.60–1.80), 1.2 (SD: 0.26; median: 1.1; range: 0.70–2.0 cm3), and 1.0 cm3 (SD: 0.23; median: 1.0; range: 0.60–1.6 cm3) for the Altitude I Group, the Altitude II Group, and the Sea Level Group, respectively. The difference in ECV between the Altitude I Group and the Altitude II Group was statistically significant (Mann–Whitney U, p = 0.043), as was the difference between the Altitude II Group and the Sea Level Group (Mann–Whitney U, p = 0.001). The ECV did not differ significantly between the Altitude I Group and the Sea Level Group. Ninety-two percent of the children in the Altitude I Group obtained normal ECV values between 0.5 and 1.5 cm3, and 94% of the children in the Altitude II Group obtained normal ECV values between 0.7 and 1.5 cm3. The boys showed a significantly higher ECV (Mann–Whitney U, p = 0.038) than the girls for the Altitude I group, but the difference between the boys and the girls for the Altitude II Group was not significant. Spearman rho correlation coefficient revealed significant associations between ECV and age for the Altitude I Group (rho = 0.514; p = 0.0002) and between ECV and age for the Altitude II Group (rho = 0.594; p = 0.0001) in which the ECV increased with age for both high-altitude groups.
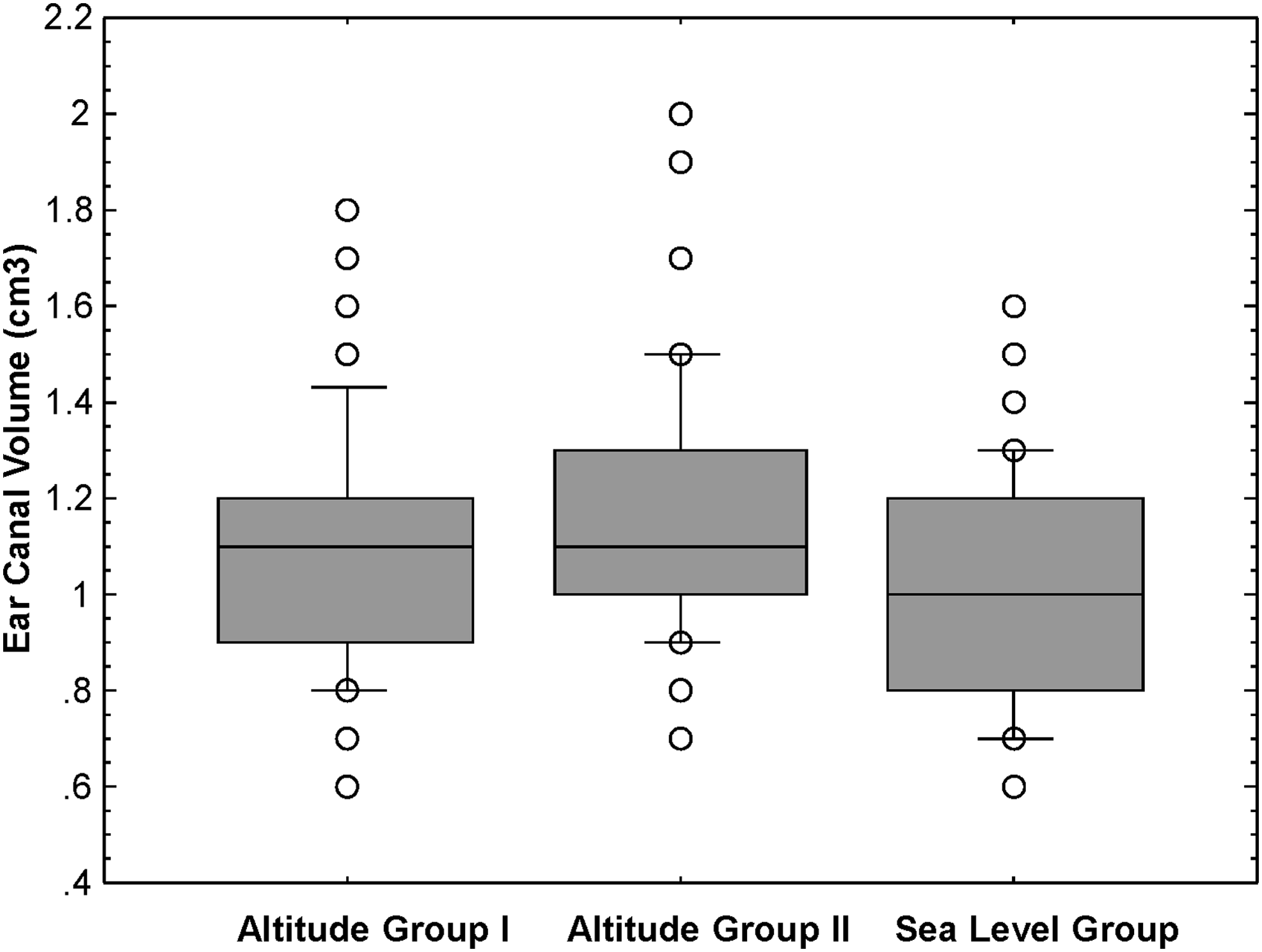
ECV for the Altitude I Group, the Altitude II Group, and the Sea Level Reference Group. See Figure 2 legend for a description of the box plots. The difference in ECV between the Altitude I Group and the Altitude II Group was statistically significant (p = 0.043), as was the difference between the Altitude II Group and the Sea Level Group (p = 0.001). The difference in ECV between the Altitude I Group and the Sea Level Group was not statistically significant.
Discussion
In a previous investigation, the authors examined the effects of altitude on the brainstem-mediated acoustic middle ear muscle reflex in the same cohort of children living at high altitudes. That study revealed no adverse effects of altitude on the acoustic middle ear reflex in children living between about 2800 and 4000 m above sea level (Counter et al., 2017). The current study investigated middle ear pathophysiology by using noninvasive tympanometry and otological procedures in children living in high-altitude environments in Andes Mountain communities in Ecuador. In addition to acute mountain sickness, cerebral edema, and pulmonary edema, high-altitude exposure (hypobaric hypoxia) has been associated with middle ear disorders from otic barotrauma in people who travel from low to high altitudes. In the current study, the authors compared MEP, TMC, and ECV for children living their entire lives at two high altitudes, ∼2850 and ∼4000 m above sea level, with children residing at sea level.
The MEP results for children living at Altitude I, Altitude II, and sea level were similar. Although a small number of the children showed negative MEP that was suggestive of Eustachian tube dysfunction, the majority of the children in the Altitude I and Altitude II Groups exhibited MEP within the clinically normal range using sea-level normative values. The MEP is regulated by a normally functioning Eustachian tube. The Eustachian tube is an osseous-cartilaginous tube, ∼35 mm in length and 3 mm in diameter (in adults), that runs from the nasopharynx to the anterior wall of the middle ear cavity. The primary function of the Eustachian tube is to equilibrate the MEP with atmospheric pressure. At high altitudes where the atmospheric pressure is lower, people adapted to sea-level ambient pressure may develop otic barotrauma while ascending to high elevations, but more frequently while descending from a higher elevation to a lower altitude. During ascent, as the atmospheric pressure is reduced, the MEP is greater (positive) relative to the ambient pressure, forcing the tympanic membrane in a lateral direction toward the ear canal. This bulging out of the tympanic membrane may cause discomfort or pain, and if the pressure on the tympanic membrane is great enough, the membrane could perforate or rupture. During descent, reverse pressure conditions exist, in which negative MEP (i.e., less pressure in the middle cavity compared with the ear canal or the atmosphere) will cause the tympanic membrane to become retracted (pulled inward toward the middle ear space). If the negative pressure condition persists, otitis media with concomitant hearing loss may develop. Depending on the change in MEP, a tympanic membrane perforation also may occur.
Pathologically abnormal negative MEP at sea level is ∼−150 daPa or greater negativity on a tympanogram (Fig. 1C), which may be indicative of Eustachian tube dysfunction or a preotitis media condition (otitis media may manifest as a flat tympanogram curve [Fig. 1D]). The boys in the current study showed significantly greater negative MEP than the girls. A previous study (Haapaniemi, 1996) also showed a tendency of boys to have a greater negative pressure range than girls. The overall normal MEP results for the children in the present study suggest that altitudes as high as about 4000 m have no unequivocal effects on MEP. The MEP findings further suggest that children residing at these high altitudes have no greater risk for Eustachian tube dysfunction than children residing at sea level.
The TMC was similar for all groups, and both altitude groups had clinically normal TMC when compared with sea-level normative data. However, the TMC or acoustic admittance at the tympanic membrane increased with age for the Altitude II Group. This age effect has been reported in sea-level studies, and it is believed to be related to anatomical and physiological developmental effects (Haapaniemi, 1996; De Chicchis, et al., 2000). It is not clear why the Altitude I Group did not show an association between TMC and age. Further investigation is needed to determine whether the TMC/age relationship for the Altitude II Group is a persistent effect related to high altitudes of ∼4000 m and above. The TMC is not only a reflection of the mobility of the tympanic membrane but also an indication of the compliance of the middle ear system, thus yielding diagnostic information about the pathophysiology of the middle ear. A TMC value higher than 1.5 cm3 may be indicative of a hypermobile tympanic membrane, such as occurs in atrophic scarring of the tympanic membrane, or it may suggest ossicular chain disarticulation (separation of the three middle ear bones). Conversely, a TMC value lower than 0.2 cm3 may be an indication of impacted cerumen, a hypomobile tympanic membrane, or middle ear disorders, such as otitis media and otosclerosis (a pathological immobilization of the third bone [stapes] of the ossicular chain). The tympanogram in Figure 1D depicts an abnormally low-compliant tympanic membrane/middle ear system, which in this participant's case was indicative of otitis media. Overall, the TMC results show that altitudes as high as ∼4000 m have no significant effects on the compliance or admittance of the tympanic membrane and the middle ear system in high-altitude native children. The results further show no pervasive pathophysiology, as reflected in the TMC values.
The ECV was significantly higher in the Altitude II Group than the Altitude I Group and the Sea Level Group, possibly demonstrating an effect of a 4000-m elevation on ECV. The 2850-m elevation did not have a significant effect on ECV compared with the Sea Level Reference Group. The boys in the Altitude I Group showed a larger ECV than the girls, but the ECV for the boys and the girls in the Altitude II Group did not differ significantly. This may be related to the participants in the Altitude I Group being somewhat more heterogeneous than the children in the Altitude II Group. That is, the participants in the Altitude I Group consisted of children of indigenous Quechua Indian ethnicity and mixed Spanish/indigenous Indian backgrounds, whereas the Altitude II Group mainly comprised children of an indigenous Quechua Indian background. This difference in participants' ethnicity for the Altitude I Group may have yielded larger differences in ear canal sizes between boys and girls. The increase in ECV with age for both high-altitude groups is consistent with previous results on sea-level participants (Haapaniemi, 1996; Shanks and Shohet, 2009), and it is a reflection of the developmental increase in the size of the ear canal. Similar to MEP and TMC, ECV has diagnostic implications. For children in the age range of the current study, ECV values above 1.5 cm3 would be indicative of an abnormally large ECV at sea level, and coupled with a flat tympanometric curve would suggest a perforation of the tympanic membrane. Further, in a child with a history of otitis media who is treated with the insertion of tympanostomy tubes in the tympanic membrane for ventilation of the middle ear cavity, a larger than normal ECV is medically informative in that it indicates to the clinician that the tympanostomy tubes are patent and are not plugged up by fluid or other ear debris.
Because of a paucity of high-altitude research and clinical studies in otolaryngology and audiology, the effects of high altitude on the middle ear and inner ear among children who have lived all their lives at high altitudes and who have adapted to low-oxygen environments are not fully understood. Chronic mountain sickness, or a loss of adaptation to altitude, which has been referred to as a “common maladaptation” of high-altitude living, occurs in some native high-altitude dwellers, especially in adults, living above 2500 m in the Andes. Chronic mountain sickness is associated with elevated red blood cell count (polycythemia or excessive erythrocytosis) and neurological symptoms, including headache, memory changes, tinnitus, and dizziness (Leon-Velarde, et al., 2005; West, 2012; Vyas, et al., 2015; Villafuerte and Corante, 2016). It is estimated that 30 million people in South America who reside above 2500 m are at risk for chronic mountain sickness (Vyas, et al., 2015). Although the symptoms of tinnitus and dizziness may suggest auditory pathology, it is unclear, however, whether Eustachian tube dysfunction, middle ear and inner ear disorders are more prevalent in native highlanders. Other than excessive/impacted cerumen, the children in the current study did not appear to show a higher incidence of ear canal or middle ear pathology. Judging by the normal pure-tone thresholds in most of the children, inner disorders also were not apparent.
The measured tympanometry results at the high altitudes may be affected by the high-altitude environment, regardless of the pathologic condition of the ear canal or middle ear system. As previously mentioned, tympanometry is based on measurement of the acoustic immittance/impedance of the ear, which determines how much energy of a probe tone is transmitted from the ear canal to the tympanic membrane, and/or how much of the probe tone energy is reflected back from the tympanic membrane, indicating the pathophysiological status of the tympanic membrane and the middle ear system. To record changes in the immittance/impedance of the ear, the probe is hermetically sealed at the entrance to the ear canal. Therefore, between the probe and the tympanic membrane is an enclosed volume of air, and this enclosed volume of air varies with altitude or elevation due to the changes in the density of the air molecules. That is, the acoustic immittance/impedance of the enclosed volume of air is inversely associated with altitude (Lilly and Shanks, 1981). This would be expected to have more of an effect on the ECV than the other tympanometry results.
Using the formula P = antilog10 [(53,012.2—h)/18,401.8], where P = atmospheric pressure in mm Hg, and h = elevation above sea level in meters (Lilly and Shanks, 1981), the authors calculated the atmospheric pressure at 2850 m to be 532.03 mm Hg and at 3973 m to be 462.29 mm Hg. The atmospheric pressure for the Sea Level Group (elevation of ∼20 m) was 758.10 mm Hg. As the atmospheric pressure decreases, the ECV is expected to increase. The ECV for the Altitude II Group increased significantly when the atmospheric pressure decreased over a range of 295.81 mm Hg from 758.10 mm Hg (sea level) to a pressure of 462.29 mm Hg (Altitude II). However, there was no significant increase in ECV when the barometric pressure was decreased over a smaller range of 226.07 mm Hg from 758.10 (sea level) to 532.03 mm Hg (Altitude I).
In conclusion, the tympanometry and otological findings of the current study did not reveal a high incidence of middle ear pathophysiology in Andean children living at altitudes close to 4000 m. These findings suggest that children adapted to living in high-altitude, low-oxygen environments may not be any more susceptible to middle ear pathology than children living at sea level. Since there is some indication in the scientific and clinical literature that auditory disorders may be more apparent at altitudes higher than 4000 m, further auditory studies are needed of highlanders who reside at higher altitudes. In addition, middle ear pathophysiology studies should be conducted on highlanders who travel from their native high altitude to even higher elevations in the course of their daily living activities.
Footnotes
Acknowledgments
The authors are grateful to Universidad San Francisco de Quito Colegio Ciencias de la Salud, Escuela de Medicina in Quito, Ecuador, for continued support of this collaborative project. They thank Dr. Gonzalo Mantilla, Dean of the College of Health Sciences and Professor of Medicine, Universidad San Francisco de Quito, for ongoing support and advice. The authors are grateful to the David Rockefeller Center for Latin American Studies at Harvard University and its Director, Dr. Brian D. Farrell for support of this project. They express their gratitude to Dr. Jeremy Bloxham, Dean of Science at Harvard University; Harvard Biological Laboratories; and Harvard University Health Services for support.
Author Disclosure Statement
The authors declare no conflict of interest.