
Abstract
Abstract
We examined the pulmonary ultrastructure in tissue from two patients with high-altitude pulmonary edema (HAPE) by electron microscopy. In one case, we found that neutrophils were trapped in pulmonary capillary lumen of alveolar–capillary wall and part of the cytoplasm of a neutrophil protruded and adhered to the capillary endothelium. There were several degranulated vacuoles in the cytoplasm of the neutrophil. The pulmonary capillary wall was deformed, thickened, and swollen and there was evidence of degeneration. In another case, infiltration of neutrophils and macrophages, proliferation of type II pneumocytes, and numerous red blood cells were also observed in alveolar air space. These electron microscopic ultrastructural observations illustrate for the first time damage to the pulmonary alveolar–capillary barrier in lung tissue of humans with advanced HAPE.
Introduction
H
Case Description
The current study was approved by the Ethics Committee of the Shinshu University School of Medicine. Written informed consent for bronchoscopy and lung tissue biopsy was obtained from both patients.
Case 1
A 67-year-old man arrived and camped at the foot (600 m) of the Japan Alps in the summer season. He coughed while climbing up to 3000 m the next day. His cough worsened with the development of pink sputum while trekking higher to 3180 m. Symptoms of fatigue, anorexia, sleep difficulty, dyspnea, and cyanosis soon followed. He was rescued by helicopter 3 days after beginning his ascent and admitted to our hospital at an altitude of 600 m. On admission, he was fully conscious. Cyanosis on the lips and extremities were observed. Coarse crackles were audible at the bases of both lungs. Chest X-ray and computed tomography (CT) examinations showed patchy infiltrative shadows in the lower fields of both lungs. Arterial blood gas analysis showed a partial pressure of oxygen (PaO2) of 42.9 Torr on ambient air. By right heart catheterization, the pulmonary artery pressure (PAP) was 40/23 mmHg (systolic/diastolic pressure) with mean PAP of 29 mmHg and pulmonary capillary wedge pressure (PCWP) was 12 mmHg. HAPE was diagnosed according to diagnostic criteria proposed at the 1991 International Hypoxia Symposium (Hackett and Oelz, 1992). Supplemental oxygen and bed rest were promptly provided. His symptoms and abnormal chest X-ray shadows completely resolved after 1 week of treatment with oxygen therapy and bed rest.
Case 2
A 49-year-old man arrived at the foot of the Japan Alps in the summer season. After climbing to 3180 m and staying overnight in a lodge at 3000 m, he developed symptoms of coughing, difficulty breathing, and cyanosis on the third day of his ascent. He was rescued by helicopter and admitted to our hospital on the next day. On admission, he was fully conscious. Cyanosis was presented on his lips and extremities. Coarse crackles were audible over both lungs. Chest X-ray and CT examinations showed a pattern of bilateral patchy alveolar filling indicative of pulmonary edema. The PaO2 was 35.6 Torr on ambient air. Under condition of oxygen supplementation, his PAP was 31/13 mmHg with mean PAP of 19 mmHg, and PCWP was 10 mmHg by right heart catheterization. He was diagnosed with HAPE as above and treated with supplemental oxygen and bed rest. The symptoms and abnormal lung shadows diminished with treatment of oxygen therapy and bed rest and he was fully recovered after 1 week.
Bronchoscopy
Flexible bronchoscopy was carried out on the second day of hospital admission in both cases after obtaining informed consent. In addition, bronchoscopy was repeated after 7 days of treatment in case 2 with his informed consent to observe lung structure in the recovery stage of HAPE. Bronchoalveolar lavage (BAL) was performed and the BAL fluid (BALF) was obtained for total cell count as well as multinucleated cells with May–Grunwald–Giemsa staining. Bacteriological examination was performed as our previous study (Kubo et al., 1998). Two to three lung tissue specimens were obtained from the lower lobe of edematous segments by transbronchial forceps biopsy. Specimens were then placed in 2.5% glutaraldehyde for fixation and then specifically prepared for electron microscopy. Experts in electron microscopy in the Pathology and Cytology Laboratories of Japan in Tokyo, blinded to the diagnosis of these patients, examined these specimens.
Results
Multinucleated cells in bronchoalveolar lavage fluid
Table 1 shows data regarding multinucleated cells in the BALF of the two patients and they are consistent with previous BALF findings in patients with HAPE (Schoene et al., 1988; Kubo et al., 1998). The number of total cells was elevated and included increased amounts of neutrophils in both patients (Table 1) indicative of increased pulmonary capillary permeability. In addition, total cell and neutrophil counts were greatly diminished after 7 days of treatment in the second lavage of case 2 (Table 1). Bacteriological cultures of the BALF were negative in both of the patients.
Data were obtained after 7 days of treatment in the second time of bronchoscopy. A second bronchoscopy in Case 1 was not performed.
Electron microscopy observation
We obtained 29 electron micrographs of different magnification of the lung tissue in case 1 and 20 in case 2. The most typical cellular findings were the presence of infiltrated neutrophils as well as the numerous red cells, macrophages, and proliferation of type II pneumocytes in the alveolar air space. The noteworthy findings by electron microscopy were that of a neutrophil trapped in the capillary lumen with a part of its cytoplasm protruding and adherent to the basement membrane of the capillary endothelium (Fig. 1, case 1). There were several degranulated vacuoles in the cytoplasm of this neutrophil. The wall of this pulmonary capillary was deformed, thickened, and swollen (Fig. 1, case 1). Figure 2 shows a slightly thickened alveolar–capillary barrier at the ultrastructural level in the lung tissue of case 2. A type II pneumocyte with numerous mature lamellar bodies is observed in the alveolar space (Fig. 2). Figure 3 shows a neutrophil infiltrating in the pulmonary parenchyma (Fig. 3, left) and numerous red blood cells in the alveolar space in case 2 (Fig. 3, right); the latter indicating disruption of the alveolar–capillary barrier.
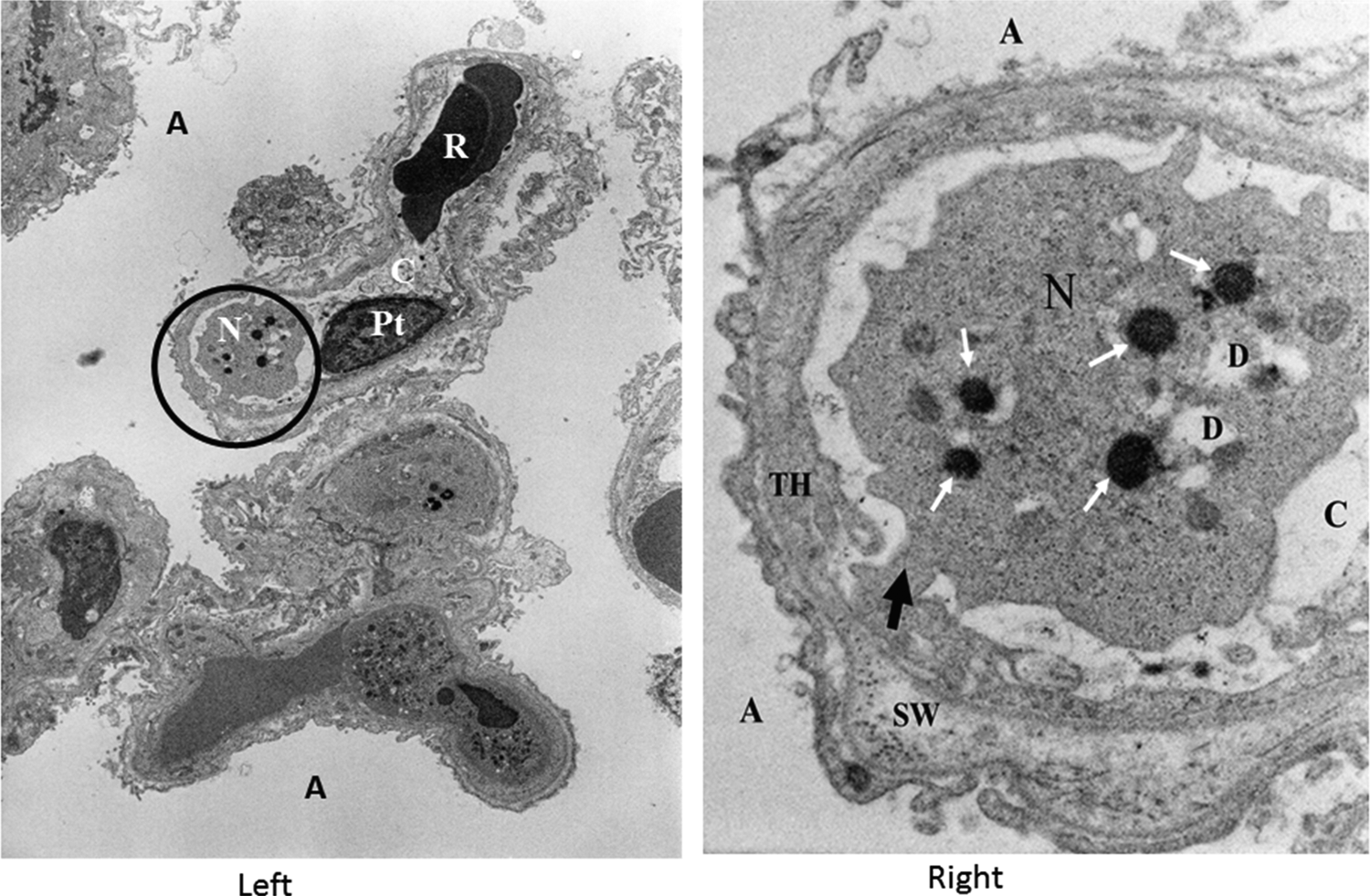
Electron micrograph showing a neutrophil in a pulmonary capillary lumen in case 1 of high-altitude pulmonary edema (HAPE). Left: A neutrophil (N), a red blood cell (R), and a platelet (Pt) were observed in the pulmonary capillary lumen (C). The part marked with black circle was further magnified and presented in the right figure. Magnification × 4500. Right: A neutrophil (N) was trapped and a part of the cytoplasm of the neutrophil protruded and adhered to the basement membrane of the capillary endothelium (black arrow). There were several degranulated vacuoles (D) in the cytoplasm of the neutrophil. The endothelial layer was swollen (SW) and thickened (TH). Magnification × 23,000. A, alveolar space; C, pulmonary capillary lumen; White arrows, segments of the nucleus.
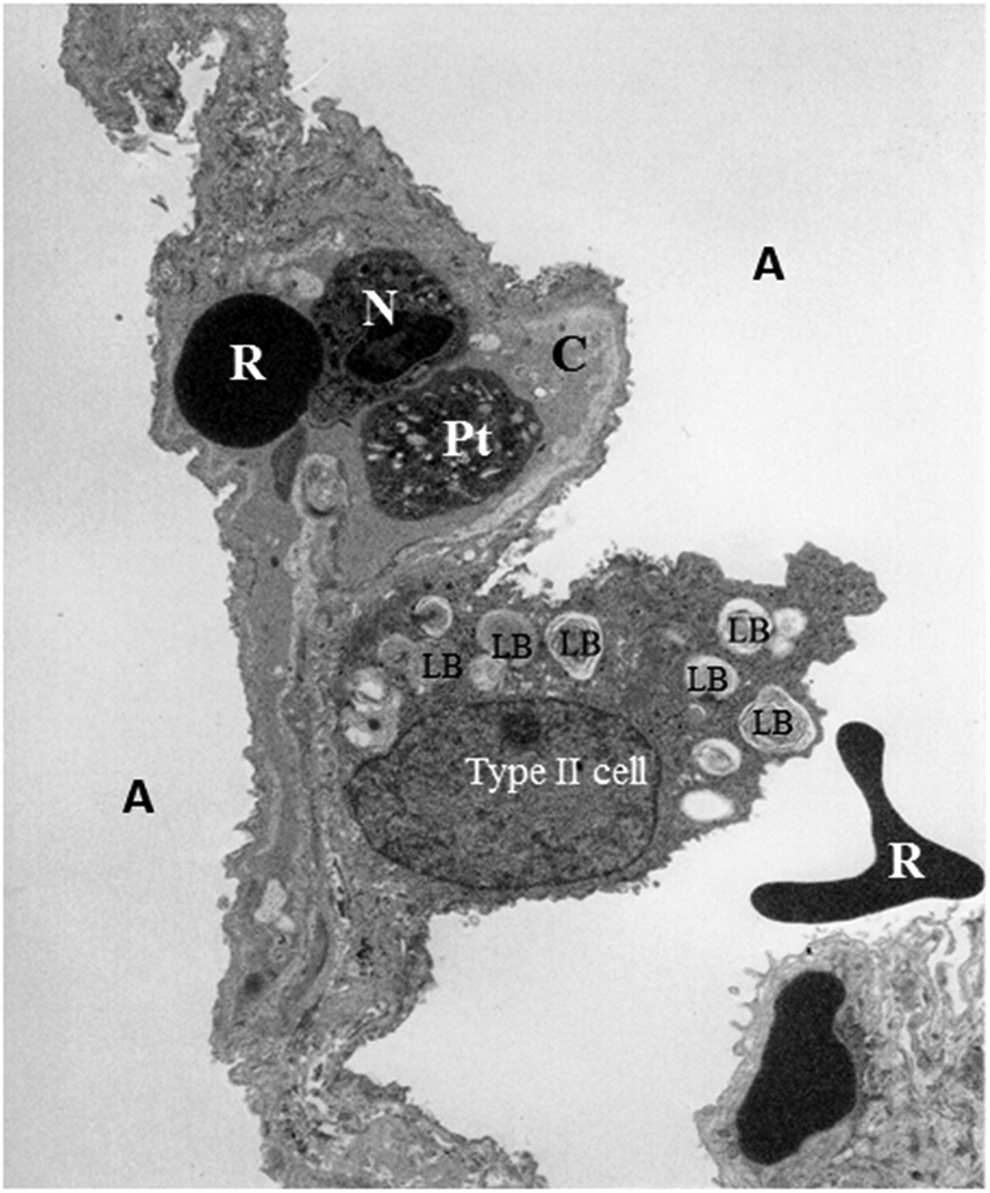
Electron micrograph showing the typical ultrastructure of the alveolar–capillary barrier in case 2. A neutrophil (N), a red blood cell (R), and a platelet (Pt) were observed in the pulmonary capillary lumen (C). The capillary wall was slightly thickened. A type II pneumocyte (Type II cell) with numerous mature lamellar bodies (LB) was observed in the alveolar space, explaining the proliferation of type II pneumocytes for the rapid recovery of HAPE. A red blood cell (R) was observed in the alveolar space, indicating disruption of the alveolar–capillary barrier. Magnification × 4600. A, alveolar space.
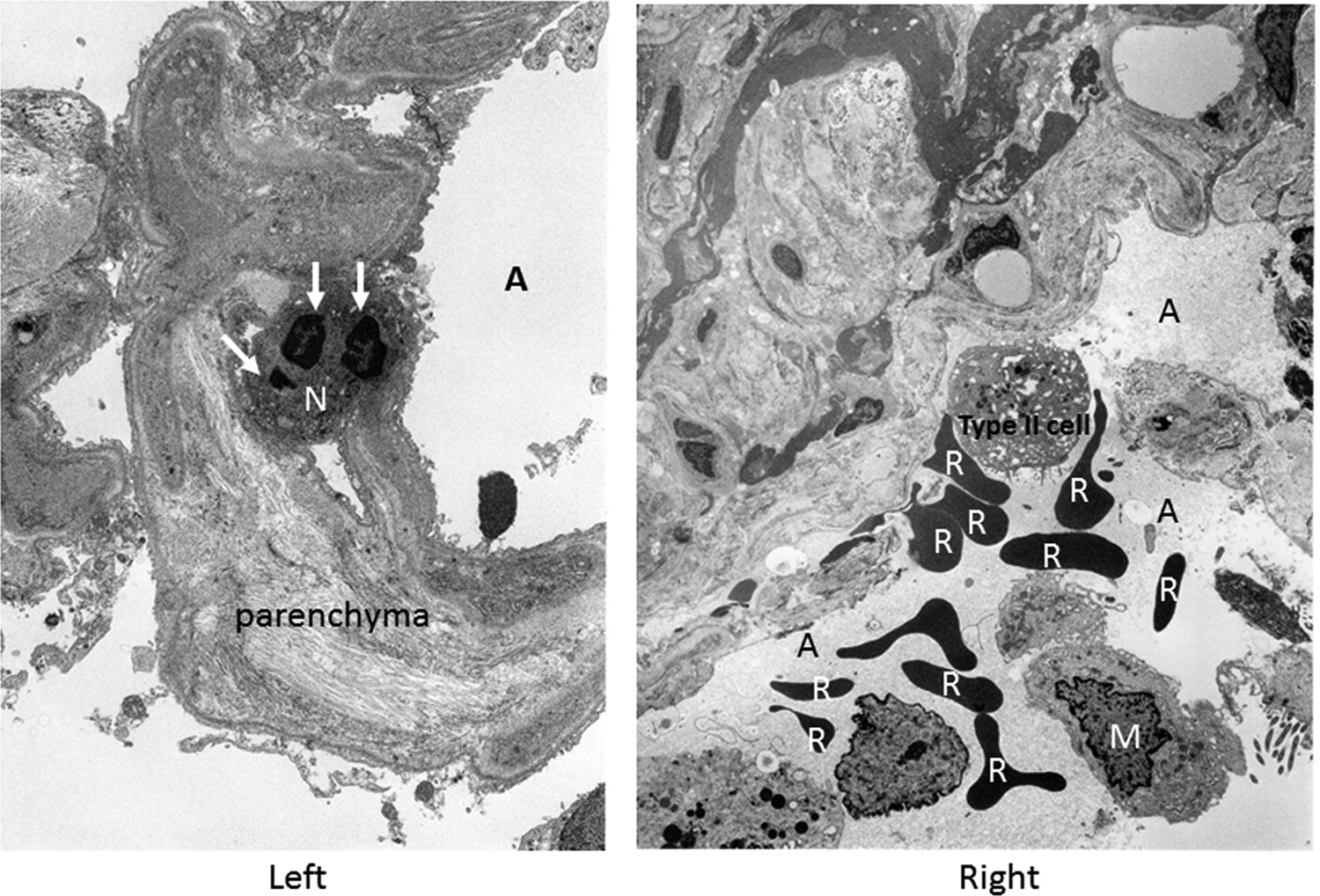
Electron micrograph showing a neutrophil (N) infiltrating in the pulmonary parenchyma (Left, white arrows: segments of the nucleus; magnification × 4500) and several red blood cells (R) in the alveolar space in case 2 (Right, M: macrophage; magnification × 3240). A, alveolar space.
Discussion
Our electron microscopy findings in two cases of advanced HAPE (4–5 days after the onset of HAPE) demonstrate that the ultrastructure of pulmonary alveolar–capillary wall can was impaired in HAPE patients as evidenced by deformation and thickening of the pulmonary endothelium, infiltration of neutrophils into the pulmonary parenchyma, and red blood cells in the alveolar space.
This is a novel pathological observation by electron microscopy of the ultrastructure of human lung tissue in patients with HAPE showing evidence of impairment of the pulmonary alveolar–capillary barrier. This is the first direct evidence of capillary stress failure in humans caused by hypoxia-induced pulmonary vasoconstriction. Previous electron microscopy studies in rat models of HAPE (West et al., 1995; Bai et al., 2010) support this supposition in demonstrating disruption of capillary endothelial layer, swelling of alveolar epithelial layer, and red blood cells in alveolar spaces. All these changes suggest a role of stress failure of pulmonary capillaries in advanced HAPE of several days duration.
The increased total cell count with large numbers of neutrophils in the BALF of two patients with HAPE (Table 1) indicates increased pulmonary capillary permeability at the moment of tissue sampling. The increased multinucleated cells in the BALF of these two patients could be explained as the consequence of stress failure in pulmonary capillaries caused by hypoxia-induced pulmonary vasoconstriction. It is likely that the highly exposed basement membrane of the damaged pulmonary capillaries undergoing stress failure can attract neutrophils that become activated and degranulated to cause further destruction of the alveolar–capillary barrier. The supporting cellular evidence by electron microscopy is that the exposed basement membrane of the damaged pulmonary capillaries also attracts platelets in the HAPE-like model of Sprague Dawley rats (West et al., 1995; Bai et al., 2010).
The major limitations of this small study are that the data analysis was not quantified and that the control lung tissue was not obtained. The highest level of quantitative data analysis of electron microscopy requires specific sample preparation with sophisticated techniques. And the control lung specimens require subjects in similar age, smoking history, and underlying lung disease, and in the case of HAPE, samples obtained from subjects without pulmonary edema after equivalent altitude exposure and duration. Nevertheless, our present electron microscopic observations on human pulmonary ultrastructure in advanced HAPE are novel and add to our knowledge of the pathophysiology of HAPE in humans.
Using electron microscopy, we can observe a small portion of the lung ultrastructure in HAPE at an incredible level of cellular detail. We identified features of several typical cells in the lungs of HAPE patients, which heretofore have not been seen in the lavage fluid from patients with HAPE. It is expected that these novel electron microscopy observations of the human pulmonary ultrastructure in subjects with HAPE may contribute to a deeper understanding of its pathophysiology.
Footnotes
Author Disclosure Statement
No competing financial interests exist.