
Abstract
Abstract
Bhandari, Sanjeeb Sudarshan, Pranawa Koirala, Nirajan Regmi, and Sushil Pant. Retinal hemorrhage in a high-altitude aid post volunteer doctor: a case report. High Alt Med Biol. 18: 285–287, 2017.—High-altitude retinal hemorrhages (HARHs) are seen at altitudes more than 3000 m, are usually multiple, flame shaped, and adjacent to blood vessels. Development near the macula causes blurring of vision, otherwise, they are symptomless and self-limiting. They often develop during the first few days after ascent to high altitude and subjects often suffer from acute mountain sickness (AMS) or high-altitude cerebral edema (HACE). People going to high altitude for the first time are more susceptible to retinal hemorrhages than experienced climbers and high-altitude dwellers. We present a case of a 31-year-old male doctor who developed sudden unilateral blurring of vision without any other symptoms after 6 weeks of volunteering at a high-altitude aid post in Nepal. There were no features suggestive of AMS or HACE. All examinations were normal except for fundoscopic examination in the left eye, which determined macular retinal hemorrhage. Although he was reluctant to descend, he was counseled to descend and refrained from further ascent to higher altitude, which could accentuate hypoxemia and any strenuous activities that increase intraocular pressure. He recovered his vision after few weeks in Kathmandu and his retinal hemorrhages regressed. Hypoxia exacerbated by repeated bouts of rapid ascent to further higher altitudes may have contributed to his HARH. This suggests that unilateral retinal hemorrhages can develop even after several weeks at high altitude without concomitant AMS or HACE. People going to high altitude are reluctant to retreat, before reaching their target, when they suffer from HARH. The same is shown by a physician. So it is very important for healthcare professionals working at high altitudes especially in the Himalayas of Nepal to have a good knowledge about HARH and its proper treatment.
Introduction
T
High-altitude illnesses have three clinical entities: acute mountain sickness (AMS), high-altitude pulmonary edema (HAPE), and high-altitude cerebral edema (HACE) (Houston, 1976).
High-altitude retinal hemorrhage was first reported by Frayser et al. (1970). Since then it has been reported many times, and studied in various high-altitude travelers such as soldiers and climbers (Rennie and Morrissey, 1975; MacLaren, 1995).
High-altitude retinopathy (HAR) was classified by Wiedman (1983). The ophthalmoscopic findings of HAR are dilated retinal veins and arteries, diffuse or punctate preretinal hemorrhages (located peripherally and sometimes in the macula), vitreous hemorrhages, papillary hemorrhages, peripapillary hyperemia, and papilledema (Wiedman, 1975).
Many individuals who ascend to heights more than 3000 m develop HAR (McFadden et al., 1981; Barthelmes et al., 2011). High-altitude retinal hemorrhages (HARHs) form part of the cluster of signs of HAR (Morris et al., 2006). These hemorrhages are almost always symptomless and self-limiting. They are usually multiple, often flame shaped, and adjacent to blood vessels. If they develop near the macula, then patients may present with the complaint of blurred vision.
These hemorrhages are mostly seen during the first few days after ascent to high altitude (Rennie et al., 1975), and the subjects are often observed to be suffering from AMS or HACE. People going to high altitude for the first time are more likely to have retinal hemorrhages than experienced climbers and high-altitude residents (Clarke and Duff, 1976). We report a case of a 31-year-old male doctor who developed unilateral retinal hemorrhage after staying at high altitude for 6 weeks, volunteering at an aid post.
Case Report
A 31-year-old white male doctor, who was a sea-level resident, traveled to Nepal and trekked up the Khumbu Valley in the Everest Region. He followed the recommended ascent profile to trek to 4470 m to volunteer in an aid post for 3 months. During his stay, he went for several single-day excursions to the surrounding lakes and peaks situated at 4600 to 5100 m. He started hiking to higher altitudes 20 days after his stay at 4470 m. The last time he went for a hike was a day before the day of presentation and 6 weeks after staying at 4470 m. While preparing for the hike to one of the other lakes, he noticed change in his vision. On subsequent examination, he found out that vision in his left eye that was previously as good as his right eye was now worse. Ophthalmoscopy done by his fellow volunteer doctor found a retinal hemorrhage in his left eye, and he was recommended to descend down to Kathmandu. He was transferred by a helicopter to a travel medicine clinic in Kathmandu.
At the clinic, the patient denied any problems with breathing or coordination and did not have tingling, weakness, or numbness. He denied heavy lifting, straining, or a significant cough. But he admitted to traveling to higher altitudes and returning to his workstation a few times during his stay at 4470 m. He had no significant medical history or history of medication use. Physical examination revealed normal vitals with an oral temperature of 37.6°C, blood pressure of 128/82 mmHg, heart rate of 86/min, respiratory rate of 16 breaths/min, and oxygen saturation of 97% in room air.
On ophthalmological examination, his visual acuity was 20/20 in the right eye and “counting fingers” on the left. His right pupil reacted normally to light, whereas the left eye was still dilated because of mydriatics used by his colleague for the ophthalmoscopic examination. Direct ophthalmoscopy revealed a retinal hemorrhage in the left eye involving the macula (Fig. 1). The optic disks were normal but the retinal veins were engorged and dilated in both eyes (Figs. 1 and 2). Laboratory investigations including complete blood count, basic metabolic panel, and urinalysis were within normal limits. Ophthalmological consultation confirmed retinal hemorrhage most likely related to his travel to high altitude, and there were no other ocular abnormalities. Fundus photographs were taken that revealed grade 4 HARH. Magnetic resonance imaging of the skull showed no abnormalities in vessels supplying the orbit.
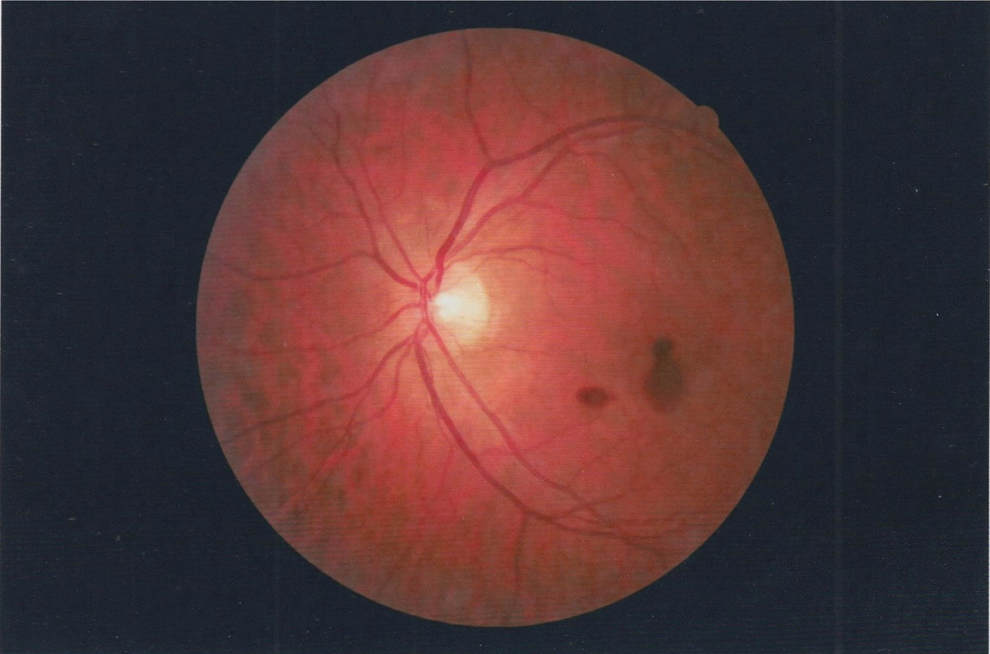
Left eye fundus photograph.
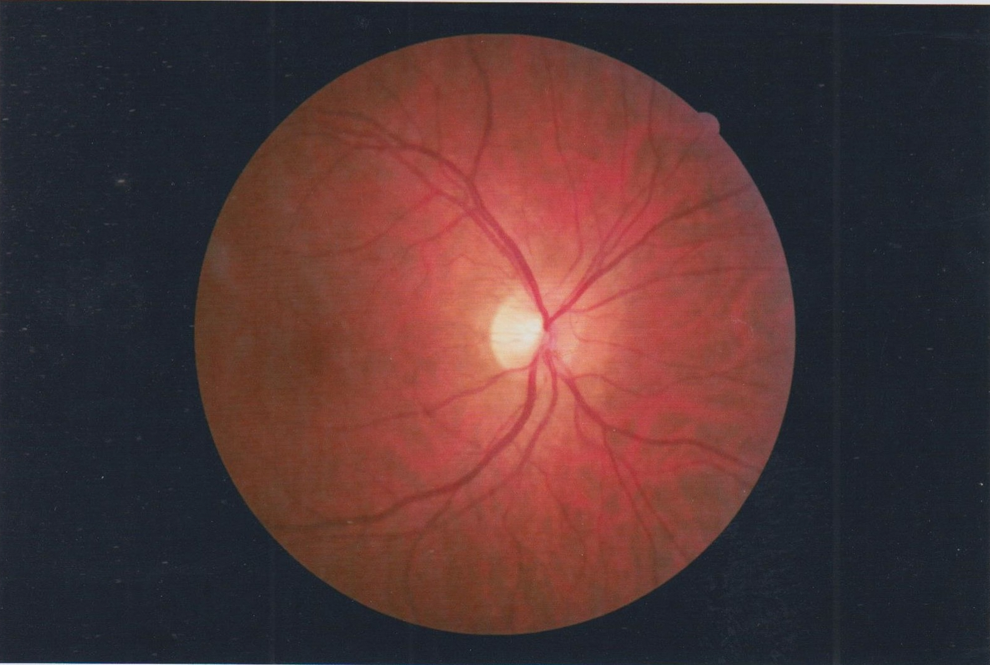
Right eye fundus photograph.
Discussion
This is the first reported case of HARH in an individual involved in healthcare activities in the Himalayas of Nepal. The grading of HAR uses findings of retinal vascular dilatation, hemorrhage, and ophthalmoscopic findings of vitreous hemorrhage and papilledema (Wiedman, 1983). The retinoscopic findings of HARH show hemorrhages in the superficial nerve fiber layer of the retina (Lubin et al., 1982; Wiedman and Tabin, 1999). In mild form, the hemorrhages involve peripheral retina and generally spare macula. As the condition progresses, macular hemorrhages producing scotoma may develop.
HARHs are likely induced by systemic hypoxic effects on the eye, despite regulatory adjustments by retinal circulation (Barthelmes et al., 2011). Hypoxia stimulates retinal vasodilatation and capillary proliferation, which leaves retinal vessels vulnerable to a sudden rise in intravascular pressure during a cough, straining, or strenuous activities. Retinal vasodilatation has been seen in both acute and chronic exposure to hypoxia.
HARH occurrence is not demonstrated in chamber studies, which may be because of the relatively short time of altitude exposure in the setting (Sutton, 1983). Hypoxia has been suggested as the good predictor for HARH occurrence, rather than absolute altitude (Hackett and Roach, 2011). Thus, hypoxia exacerbated by repeated rapid ascent to further higher altitudes may have contributed to HARH in our patient. Our patient's long travels in shorter duration may have emulated vigorous activity for the duration he was traveling. It is not certain whether prolonged exposure to hypoxia at 4400 m or many short and vigorous insults at even higher altitude triggered the HARH seen in our patient. In addition, several case studies suggest the association of hemoconcentration at altitude and HARH (Lang and Kuba, 1997; Wiedman and Tabin, 1999).
HARH is closely associated with HAPE and HACE and is part of these high-altitude illnesses (Sutton, 1983; MacLaren, 1995). These hemorrhages are usually asymptomatic and resolve spontaneously within 1 to 2 weeks. The patient presents with symptoms of vision only when the macula is involved. Although it is generally believed that HARH is a benign condition, some have argued that at extreme elevations, it may be a reflection of a pathophysiological process similar to HACE in the brain. Correlation between HARH and HACE (Wiedman and Tabin, 1999) has been noted.
Most of the individuals with severe HACE have HARH, but the opposite has not always been observed. HARH may even occur in perfectly acclimatized humans after prolonged high-altitude hypoxia, independent of the clinical signs of high-altitude-related illnesses such as AMS or HACE, most likely because of hypoxia when reaching even higher altitudes.
Careful assessment of vision must be undertaken to determine the need for descent. Clinicians evaluating patients with acute vision problems at high altitude should test visual acuity and must perform fundoscopy to determine whether HARH is present regardless of their length of stay and level of awareness of the problem. Patients with macular involvement should be counseled to refrain from further ascent or activity that could accentuate hypoxemia or increase intraocular pressure until retinal hemorrhage resolves.
Groups of sojourners at high altitude, like mountaineers, are very reluctant to descend to lower altitudes when suffering from high-altitude illnesses. This is often because of the significant time, effort, and money that have been invested in the trip. It is paramount for healthcare professionals working at high altitude to have a good working knowledge about HARH, and should know about how to deal with and how to counsel patients. HARHs can be a debilitating problem at high altitude, and further work needs to be done to clearly define when it is safe to continue a trip in the setting of HARH, and when patients should descend.
Footnotes
Author Disclosure Statement
No competing financial interests exist.