
Abstract
Abstract
Bhandari, Sanjeeb Sudarshan, Pranawa Koirala, Sadichhya Lohani, Pratibha Phuyal, and Buddha Basnyat. Breathlessness at high altitude: first episode of bronchoconstriction in an otherwise healthy sojourner. High Alt Med Biol.. 18:179–181, 2017—High-altitude illness is a collective term for less severe acute mountain sickness and more severe high-altitude pulmonary edema (HAPE) and high-altitude cerebral edema, which we can experience while traveling to high altitude. These get better when we get down to the lower altitudes. People with many comorbidities also have been traveling to high altitudes from the dawn of civilization. Obstructive airway diseases can be confused with HAPE at high altitude. Asthma is one of those obstructive pulmonary diseases, but it is shown to get better with travel to the altitudes higher than the residing altitude. We present a case of 55-year-old nonsmoker, athletic, female, a lowland resident who developed difficulty breathing for the first time at high altitude. She did not get better with the descent to lower altitude and timely intake of acetazolamide. Her pulmonary function test showed obstructive airway pattern, which got better with salbutamol/ipratropium nebulization and oxygen.
Introduction
A
The Case
A 55-year-old nonsmoking female lowlander visited a travel medicine clinic in Kathmandu (1300 m) with complaints of difficulty breathing over the preceding 3 days. She was trekking in the Langtang region when her symptoms started. She began her trek from Syaphrubesi (1460 m) and reached Langtang village (3545 m) in 2 days. After resting there overnight, she ascended to Kyanjin Gompa (3800 m) on the fourth day. While at Kyanjin Gompa, she developed a cough and rhinorrhea and during her ascent to Kyanjin Ri (4770 m) the following day, she had the onset of headache and difficulty breathing when she reached an altitude of 4200 m. She also experienced dizziness and decreased appetite, but denied having any nausea or vomiting. She had chills but did not report feeling feverish. When self-medication with aspirin 500 mg and acetazolamide 250 mg did not relieve her symptoms, she descended to Langtang the next day without any improvement in her symptoms. The next day she went down to Lama Hotel (a village at 3541 m) and then to Thulo Syabru (2260 m). Although her headache and cough abated, her breathlessness continued to worsen despite further descent to 2260 m. The next day, she returned by vehicle to Kathmandu and upon arrival at the clinic, she was persistently breathless.
Her history was significant for no chronic illnesses, including asthma or allergies. Her medications included aspirin and ibuprofen, which she took during the trek. On examination on arrival, her blood pressure was 140/90 mmHg, pulse 74 beats/min, respiratory rate 22 breaths/min, temperature 37°, and oxygen saturation of 91% by pulse oximetry while breathing ambient air. There was no cyanosis. Wheezing was heard bilaterally on chest auscultation, but no crackles were appreciated. Spirometry revealed an obstructive airway pattern with a FEV1/FVC of 0.67 and a FEV1 of 1.55 (54% of predicted). Her ECG was normal and a chest radiograph (Fig. 1) showed only mild hyperinflation. Her complete blood count was normal.
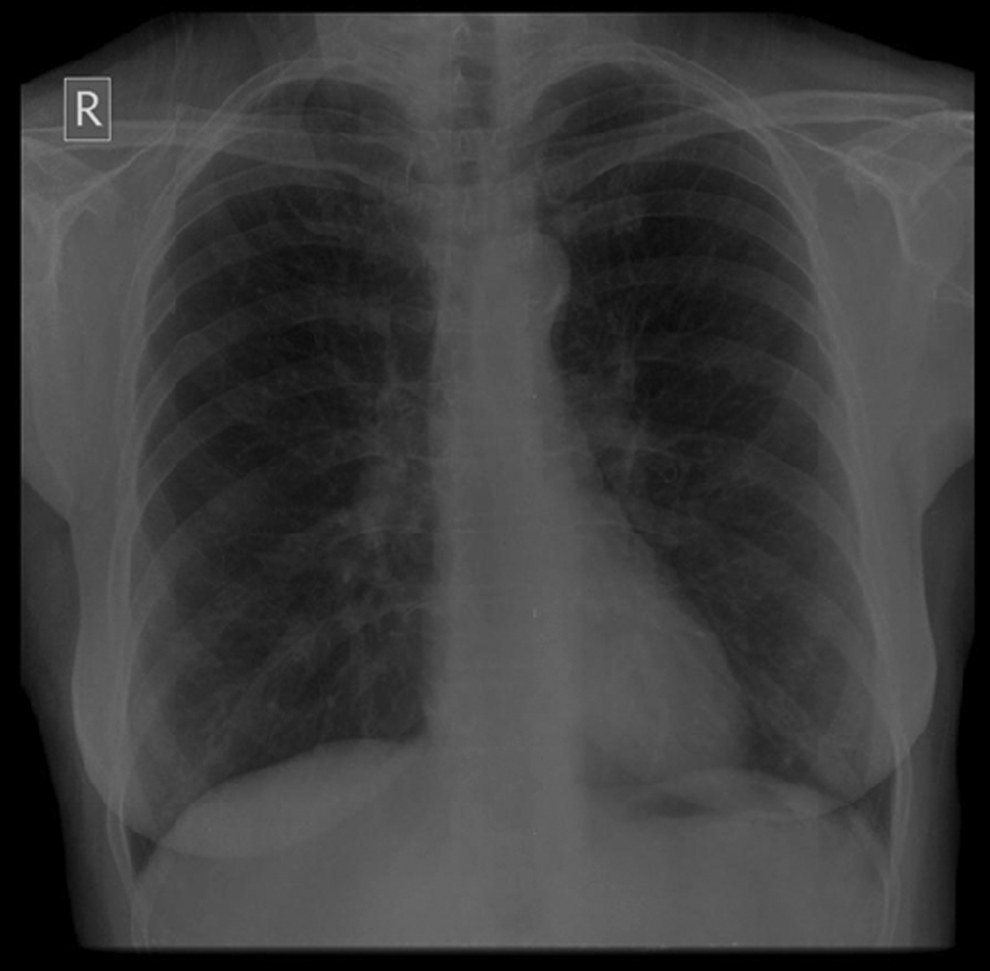
Chest radiograph at presentation.
With a diagnosis of diffuse bronchoconstriction of unknown cause and impaired exertion at high altitude, she was observed overnight. Her treatment included oxygen by nasal cannula at 2–3 L/min to maintain her oxygen saturation above 95%, nebulization of ipratropium/salbutamol, and 60 mg of oral prednisone. She was also given nifedipine 20 mg SR every 8 h so as to treat mild HAPE, despite the lack of any interstitial or alveolar edema on X-ray or improvement with her considerable descent.
She was reevaluated the next day, at which time her oxygen saturation was 94% on ambient air and BP was 130/80 mmHg. Chest auscultation revealed decreased wheezes on both lungs. Nifedipine was stopped. She was continued on prednisone 40 mg once a day for 7 days and salbutamol by metered dose inhaler was prescribed to be used as needed. On discharge, her oxygen saturation was 95% on ambient air. There were minimal wheezes bilaterally, which had markedly decreased compared to her initial presentation.
Discussion
As a rule, illness occurring at high altitude should be attributed to the altitude until proven otherwise (Rodway et al., 2003). The symptoms of headache, cough, and shortness of breath, which occurred in this case are in fact some of the typical symptoms of AMS with a component of HAPE. However, the patient's pulmonary symptoms did not improve with descent. Other differential diagnoses must be considered when taking recommended measures like descent and acetazolamide do not help as in our case. In addition, our patient had obstructive features on spirometry. An important limitation of this case presentation is that we did not obtain a postbronchodilator response on spirometry but with the improvement in her breathlessness and oxygen saturation following treatment, bronchodilation can be assumed to have occurred.
In some asthmatic individuals, aspirin can cause asthma or exacerbate bronchoconstriction (Szczeklik and Stevenson, 2003). Thus in this case, aspirin could have made her bronchoconstriction worse. It is also known that breathing cold dry air while doing exercise leads to bronchoconstriction and elevated residual volume in comparison to breathing warmer and more humid air (Strauss et al., 1977).
In conclusion, although it is generally believed that going to high altitude may improve asthmatic symptoms; this may be not true for everyone (Cogo and Fiorenzano, 2009). And as in our patient, high-altitude hypoxia and cold, perhaps along with the onset of an upper respiratory tract viral infection, may have triggered her bronchoconstriction and asthma-like symptoms. Bronchoconstriction and asthma may be important alternative diagnoses to consider in those suspected of having HAPE, so that proper treatment can be initiated and to avoid unnecessary medications such as nifedipine and other pulmonary vasodilators, which can worsen hypoxemia in asthma.
Footnotes
Author Disclosure Statement
No competing financial interests exist.