
Abstract
Abstract
Lanfranconi, Francesca, Luca Pollastri, Giovanni Corna, Manuela Bartesaghi, Massimiliano Novarina, Alessandra Ferri, and Giuseppe Andrea Miserocchi. The elusive path of brain tissue oxygenation and cerebral perfusion in harness hang syncope in mountain climbers. High Alt Med Biol. 18:363–371, 2017.
Aim:
Harness hang syncope (HHS) is a risk that specifically affects wide ranges of situations requiring safety harnesses in mountains. An irreversible orthostatic stasis could lead to death if a prompt rescue is not performed. We aimed at evaluating the risk of developing HHS and at identifying the characteristics related to the pathogenesis of HHS.
Results:
Forty adults (aged 39.1 [8.2] years) were enrolled in a suspension test lasting about 28.7 (11.4) minutes. We measured cardiovascular parameters, and near infrared spectroscopy (NIRS) was used to assess cerebral hypoxia by changes in the concentration of oxyhemoglobin (Δ[HbO2]) and de-oxyhemoglobin (Δ[HHb]). In the four participants who developed HHS: (1) systolic and diastolic blood pressure showed ample oscillations with a final abrupt drop (∼30 mmHg); (2) Δ[HbO2] increased after 8–12 minutes of suspension and reached a plateau before HHS; and (3) Δ[HHb] decreased with a final abrupt increase before syncope.
Conclusions:
Participants who developed HHS failed to activate cardiovascular reflexes that usually safeguard O2 availability to match the metabolic needs of the brain tissue. Since cerebral hypoxia was detected as an early phenomenon by Δ[HbO2] and Δ[HHb] changes, NIRS measurement appears to be the most important parameter to monitor the onset of HHS.
Introduction
W
There is a paucity of data regarding the true numbers of individuals potentially exposed to HHS, but this is a risk that specifically affects people of mountaineering and caving communities (Fig. 1A) as well as workers involved in high-altitude civil engineering. According to the reports of the Italian National Alpine and Speleological Rescue Organization, 3504 high mountain casualties were assessed from 1955 to 1985. The trend in high mountain casualties is increasing in Alpine regions and 18,658 victims were recorded from 1990 to 2009 (www.cnsas.org). Unfortunately, there is a cultural gap existing in professional debates regarding HHS as a patent risk for harness users, and as a matter of fact, no National or International registries are available to identify the incidence of HHS and there is only anecdotal evidence of death due to harness suspension.

Thus, the full HHS phenomenon appears underestimated and its fate is not entirely different in scientific papers where only a paucity of human experimental perspective studies have been conducted since the pioneering studies mentioned by the extensive review of Seddon (2002). In the past 15 years, only few studies have investigated or reviewed the tolerance of the human body to motionless suspension while wearing a full-body safety harness, and HHS has been definitely demonstrated as a possible final effect (Lee and Porter, 2007; Turner et al., 2008; Mortimer, 2011; Pasquier et al., 2011).
Included in the definition of syncope is the strong relationship between gravitational stress, vasomotor failure and/or bradycardia, reduced venous return, and fallen cardiac output (CO) with a definitive decrease in cerebral oxygenation before fainting (Moya et al., 2009; Schwartz et al., 2013). Due to the limited scientific literature available on HHS, it appears a remarkable issue to search whether there is an individual critical amount of cerebral and midbrain deoxygenation that eventually inhibits the cardiovascular reflexes when the syncopal event occurs. Accordingly, a global cerebral hypoperfusion due to failure in the cardiovascular reflexes response might be the underlying cause of HHS, leading to a mismatch between cerebral oxygen demand and supply.
The adaptations of the cardiovascular reflexes in HHS have to take into account additional factors, including environmental stressor (hypothermia, exertional stress) and microgravity stimulus. Different models of exposure to both real and simulate microgravity (i.e., space flights or 6° head-down model of bed rest confinement) have been shown to affect the cardiovascular function by inducing elevations in heart rate (HR) and reductions in stroke volume and CO (Convertino et al., 1994; Serrador et al., 2000). Incidence of syncope occurs regardless of whether the exposure to microgravity is prolonged or brief (Butler et al., 1991).
Examining metabolic impairments along the human O2 transport-utilization chain could provide important insights into the pathophysiology of the lethal multivisceral hypoxia that distinguishes HHS. In vivo, the evaluation of the dynamic balance between O2 delivery and O2 consumption, fulfilling the principle of mass conservation as defined by Fick equation, is possible by near infrared spectroscopy (NIRS). NIRS is a noninvasive method that gives the individual estimation of tissues fractional O2 extraction, that is, oxidative metabolism at rest or during exercise in healthy subjects and patients (Mancini, 1997; Ferrari et al., 2004; Grassi and Quaresima, 2016). Thus, NIRS appears an advantageous and not-invasive tool to investigate when cumulative cerebral hypoxia is no more sustainable by the central nervous system in syncopal events (Madsen et al., 1998; Karsten et al., 2000).
The purposes of this study were: (1) to verify the timing of cerebral hypoxia preceding the inappropriate control of cardiovascular reflexes in HHS; (2) to investigate whether specific characteristics related to suspension (brief and real exposure to microgravity) need to be taken into account in the pathogenesis of HHS.
Methods
Participants
The study conformed to the standards set by the latest revision of the Declaration of Helsinki, and all procedures were approved by the ethics committee of the University of Milano-Bicocca. Personal data were treated according to standard principles of confidentiality. Participants were informed about the risks of developing HHS and the ability of the medical team to manage the possible occurrence. All participants were provided and signed an informed consent to be part of the project.
Forty adults participated in this study (mean [SD]: age 39.1 [8.2] years; body mass index 24.2 [3.03]; 85% men, 15% women). Participants included people who had never experienced the use of a harness, as well as professional and/or habitual users of a harness. The latter were recruited from different backgrounds in the Italian northern mountain area: Alpine guides, high-altitude civil engineering workers, mountain rescuers, and climbing community members. All participants underwent a medical check, including a careful collection of clinical history, a complete physical examination, and a cardiopulmonary exercise test (CPET). There were no exclusions on medical grounds for respiratory, cardiovascular, skeletal muscle, or neurological diseases.
Exercise and suspension protocol
Each participant underwent an incremental exercise on a treadmill (Pulsar: h/p/Cosmos, Dusseldorf, Germany) a week before the motionless suspension tests (ST). All the CPET and ST were conducted under medical supervision: HR was continuously monitored by 12-lead electrocardiography (Quark C12x: Cosmed, Roma, Italy), such as arterial blood O2 saturation (SaO2) recorded via pulse oximetry at the finger (RAD 9 Signal Extraction Pulse Oximeter: Masimo Corporation, Irvine, CA). A careful assessment while the participants were in a resting condition was carried out before the CPET by measuring HR, pulmonary ventilation (in body temperature and pressure, saturated), and observation of the participant. O2 uptake
The same cardiopulmonary variables were measured on a different day, after 4–6 minutes in a resting condition, when each participant underwent an ST, hanging from a chest ring attachment raised about 50 cm from the floor (Fig. 1B). Participants wore a full body harness with ergonomic back padding and leg-loops with quick-release buckles (Golden Top Evo Alu, CAMP, Premana, Italy). The harness fit was evaluated at rest after checking the position of the shoulder straps, chest and hip rings. Participants were allowed to voluntarily control trunk posture, but they were not permitted to move their limbs. In a previous experimental set, this posture guaranteed that small torso adjustments were not enough to generate signals of cerebral perfusion/oxygenation monitored by cerebral NIRS. Circumferences were measured at the medium third of the thigh and at the middle of the calf, using a measuring tape on a previously marked region of the limb before and after ST, to evaluate blood pooling signs, such as increased inferior limb diameters due to orthostasis.
The ST time was recorded from the start of a motionless hanging condition (reached within 10–20 seconds after hanging at rest) until the time the participant returned to the ground. Blood pressure (BP) was measured every 4 minutes or less if initial signs of orthostatic intolerance were recorded, that is, when abruptly modification of HR was monitored on the ECG or symptoms of discomfort were reported. As syncope often occurs without warning (Moya et al., 2009), we ended the ST when at least one of the following signs was detected: (a) decrease of systolic BP (SBP) by more than 20 mmHg relative to the resting value; (b) decrease of diastolic BP (DBP) by more than 10 mmHg relative to the resting value; (c) development of systolic hypertension (above grade 2, >160 mmHg); (d) development of diastolic hypertension (above grade 2, >100 mmHg); (e) an increase in HR by more than 25 bpm above the baseline value; (f) extreme subjective discomfort causing voluntary termination; and (g) uncontrollable systemic signs such as full-body light-headedness, nausea, sweating, trembling, or severe headache. Participants who developed syncope were kept in a supine position by passive raising of both legs above cardiac level (Bridges and Jarquin-Valdivia, 2005; Geerts et al., 2012; Debaty et al., 2015). All the other participants were placed in supine position within 30 seconds from termination of the ST, with full flexion of the hips and knees until recovery of HR, SBP, and DBP to baseline values (Kweon et al., 2012). No time limit was previously set. In the case of syncope, the end time was considered when the unconscious participant lay down on the examination table.
Environment-laboratory ambient conditions were assessed during the exercise test and ST, assuring that laboratory conditions were stable during the performance of testing and data collection: Ambient temperature and relative humidity measurements were made with a thermocouple and a hygrometer, respectively. Testing was performed if temperature and humidity measurements were in the range of 23°C ± 5°C and <70%, respectively.
NIRS technique
Cerebral and skeletal muscle oxygenation were continuously monitored during CPET and ST. NIRS is a noninvasive method that allows for the monitoring of tissue oxygenation by using the principle that the near-infrared (NIR) light absorption characteristics of hemoglobin (Hb) and myoglobin depend on their O2 saturation at different wavelengths (780 and 850 nm, respectively). Technical and physical details of NIRS have been described elsewhere (Lanfranconi et al., 2006, 2014; Grassi et al., 2007; Porcelli et al., 2010).
In summary, light in the NIR spectrum readily penetrates skin, fat, and bone and is differentially absorbed by heme-containing molecules in underlying tissues, predominantly oxyhemoglobin (Δ[HbO2]) and de-oxyhemoglobin (Δ[HHb]). A modified form of the Beer-Lambert law quantifies changes in Δ[HbO2] and Δ[HHb] concentrations over time to reflect the oxygenation in the illuminated area. The Beer-Lambert law was used to calculate micromolar (μM) changes in tissue oxygenation; variation of absolute values relative to baseline were considered as changes in the concentration of Δ[HbO2] and Δ[HHb]. A decrease in Δ[O2Hb] and increases in Δ[HHb] were interpreted as evidence of an unbalance between delivery and extraction relative to the tissues under study. A two-channel continuous wave NIRS was used to detect skeletal muscle and brain oxygenation (Nimo: Nirox, Brescia, Italy). This system is not equipped to measure blood flow. The data Δ[HbO2] and Δ[HHb] were acquired at 2 Hz. During the data collection procedure, concentration changes were displayed in real time, and the signal quality and the absence of movement artifacts were verified.
The skeletal muscle NIRS probe was positioned on the distal end of the dominant thigh to monitor oxygenation changes in the vastus lateralis. The probe was composed by an optical fiber bundle (length: 3.15 m; diameter: 4.50 mm) that was utilized to carry out the light to the muscle, whereas one optical fiber bundle of the same size was utilized to collect the light emerging from the same tissue. The probe was firmly placed on the skin (∼10 cm above the proximal border of patella and 3 cm lateral to the midline of the thigh) and secured with a small belt of Velcro straps. The detector–illuminator distance was set at 3.5 cm. Elastic bandages were put around the probe to prevent contamination from localized light. Pen-marks were made over the skin to indicate the margins of the plastic spacer to check for any downward sliding of the probe during treadmill walking or ST. Once secured in place, no sliding of the probe was detected for any of the tests.
Skinfold thickness at the site of application of the muscle NIRS probe was determined before the exercise protocol by a calliper (C10 Plicometer Tanner–Whitehouse; Holtain, Ltd., Crymych, United Kingdom), and the measured average values of skin and subcutaneous thigh tissue thickness were 10.1 (2.9) mm (range 4.4–26.6). After the exercise, a wider cuff (tourniquet) was placed on the proximal part of the thigh, inflating at 250–350 mmHg (depending on the participant's body mass index), to induce ischemia and estimate the maximal de-oxygenation, when a plateau was reached for the increase in Δ[HHb] and a related decrease in Δ[O2Hb]. Ischemia was obtained while individuals were sitting on the examination table.
For frontal cortex oxygenation, a different probe was used and positioned on the left side of the forehead in the frontal region (one optode close to the midline and one ∼5 cm laterally, avoiding the temporal region, and as close as possible to the hairline). The optodes were spaced in accordance with adequate light detection (4.8 cm) to avoid the relative contribution of skin blood flow to signals from cerebral tissue (Owen-Reece et al., 1996). The probe holder was fixed over the head by a fastener, adapted to the individual head's size and shape. We checked for a stable optical contact with the scalp for the optodes, which was also verified at the end of the protocol. Elastic bandages were put around the probe to prevent contamination from environmental light. The pressure created by the fastener was adequate to induce a partial transient blockage of the skin circulation during the NIRS study.
Statistical analysis
Values were expressed as mean (SD). Sample size calculation determined that a sample of 34 participants would be adequate to detect a difference of 6 minutes in suspension time between them, with a power of 0.80 (α = 0.05). D'Agostino and Pearson omnibus normality test was used to check whether values follow a Gaussian distribution. The statistical significance of the difference between mean values was evaluated by a two-way analysis of variance. A Sidak multiple-comparison test for grouped data was applied. Regression and correlation analyses were performed by using the least-squared residuals method. The level of significance was set at p < 0.05. All statistical analyses were performed by using a commercially available software package (Prism 6.0: GraphPad, La Jolla, CA).
Results
Cardiopulmonary parameters during ST
A posteriori participants were divided into three groups, based on the cardiovascular events during ST, identified as SYN, OVER, and NORM, and are summarized in Table 1. As shown in Table 1, in OVER (n = 8), a large increase of SBP (greater than 30 mmHg relative to baseline) was reached after 8–12 minutes, and ST was terminated (26.5 [18.4] minutes) when SBP reached values higher than 160 mmHg. The increase in DBP showed a similar pattern with an average increase of 25 mmHg till the end of ST. HR also increased on the average by 10 bpm, but this parameter showed the greater individual variability relative to similar BP values among OVER. In OVER, different signs were related to the severe SBP hypertension: trembling (50%), nausea (25%), sweating, and light-headedness (18.0% and 12.5%, respectively) during ST.
SYN, participants who experienced a harness hang syncope; OVER, participants who experienced a severe blood hypertension; NORM, participants who ended the suspension test for other reasons (see text for furthers information).
Experienced in harness use versus nonexperienced.
p < 0.001 compared with the corresponding value of the same group after 8–12 minutes.
p < 0.001 compared with SYN, same column.
p < 0.0001 compared with OVER, same column.
BL, baseline; BP, blood pressure; HR, heart rate; Pet, end tidal pressure; SaO2, O2 saturation; SD, standard deviation.
In NORM (n = 28), SBP was increased from baseline by 10 mmHg after 8–12 minutes (significantly lower than OVER) and remained steady up to the end of ST (29.9 [10.2] minutes). On average, DBP increased from baseline to the end of ST by 14 mmHg (significantly lower than OVER), respectively. In NORM, different reasons led to the end of ST, including: systolic hypotension (14%), diastolic hypertension (42%), HR increase from baseline value >25 bpm (8%), tremble (17%), headache (17%), sweating (7%), and subjective poor harness comfort (21%). During recovery, in both these groups, differences in SBP and DBP pattern tended to disappear and HR showed a tendency to a bradycardic effect.
In SYN (n = 4), SBP showed ample oscillations within the first 8–12 minutes (significantly different from OVER and NORM) and a final significantly abrupt drop of −35.0 (12.2) mmHg with respect to baseline, preceding HHS (ST, 30.0 [7.7] minutes). Changes in DBP were not steady, and a significant decrease of −18.7 (8.5) mmHg was noticed in phase with the decrease in SBP, during the ST. HR also showed ample oscillations as in the other two groups, with a final increase just before fainting (pre-syncopal sign) in three out of four participants. In SYN, remarkable bradycardia was observed during recovery.
Table 1 also summarizes for the three groups the experience in the use of a harness, PetCO2, SaO2. In SYN, SaO2 remained unchanged up to the sharp decrease preceding syncope and PetCO2, increased at the onset of ST, and returned thereafter below normal at the end of ST.
Events related to syncope
Clinical characteristics of HHS were: (a) abrupt onset (few seconds) in two participants, with only evanescent symptoms before the loss of consciousness; (b) slower onset (from seconds to minutes) in two participants, with nausea and light-headedness before syncope. Among the SYN, one was a sedentary woman not used to wearing harness; one was a man, a professional user of the harness and a highly trained sky runner athlete involved in international-level competitions (measured
Cerebral NIRS during ST and exercise
Figure 2A and B shows that Δ[HbO2] and Δ[Hbtot] significantly increased in OVER and NORM, if compared with SYN, toward the ST (p < 0.001). In SYN, a plateauing was observed early after the onset of the ST, with a significant severe decrease preceding HHS (p < 0.05). Panel C shows a progressive but non-significant increase in Δ[HHb] in OVER and NORM during the ST, if compared with baseline. Meanwhile in SYN, after an initial increase in Δ[HHb], a decrease was observed with a final increase preceding HHS (p < 0.05, comparing the last two mentioned values). Once in the supine position, a rapid increase in Δ[HbO2] and Δ[Hbtot] was observed, whereas Δ[HHb] decreased.
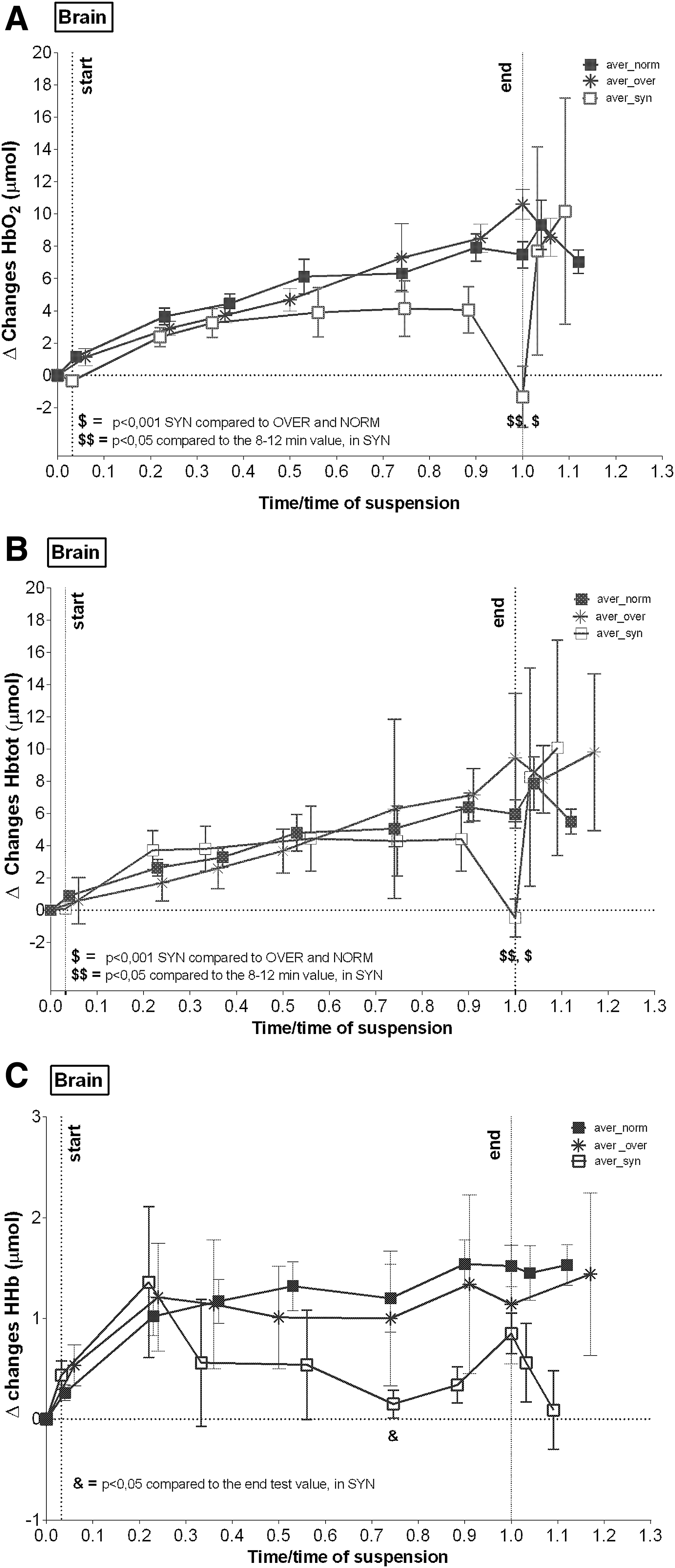
Mean (SE) values of cerebral O2 oxygenation. Δ[HbO2]
During the incremental exercise, the time course of brain NIRS (data were pooled for all participants as no differences were noticed) showed an increase in Δ[HbO2], with Δ[Hbtot] reaching a plateau at about 80% of the maximum load; Δ[HHb] increased progressively till the end of the exercise.
Muscle NIRS during ST and postischemia
No appreciable changes in NIRS variables were observed in all subjects during the ST, similar to what is observed in resting conditions when not wearing a harness. On the other hand, the experimental thigh ischemia caused an expected increase of Δ[HHb] and a corresponding decrease of Δ[HbO2] till a plateau was reached and, as a consequence, the cuff deflated.
ST time and correlations
The measured
Discussion
This study was performed on a relatively large number of participants, including mountain climbers, as compared with previous studies, which gave us the opportunity to evaluate the individual variability in response to a potential source of cerebral hypoxia induced by suspension in a harness. The present NIRS data suggest that participants who did not develop HHS were able to activate a cardiovascular response of various intensities to defend brain O2 metabolic needs. Conversely, participants who developed HHS were not able to activate a cardiovascular response that was adequate to avoid cerebral hypoxia.
In SYN, NIRS data suggest that the development of cerebral hypoxia was an early phenomenon finally leading to HHS. Madsen et al. (1998) found that during head-up tilt test orthostatic hypotension, cerebral hypoperfusion and brain oxygenation (measured by NIRS) are related to syncopal symptoms. Our study found various degrees of dissimilarity during ST if compared with the head-up tilt test. The inappropriate control of cardiovascular reflexes in participants who developed HHS is instead similar to that reported in microgravity studies (Convertino et al., 1994; Henson et al., 1998; Serrador et al., 2000). The pathophysiology of HHS depends on several factors interfering with cerebral oxygenation; these include the orthostatic hypotension, the gravity-dependent pooling of blood and interstitial fluid in the lower parts of the body, and the lack of antigravity muscle activity. In addition, the discomfort caused by staying in the harness may also have contributed to the development of HHS in three out of four participants.
We, therefore, discuss the present data considering these factors and the risk of death if countermeasures are not immediately taken when HHS occurs in healthy individuals.
Brain tissue oxygenation and cerebral perfusion
According to Quaresima et al. (2000), cerebral cortex hemoglobin oxygen saturation measured directly at the forehead reflects predominately the saturation of the intracranial venous compartment of circulation. In OVER and NORM, cerebral NIRS data revealed a progressive increase in Δ[HbO2], concomitant with a moderate increase of Δ[HHb], which suggests a sustained O2 availability to match the metabolic needs of the brain tissue, as seen in maximal exercise (Nielsen et al., 2001; Gonzales-Alonso et al., 2004; Shibuya et al., 2004; Rasmussen et al., 2007).
Conversely, in SYN, the increased Δ[HbO2] was about 50% lower than in OVER and NORM, whereas the Δ[HHb] decreased, thus suggesting a decline in oxidative brain metabolism early in the symptom-free phase (Smith et al., 2003; Volianitis et al., 2008). In the pre-syncopal phase, a non-sustained O2 need (i.e., a decrease in O2 delivery and/or an increase in O2 extraction) was the cause of HHS. Based on the cardiovascular parameters we measured, where especially SBP was statistically lower if compared with OVER and NORM, we considered that HHS likely relates to a decreased cerebral blood flow and/or a decreased O2 extraction. Since the plateauing of Δ[HbO2] is an early phenomenon (developing within 8–12 minutes in SYN), when it is coupled to an increase in Δ[HHb], it appears to be the most important and early pathophysiological parameter to monitor when a critical level of cerebral hypoxia is reached and HHS develops.
To provide importance in Clinical Practice, one can envisage technology developments, commercialization, and clinical validation of NIRS portable devices that are able to evaluate cerebral oxygenation levels as easy to use as the pulse oximetry continuous monitoring of a patient's saturation. Forty years after its discovery, NIRS is currently at a stage of transition from basic clinical research to an adjuvant in clinical applications and our study goes in the direction of using NIRS in clinical everyday routine (Wolf et al., 2007; Rummel et al., 2014).
In this study, a similar occurrence was seen during the final steps of the CPET (from 80% to 100% of peak power), when cerebral oxygenation fell, showing an increased Δ[HHb] and a plateauing of Δ[HbO2]. This critical change in frontal cortex oxygenation is known to precede voluntary cessation of exercise (Subudhi et al., 2007). Similarly, the critical point of cerebral hypoxia reached by SYN when pre-syncopal signs are manifest can be heralded by a reduced activation of efferent neurons affecting the vasomotor control (Fu et al., 2012). Finally, the recovery of Δ[HbO2] after the end of ST may be explained by cerebral vasodilatation and required minutes after the decrease of sympathetic tone as an auto-regulatory and rapid (5 seconds) response to clinostatism (Madsen et al., 1998).
Control of BP and baroreflex response
Considering the SBP adaptation to the ST, we identify different levels of response. In OVER and NORM participants, a reflex response to set an increase in SBP occurs within 1–3 minutes from the start of ST and is completed within 8–12 minutes. In OVER, a strong peripheral vasoconstriction tone is the regulatory factor of SBP; in fact, the ST was terminated due to an SBP increase above the value set as criteria to end the test. In NORM, compared with the OVER, the increase in SBP was less marked; whereas in SYN, the control on SBP was lacking.
In the SYN, an inappropriate cardiovascular control was observed as SBP failed to increase in the first 8–12 minutes and further, it decreased markedly before fainting. A decrease in SBP, associated with syncope, was reported as resulting from a fall of CO and/or of total peripheral vascular resistance (Moya et al., 2009). The case of HHS is similar to the orthostatic intolerance observed in lower body negative pressure (LBNP) supine experiments and bed rest proposed by Convertino (2014), where a minimal muscular activity of anti-gravitary muscle is observed. Consistent with the notion that peripheral constriction plays a central role in maintaining BP, Convertino (2014) found that the systemic vascular resistance was greater in high-tolerant orthostasis participants compared with low, in line with greater elevations in the circulating vasopressor hormones (vasopressin, angiotensin, and norepinephrine).
Reflex syncope is regarded by some authors as the result of a loss of muscle sympathetic neural activity to limb muscles controlling arteriolar tone: The vasomotor regulatory centers located in the brain (medulla) fail to respond to the decreased afferent input from baroreceptors (located in the aortic arch, carotid sinus, cardiopulmonary arteries) to induce peripheral vasoconstriction (Dampney et al., 2003). Fu et al. (2012) found that muscle sympathetic neural activity is well preserved during symptom free tilting, thus confirming the loss of synchronization between muscle sympathetic neural activity and the arterial pressure as a consequence (and not as a cause) of syncope.
Looking at DBP, we found that its increase in OVER and NORM occurs when an efficient reflex is present and mirrors a possible increase in peripheral resistances at 8–12 minutes. Conversely, in SYN, an increase in DBP occurred during the ST (before the syncopal event), at variance with what was reported by Fu et al. (2012) in a population of healthy people with syncope during the tilt test. Thus, this finding in SYN seems to be not synchronized with the efficiency of the baroreflex control and could be attributed to an obstacle to a venous return that is further aggravated by the lack of movement of the lower limbs. An obstacle to a venous return by the harness straps at the thighs is not demonstrated by our NIRS data: The lack of increase in muscle Δ[HHb] during the ST essentially suggests no massive blood flow limitation from wearing the harness, at least not of the same amount as during a lower limb ischemia.
Regarding blood pooling at the splanchnic level and lower limbs as a cofactor to induce syncope, we documented a significant increase in the circumference of the calf and thigh after the ST in all participants. This is compatible with an impaired fluid balance between the vessels and the interstitium, with an increase in extravascular water. Apart from HHS, this involves a higher risk to develop a deep venous thrombosis as documented by Pisati et al. (2007) in working at heights while using harness.
The HR values appear to be less sensitive at 8–12 minutes during ST, compared with SBP and DBP, as an index of proneness to develop HHS. In LBNP, data support the notion that in addition to peripheral vascular constriction, an increase in HR represents a physiologically important response to tolerate an acute reduction in central blood volume (Furlan et al., 1998; Prakash and Madanmohan, 2005; Convertino, 2014). It appears plausible to identify an inappropriate control of cardiovascular reflexes as a common trait between the LNBP, bed rest, and the SYN in our study. The final result is an incapacity by SYN to control the circulation due to a failure in control cardiovascular reflexes, resulting in vasodilation and in a lack of HR increase.
In SYN, the unbalanced control of arterial BP by cardiovascular reflexes is not supported by an increase in HR and, therefore, the fate of a fallen global perfusion seemed unescapable. A protracted and increased cardio-inhibitory effect is certainly noticed in the recovery phase for SYN when bradycardia until asystole was shown and has to be taken into account when rescue procedures are started: Microgravity may compromise the capacity to increase both CO and peripheral vascular resistance after return to the orthostatic challenge of the upright posture in terrestrial gravity (Convertino et al., 1994; Hargens and Richardson, 2009).
Comfort of the harness, environmental conditions, and trauma events
The evaluation of the individual risk of developing HHS could have important implications for developing the countermeasures to avoid the potential conditions that limit cerebral oxidative metabolism during suspension and lead to the development of HHS. When looking at the variability in the duration of the ST among participants, one should consider the complex relationship between individual adaptations to the potential failure of O2 transport/utilization chain and/or symptoms of discomfort. The latter may be caused by the pain of wearing the harness. In 6 out of the 40 participants, interruptions of the ST was due to intolerable discomfort of the harness (Hsiao et al., 2012).
Also, environmental conditions are an important factor to consider when a harness has to be worn: Our data suggest a negative correlation between the duration of the ST and the ambient temperature, confirming a previous observation by Galli et al. (2011). As a consequence, mountain climbers and high-altitude workers are recommended to use caution when exposed to specific seasonal changes of temperature (particularly during the transition from cold to hot weather conditions) due to the higher risk of syncope. Unexpectedly, neither the long-term experience in use of a harness nor higher aerobic fitness levels appear to be protective factors against the development of HHS.
A limitation of this study, in terms of translating the results to an incapacitated free hanging climber in a harness, is that participants were not injured and a prompt rescue was available. In case of trauma, an injured climber might be at an increased risk of developing severe cerebral hypoxia.
In summary, the main indicator of unsuccessful cardiovascular reflex activation in SYN was related to the lack of control on SBP. The attainment of a critical point of cerebral hypoxia, related to the special condition of suspension, seems to be a likely cause of HHS. Given the relatively short time for developing HHS, we might recommend the following: (1) climbers should avoid solo conditions; (2) harnesses should be designed to assure comfort, rapid rescue, and a body posture that does not result in more critical cerebral O2 perfusion when losing consciousness; and (3) as to the immediate treatment of HHS, the supine position that we adopted was certainly adequate to prevent more severe cerebral hypoxia.
Finally, based on our results, we believe that HHS is a fairly more appropriate term with respect to “Suspension Trauma” for defining this potentially harmful event.
Footnotes
Acknowledgments
The authors are indebted to the inspiring figure of Prof. G. Pisati, who devoted his life toward the safeguarding of workers. They sincerely thank G. Moles, former President of Lombardy Alpine guide. They also thank Prof. David Bishop, a knowledgeable native speaker, and Drs. Hayley Vergani and Cinzia Molteni for their technical assistance.
Author Disclosure Statement
No competing financial interests exist.