
Abstract
Abstract
Lizamore, Catherine A., and Michael J. Hamlin. The use of simulated altitude techniques for beneficial cardiovascular health outcomes in nonathletic, sedentary, and clinical populations: A literature review. High Alt Med Biol 18:305–321, 2017.
Background:
The reportedly beneficial improvements in an athlete's physical performance following altitude training may have merit for individuals struggling to meet physical activity guidelines.
Aim:
To review the effectiveness of simulated altitude training methodologies at improving cardiovascular health in sedentary and clinical cohorts.
Methods:
Articles were selected from Science Direct, PubMed, and Google Scholar databases using a combination of the following search terms anywhere in the article: “intermittent hypoxia,” “intermittent hypoxic,” “normobaric hypoxia,” or “altitude,” and a participant descriptor including the following: “sedentary,” “untrained,” or “inactive.”
Results:
1015 articles were returned, of which 26 studies were accepted (4 clinical cohorts, 22 studies used sedentary participants). Simulated altitude methodologies included prolonged hypoxic exposure (PHE: continuous hypoxic interval), intermittent hypoxic exposure (IHE: 5–10 minutes hypoxic:normoxic intervals), and intermittent hypoxic training (IHT: exercising in hypoxia).
Conclusions:
In a clinical cohort, PHE for 3–4 hours at 2700–4200 m for 2–3 weeks may improve blood lipid profile, myocardial perfusion, and exercise capacity, while 3 weeks of IHE treatment may improve baroreflex sensitivity and heart rate variability. In the sedentary population, IHE was most likely to improve submaximal exercise tolerance, time to exhaustion, and heart rate variability. Hematological adaptations were unclear. Typically, a 4-week intervention of 1-hour-long PHE intervals 5 days a week, at a fraction of inspired oxygen (FIO2) of 0.15, was beneficial for pulmonary ventilation, submaximal exercise, and maximum oxygen consumption (
Introduction
A
However, for a nonathletic population, the real-world practicalities of work and family commitments typically prohibit the use of real altitude exposure, restricting these users to a variety of simulated altitude models (Wilber, 2001). These simulated protocols either use hypobaric chambers or create a normobaric hypoxic environment through nitrogen dilution (Wilber, 2001), recycling expired air using rebreathers (Sausen et al., 2003), or using a polymeric membrane air separation process to filter out oxygen by devices called “hypoxicators” (Serebrovskaya et al., 2003).
While there is little doubt that there are differences between hypobaric and normobaric hypoxia (Levine et al., 1988; Roach et al., 1996; Snyder et al., 2006; Girard et al., 2012; Millet et al., 2012a, 2012b), it is the reduction of oxygen that is the trigger for adaptations associated with the oxygen-sensing transcription factor, the α-subunit of hypoxia-inducible factor-1 (HIF-1α) (Mounier and Brugniaux, 2012a, 2012b). For example, activation of HIF-1α upregulates genes responsible for angiogenesis, erythropoiesis (Semenza, 2009), iron homeostasis [observed as an increase in hemoglobin (Clark et al., 2009; Saunders et al., 2009)], and altered glucose and energy metabolism (Semenza, 2001).
In addition to these adaptations, physiological changes such as increased chemoreflex sensitivity to hypoxia (Bernardi et al., 2001), increased pulmonary arterial pressure (Zhao et al., 2001), and increased subsarcolemmal mitochondrial expression (Schmutz et al., 2010), which is a subgroup of mitochondria that appears to be most responsive to endurance training (Koves et al., 2005), are observed. While the hematological adaptations (red blood cells and hemoglobin in particular) typically receive most of the credit for improved athletic performance (Levine and Stray-Gundersen, 2005), nonhematological adaptations such as improved muscle buffering capacity, lactic acid tolerance, and greater mitochondrial efficiency (Gore et al., 2007) are increasingly being viewed as equally important (Garvican et al., 2011).
All altitude and simulated altitude training protocols usually involve a relatively brief altitude exposure (typically a few weeks) for the purpose of adapting the body to either enhance sea level performance or reduce the compromise in performance at altitude. Thereafter, the individual returns to sea level for their usual training. As such, the hypoxic exposure is “intermittent”. However, the “intermittent” nature of the hypoxic dosage is highly varied and several different training approaches have been developed.
Some popular altitude training methods include the following: live high train high, live high train low (LHTL), intermittent hypoxic training (IHT), and intermittent hypoxic exposure (IHE). Refer to Table 1 for a description of these techniques. Typically, prolonged hypoxic exposure (PHE) such as protocols incorporating a “live high” element or protocols incorporating exercise in hypoxia use lower hypoxic dosages (2000–3000 m), while shorter hypoxic exposures, as is used in passive IHE models, use a higher hypoxic dosage (4000 m). At times, a combination of these techniques is used. For example, IHT may be used in conjunction with IHE, whereby participants initially perform 30–60 minutes of exercise in hypoxia followed by another 3 hours of passive hypoxic exposure. Alternatively, additional IHT may be performed in conjunction with the LHTL model (also referred to as “live high train low and high”).
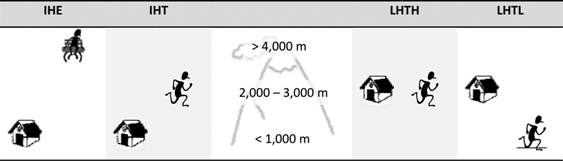
IHE is usually achieved using either a hypobaric chamber or altitude tent, or by delivering a lower FIO2 through a hand-held face mask. This method of simulated altitude exposure is distinct from the others in that, there is no physical training performed within or alongside the altitude exposure. Hypoxic exposure can range from several repeated doses of a few minutes of hypoxic exposure interrupted by several minutes of ambient air over 40–90 minutes, or a single dose of several hours. IHT requires that the individual either travels to real altitude for their training program or trains within a hypobaric chamber (hypobaric hypoxia) or altitude tent (normobaric hypoxia), or while inspiring a hypoxic gas delivered through a face mask. The individual then returns to sea level following the exercise. During LHTH, the individual either resides at and trains in real altitude, in a hypobaric chamber (hypobaric hypoxia), or in an “altitude apartment” (normobaric hypoxia). The hypoxic exposure is uninterrupted and can range in time from several days to several weeks. However, with LHTL, the individual resides at real altitude, in a hypobaric chamber, in an “altitude apartment”, or in an “altitude tent”, but returns to a normoxic environment for training. The hypoxic exposure usually ranges from 8 hours (in the case of altitude tents) to 18–20 hours (in altitude apartments, real altitude, or hypobaric chambers).
FIO2, fraction of inspired oxygen; IHE, intermittent hypoxic exposure; IHT, intermittent hypoxic training; LHTH, live high train high; LHTL, live high train low.
The purpose of this review is to determine the extent to which simulated altitude has been investigated in nonathletic/sedentary populations and examine the treatments used and findings from the retrieved articles.
Methods
Science Direct, PubMed (via Medline), and GoogleScholar, were searched using a combination of “include” and “excluding” terms. In addition to these databases, all American Physiological Society journals and the “High Altitude Medicine and Biology” journals were searched individually. The focus of this literature review is on the health-related adaptive response to short-term, simulated altitude in un-acclimatized, nonathletic/sedentary humans. Excluding factors included studies involving high-altitude natives, permanent or long-stay sojourns to real altitude, mountaineering expeditions, or hypoxia associated with disease states (obstructive sleep apnea, ischemic heart disease, or neonatal hypoxia), single dose, and all animal studies. Inclusion factors comprised the following: an intervention-styled study, individuals ranging from healthy (but sedentary) to diseased states, adult participants, the provision of voluntary written informed consent, and English-speaking, full-text, peer-reviewed academic journal articles. Refer to Figure 1 for all search terms used, and the filtering process. In addition, the reference lists of selected review articles (Muza, 2007; Wilber, 2007; Bärtsch et al., 2008; Burtscher et al., 2010; Astorino et al., 2015) were reviewed and any additional articles were added.
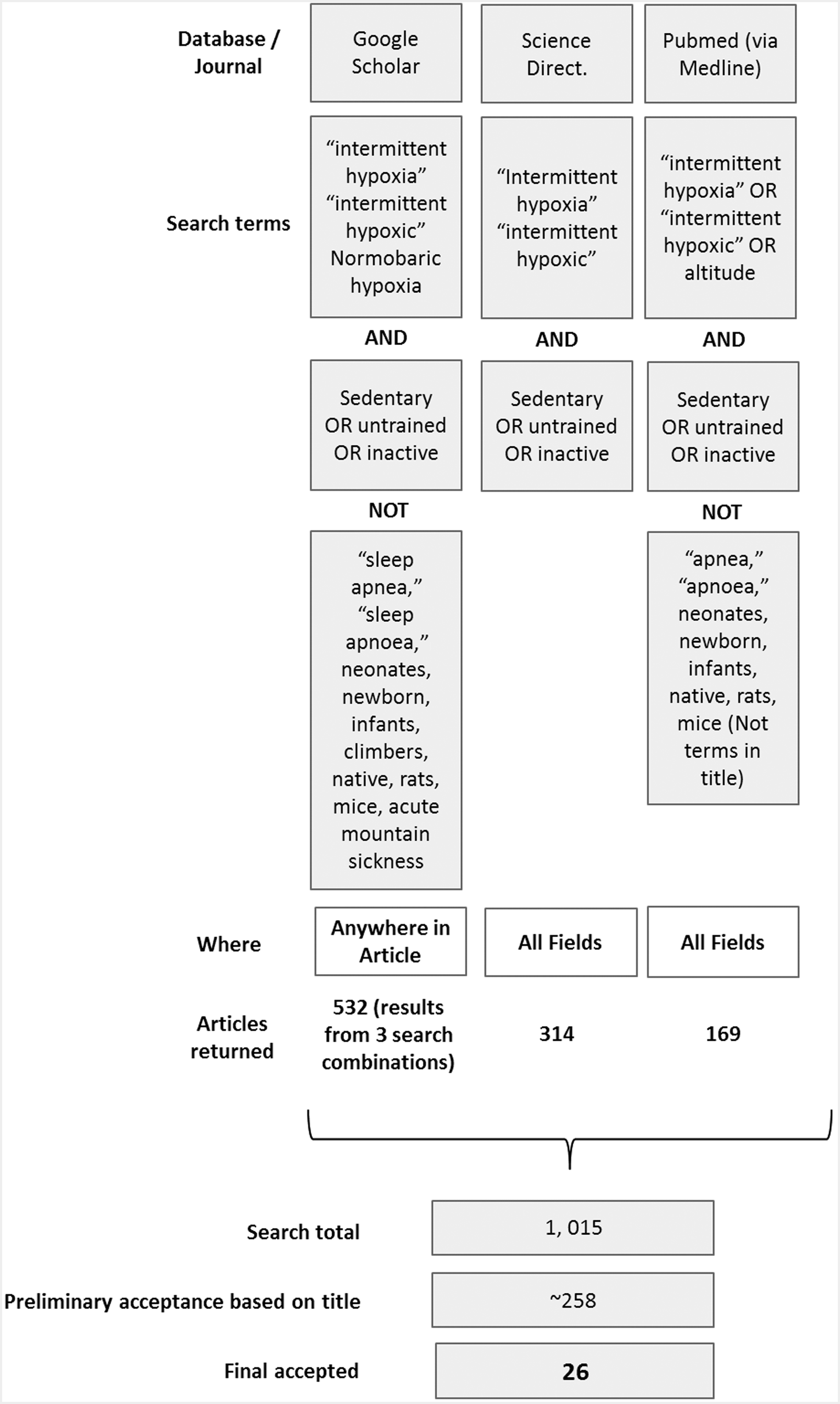
Overview of database and journal search procedure.
The specificity of population-related search terms (“sedentary” OR “untrained” OR “inactive”) may have excluded studies where the training status of the population was not specified. So this review should be considered an extensive, rather than an exhaustive review.
A quality assessment protocol adapted from van Tulder et al. (1997) and used in whole body vibration studies (Rehn et al., 2007; Manimmanakorn et al., 2014) was used to assess the quality of the selected journal articles. In short, the quality of the studies was based on the suitability of patient selection, intervention, outcome measurements, timing of the follow-up measurements, and the statistical approach to the study. Each “yes” yielded 1 point and was therefore assessed on a 16-point scale using the following qualitative outcome: >11 points: high quality; 7–10 points: moderate; and <6 points: low methodological quality.
After articles were retrieved and documented, they were then sorted into one of two participant categories:
• Sedentary/untrained • Clinical
Deciding to include a study of nonathletic, but active participants was, at times, difficult, and the ultimate decision to include the study or not often came down to the wording used by the authors. For example, if participants were described as healthy and explicitly stated noninvolvement in exercise or physical activity, or were “untrained,” they were included in the review. In cases where participants were described as healthy, but no explicit physical activity level was recorded, but included a description akin to “healthy lowlanders, not taking medications and without disease,” the study was included in a “healthy/active” category and was not included in this review. Therefore, there is a possibility that some studies have been misclassified, and have been incorrectly omitted from this review.
Within the IHE protocol, there were two distinct techniques: Those that included one continuous, passive exposure of simulated altitude, usually over 3–4 hours, and those that included short (several minutes) severe hypoxic exposure alternated with a similar duration of ambient air, and repeated for 40–90 minutes. For the sake of clarity, repeated, short intervals of hypoxic air alternated with short periods of breathing normoxic air will be referred to as intermittent hypoxic exposure (IHE), while the sustained periods of passive hypoxic exposure will be referred to as PHE.
Results
The most common reasons for the rejection of articles were as follows: nonintervention studies, reviews/commentaries/debates, real-altitude studies, duplicates, animal studies, case studies, or were irrelevant. Four articles (Ciuha et al., 2015; Stavrou et al., 2015; Debevec et al., 2016; Rittweger et al., 2016) were excluded due to extended confinement (with and without bedrest) akin to long-stay sojourns. Articles ranged in date from 1992 to 2016, and were generally of moderate (n = 14, 53.9%) to high (n = 9, 34.6%) quality, with only three articles of low quality (11.5%) (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/ham)
Studies were male dominant (Table 2) and in the sedentary/untrained group, two distinct age groups were evident: 14 studies ranged in age from 19–29 years and 8 studies ranged in age from 42–64 years.
Discussion
The effectiveness of simulated altitude in altering health states in a sedentary or clinical population makes up a minority of the overall simulated altitude research field. This review has divided the “sedentary population” into clinical participants and sedentary, but otherwise healthy participants. The first part of this review provides an overview of the findings for each simulated altitude study on the health outcomes, and critiques the studies making up the section. In the second part of the discussion, health measures worthy of further exploration are examined.
Clinical populations
There were only four articles examining the effect of IHE in a clinical population, all of which used passive hypoxic exposure (Table 3). Within the IHE protocols, one article focused on interval IHE (Haider et al., 2009) and three focused on PHE (Tin'kov and Aksenov, 2002; del Pilar Valle et al., 2006; Saeed et al., 2012). The studies examining the use of simulated altitude in a clinical population are promising. The three articles examining PHE have found that ∼3–4 hour episodes of sustained PHE at a simulated altitude of 2700–4200 m for 2–3 weeks in patients with various forms of heart disease appear to have beneficial effects on blood lipid profile, myocardial perfusion, and exercise capacity. While there appears to be potential for IHE to improve autonomic function in a clinical population, only one study has used this protocol and so, further placebo-controlled (or randomized crossover), double-blind studies are required before more certain conclusions can be made.
Hypobaric hypoxia.
↑, increase; ↓, decrease; ⇆, no change; C: control; sham: normoxic placebo; COPD: chronic obstructive pulmonary disease; F, female; HDL, high-density lipoprotein; LDL, low-density lipoprotein; HCVR, hypocapnic ventilatory response; HVR, hypoxic ventilatory response; M, male; NS, not significant ; PHE, prolonged hypoxic exposure; RR, R wave-to-R wave interval, average distance between RR peaks; SBP, systolic blood pressure;
Intermittent hypoxic exposure
There was only one study examining the effect of IHE in a clinical population. The aim of Haider et al.'s study was to assess whether IHE could attenuate the decline in cardiovascular autonomic function in patients with chronic obstructive pulmonary disease (COPD) (Haider et al., 2009). Following the 3-week trial, participants receiving IHE demonstrated improved baroreflex sensitivity and a slight (nonstatistically significant) decrease in systolic blood pressure (SBP) compared to baseline data. Heart rate variability (R wave-to-R wave [RR] interval) also increased, suggesting improved parasympathetic modulation of the autonomic nervous system.
Prolonged exposure
The reports of improved exercise tolerance (Saeed et al., 2012), myocardial perfusion (del Pilar Valle et al., 2006), and blood lipid profile (Tin'kov and Aksenov, 2002) in a clinical population following PHE are promising. However, the small number of studies in this population and the different focus in each of the studies make it difficult to assess the repeatability of the respective findings. There are also limitations in each of these studies that cloud the clarity of outcomes in these trials.
The major limitation in these studies has been the lack of a control group. For example, despite a relatively large (n = 46) number of participants, Tin'kov and Aksenov (2002) did not include a group receiving a normoxic placebo. Therefore, it is possible that the change in the blood lipid profile over the course of the study could have been attributed to the participant's ongoing use of medication, a change in season (Ockene et al., 2004), change in physical activity level, or diet. Similarly, oral acetazolamide was administered to 11 of the 12 participants in Saeed et al.'s (2012) study before the PHE treatment to prevent altitude sickness. Acetazolamide has been reported to reduce maximum oxygen consumption (
The small sample size in the study by del Pilar Valle et al. (2006) was possibly their largest limitation. However, given the high-risk population used in their trial and the absence in participant motivation required for their measurements, their results are likely valid. The improvement in myocardial perfusion was attributed to the improved blood flow from increased angiogenesis and/or increased vasodilation as a result of improved serum nitric oxide following the PHE protocol.
IHT and IHE in sedentary or untrained populations
The results of the studies utilizing sedentary/untrained, but otherwise relatively healthy individuals are summarized in Table 4. The research involving this cohort focused exclusively on IHE, PHE, and IHT training modalities. Overall, the quality of these studies was better than in the clinical groups, with more researchers reporting comparisons relative to control groups.
Hypobaric hypoxia.
ANS, autonomic nervous system; BP, blood pressure; DBP, diastolic blood pressure; Hb, hemoglobin; HCVR, hypocapnic ventilatory response; HIF-1α, hypoxic inducible factor-1; HR, heart rate; HVR, hypoxic ventilatory response;
Intermittent hypoxic exposure
Five studies used IHE as the simulated altitude model, and included populations ranging from participants with mild COPD (or at risk for COPD), who were overweight, to people who were healthy and normally active, but elderly (60–74 years). Most of the studies reported an improvement in exercise tolerance during a submaximal workload (Burtsher et al., 2004; Shatilo et al., 2008; Burtscher et al., 2009; Lizamore et al., 2016), particularly in those with greater disease (Burtsher et al., 2004) or a sedentary nature (Shatilo et al., 2008). Changes in maximal exercise capacity were somewhat harder to detect. Only the elderly men in Burtscher et al.'s (2004) earlier study demonstrated a clear increase in
There were several conflicting hematological adaptations in response to the IHE protocol. For example, while some studies report an increase in red blood cells (Burtsher et al., 2004) and hemoglobin (Burtsher et al., 2004; Burtscher et al., 2009), others have noticed no such change (Shatilo et al., 2008). Interestingly, both Shatilo et al.'s (2008) and Burtscher and et al.'s (2009) later study reported small, but not statistically significant decreases in cholesterol, which is in line with the improvement in blood lipid profile following PHE in a clinical population (Tin'kov and Aksenov, 2002). However, the decrease in cholesterol in the test group in Burtscher et al.'s (2009) study was similar to the decrease in the control group and therefore these results are equivocal and add doubt to the assumed intervention-based changes in the clinical cohort (Burtscher et al., 2009).
The IHE intervention also appeared to reduce systemic stress. Balykin et al. (2004) and Lizamore et al. (2016) demonstrated improved heart rate variability following the hypoxic exposure intervention, indicating improved sympathetic/parasympathetic balance. This was also reflected in the reduced systolic blood pressure (Shatilo et al., 2008; Burtscher et al., 2009) reported by others. The study by Balykin et al. (2004) primarily investigated the effectiveness of different IHE protocols with and without the use of exercise. The IHE protocols used in conjunction with exercise training (either simultaneously or sequentially) were more effective regarding exercise capability (see discussion regarding “Intermittent hypoxic training”). Typically, participants receiving IHE appear to tolerate hypoxia well. The most frequently reported side effects include dizziness, shortness of breath, and chest discomfort (Shatilo et al., 2008; Lizamore et al., 2016). However, there may be some risk to blood pressure in severe hypoxia (fraction of inspired oxygen [FIO2] ≤0.12) intervals lasting more than 7 minutes (Shatilo et al., 2008), whereas 5-minute intervals were tolerated well. There have also been some reports of tinnitus following IHE (Shatilo et al., 2008). Interestingly, in both Burtscher et al.'s studies (Burtsher et al., 2004; Burtscher et al., 2009) and in the study by Lizamore et al. (2016), side effects were also observed in the control groups who reported feeling dizzy or sleepy during the hypoxic exposure. The side effects also seem to be highly individual, with some participants reporting no side effects and others frequently reporting discomfort (Lizamore et al., 2016). Therefore, researchers should consider the sensitivity of their participants to hypoxia before enrolling them in the study.
All the IHE studies made use of a control group of sorts (while Shatilo et al. (2008) did not use a placebo group, they did examine the same intervention in sedentary compared to active participants; Balykin et al. (2004), on the other hand, only used sedentary participants, but compared a range of different simulated altitude techniques). Of note is that, while some of the hematological parameters are unclear, there were no negative health outcomes attributed to the IHE interventions (such as increased SBP, or a decline in exercise tolerance). Intermittent hypoxic exposure appears to present a reasonable possibility of health benefit, particularly for those with limited exercise ability. Care should be taken to carefully monitor side effects during the hypoxic exposures; however, symptoms of discomfort seem to readily abate upon return to normoxic conditions.
Prolonged hypoxic exposure
Only the studies by Wang et al. (2007a, 2007b, 2010) and Gatterer et al. (2015) have used normobaric PHE, while the others used hypobaric hypoxia. Wang et al. focused primarily on how hypoxic severity (FIO2 of 0.12 vs. 0.15) affects hemodynamic control (Wang et al., 2007a, 2010) and eosinophil- and neutrophil- platelet aggregation, and the cytokine response to strenuous exercise (Wang et al., 2007b), as well as exercise tolerance and ability.
The results of Wang et al.'s studies are extremely useful in gauging an appropriate dosage of PHE in both session duration and session intensity. For example, 4 or 8 weeks of 1-hour-long PHE, 5 times/week using an FIO2 of 0.15 resulted in improved pulmonary ventilation, submaximal exercise performance, and
Contrastingly, 8 weeks of the same PHE protocol at an FIO2 of 0.12 or 0.15 resulted in a reduction in the proinflammatory cytokine and thrombo-inflammatory responses to strenuous exercise, but only the group receiving an FIO2 of 0.12 demonstrated a substantial increase in circulatory anti-inflammatory cytokines IL-6 and IL-10 during hypoxia and exercise, and at rest (Wang et al., 2007b). Wang et al. (2010) noted no significant difference between PHE and normoxic controls on exercise ability. While the effects of hypobaric PHE are likely to improve hypoxic sensitivity (Katayama et al., 1998) and acclimatization through increased ventilation and SpO2 during hypoxic exercise (Ricart et al., 2000), there is insufficient literature available to comment on its effectiveness as a means of improving exercise tolerance or health in a sedentary population. Overall, a normoxic PHE protocol of >4 weeks for 1 hour/day, 5 days/week at an FIO2 of 0.15 is likely to be the safest PHE model for a sedentary/untrained population. While this protocol may improve submaximal performance and
Intermittent hypoxic training
When researchers have used identical exercise intensity protocols in hypoxic, compared to normoxic conditions, the participants training in hypoxia have demonstrated superior aerobic capacity following as little as 6–10 IHT sessions (Katayama et al., 1998; Balykin et al., 2004) for as long as 4–5 weeks (Wang et al., 2010; Mao et al., 2011) of IHT (30 minutes/day and 5 days/week). However, other researchers have demonstrated no improvement in sea level performance compared to the control group following 5–6 weeks of IHT (between 67% and 80%
Interestingly, even when there is little change in exercise performance, there are likely to be hypoxia-related adaptations at the cellular level (Geiser et al., 2001; Vogt et al., 2001; Friedmann et al., 2003). For example, despite positive correlations between mRNA levels of vascular endothelial growth factor (VEGF) and myoglobin, and between phosphofructokinase and lactate dehydrogenase following IHT (but not before), there was no additional advantage of strength training in hypoxia compared to normoxia (Friedmann et al., 2003). Other structural alterations reported as a consequence of IHT include significant increases in muscle volume of knee-extensors, capillary length density, which is the capillary length in 1 mm3 (Tomanek, 2013), and mitochondrial volume density (Geiser et al., 2001; Vogt et al., 2001), and elevated mRNA concentrations of the HIF-1α (Vogt et al., 2001), that is, HIF-1α is a subunit of hypoxia-inducible factor-1, which is responsible for upregulating genes that act to reduce the hypoxic stress and include the promotion of erythropoietin and VEGF (Wenger and Gassmann, 1997).
None of the studies reported any beneficial erythropoietic response as a consequence of 4–6 weeks of IHT (Engfred et al., 1994; Geiser et al., 2001; Wang et al., 2010; Mao et al., 2011). Indeed, Mao et al. (2011) demonstrated accelerated aging, decreased size, a reduction in the ability of erythrocytes to deform under stress, and increased eryptotic (or suicidal cell death) response to hydrogen peroxide in cells, following IHT. These findings raise concern over the appropriateness of IHT interventions in groups or clinical populations with blood disorders that may become further compromised following IHT.
However, potentially valuable adaptations for a sedentary population that were reported following IHT include improved autonomic balance and increased lipid metabolism as evidenced by a lower RER during exercise (Balykin et al., 2004), which was possibly responsible for the 13% decrease in body fat compared to little change following normoxic exercise (Balykin et al., 2004). However, the value of adding hypoxia to a long-term weight loss exercise program was negligible in a recent study (Gatterer et al., 2015).
In Gatterer et al.'s study, both the IHT groups (one working at the same absolute intensity as the normoxic control group and the other at a relative intensity factoring in the added altitude stress) demonstrated similar fitness and body composition changes as the normoxic control group. The authors noted that given the similar fitness and body composition outcomes at lower absolute exercise intensity (in the relative hypoxic group), the IHT may be worthwhile in a cohort unable to physically perform a higher level of physical activity. Otherwise, there was no added advantage of IHT over regular exercise training in an obese population (Gatterer et al., 2015). Nishiwaki et al. (2011) reported improvements in vascular health (decreased pulse wave velocity and improved flow-mediated vasodilation) following hypobaric IHT, but not normoxic exercise. Further research should examine whether these improvements in vascular health can be repeated following normobaric hypoxia.
Key areas for future research in a sedentary or clinical population
In the sedentary and clinical populations, IHT does not appear to be particularly more effective than normoxic training in improving exercise capacity (Vogt et al., 2001; Friedmann et al., 2003; Pesta et al., 2011; Gatterer et al., 2015); however, the effects on vascular health are promising (Nishiwaki et al., 2011; Shi et al., 2013). Contrastingly IHE appeared to be effective in inducing beneficial adaptations, such as improved submaximal aerobic fitness and exercise tolerance (Burtsher et al., 2004; Shatilo et al., 2008; Burtscher et al., 2009), autonomic modulation (Balykin et al., 2004), and blood lipid profile (Tin'kov and Aksenov, 2002).
Autonomic modulation and systolic blood pressure
A decline in autonomic function may be linked to numerous risk factors for cardiovascular disease, and indeed even precede the risk factors themselves (Thayer and Lane, 2007). With this in mind, the potential for hypoxic exposure treatments to improve autonomic balance in a sedentary population warrants further investigation.
While there is an increase in sympathetic activity with hypoxia (Lizamore et al., 2016) as evidenced by an increase in heart rate variability, systolic blood pressure, and heart rate with hypoxia (Rodway et al., 2007), the “training effects” of this sympathetic activation appears to result in reduced basal sympathetic activity (Lizamore et al., 2016). Indeed, a decrease in resting (Shatilo et al., 2008) and exercising (Burtsher et al., 2004) systolic blood pressure has been observed following an IHE protocol at an FIO2 of 0.12 (particularly in a sedentary population). The improvements in autonomic regulation (Balykin et al., 2004; Haider et al., 2009; Lizamore et al., 2016) appear to be particularly effective in an unhealthy population (overweight and at risk of or with mild COPD), compared to their more healthy counterparts (Bernardi et al., 2001). However, these improvements do not appear to be associated with PHE (Wang et al., 2007a). Therefore, when selecting a mode of hypoxic intervention for a sedentary population, an IHE protocol (rather than PHE) may be preferential in a sedentary population who may be at risk of high BP.
Blood lipid profile and vascular health
High-density lipoprotein (HDL), low-density lipoprotein (LDL), and total cholesterol are important considerations in the assessment of a person's overall cardiovascular risk (New Zealand Guidelines Group, 2003). However, the effect of hypoxic intervention in these measures is conflicting. For example, Tin'kov et al. reported decreased total cholesterol and LDL and a corresponding increase in HDL following PHE (Tin'kov and Aksenov, 2002); however, Gatterer et al. (2015) reported no real differences in these measures between their groups receiving IHT + PHE and normoxic exercise. Furthermore, placebo-controlled trials examining the differences in hypoxic dose on blood lipid profile would be valuable. For example, two recent studies have demonstrated an improvement in vascular health following IHT protocols in both postmenopausal women and healthy young men (Nishiwaki et al., 2011; Shi et al., 2013). However, Wang et al. (2007a) have reported a decrease in hemodynamic function following a PHE of 60 minutes (FIO2 of 0.12), but not following 60 minutes at an FIO2 of 0.15 (Wang et al., 2007a; Wang et al., 2010), which suggests that the severity of the hypoxic stimulus should pass a minimum threshold, but not be excessive (for the sedentary or clinical population, “excessive” may be an FIO2 below 0.12 for an hour or more).
An improvement in flow-mediated dilation and arterial compliance was noted following 2 hours of IHT+PHE at a simulated altitude of 2000 m (IHT: 30 minutes of swimming at 50%
Dosage
Katayama et al. have investigated various alterations and adjustments between the different hypoxic delivery modalities. In doing so, Katayama's research group has established that, there is no added advantage to using a 3-hour exposure compared to 1 hour of hypoxia for enhancing hypoxic ventilatory chemosensitivity, 14 days are better than 7 days for enhancing central hypercapnic ventilatory chemosensitivity, and an FIO2 of 0.123 is better than 0.15 for improving resting (but not exercising) hypoxic chemosensitivity (Katayama et al., 2005; Katayama et al., 2007; Katayama et al., 2009). However, most of these studies have been conducted in well-trained cohorts, using the PHE model, and were focused on acclimatization. Further research regarding dosage is needed in a sedentary population. Furthermore, no researchers have investigated the differences in the frequency of hypoxic exposures per week. As there are no additional advantages to a longer session compared to a shorter session (1 hour compared 3 hours), or IHE to PHE (Koehle et al., 2007), a 60-minute IHE session may prove most beneficial for a sedentary population. In addition, IHE is unlikely to cause any increase in systolic blood pressure (Foster et al., 2005) and may avoid the reduction in hemodynamic function with 60 minutes of PHE at an FIO2 of 0.12.
Key points and further research from literature review
• The effects of simulated altitude on health outcomes in a sedentary or clinical population appear to range from not effective to beneficial.
• There is some evidence that severe PHE can be harmful at the cellular level (even in the absence of physical performance change) and so, researchers should carefully consider their population when designing their interventions.
• Based on the current literature, 1 hour of IHE to an FIO2 of 0.12 for at least 2 weeks is likely to be most worthwhile for health adaptation, with little risk of harm to health. Intervention response seems to decline following 3 months of treatment. More research is needed on the frequency of IHE per week for beneficial adaptation.
• Further research is needed regarding the effects of simulated altitude on autonomic function, vascular health, blood lipid profile, and the optimal hypoxic dosage for the improvement of these measures.
Footnotes
Acknowledgments
C.A.L. conceptualized and designed the study, C.A.L. and M.J.H. assisted in planning and acquisition of data, C.A.L. completed the analysis and interpretation of the data, and M.J.H. helped critically revise the article adding important intellectual content. C.A.L. received a research grant from the New Zealand National Heart Foundation.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.