
Abstract

To the Editor,
Pham et al. (2017), in their article entitled “Cross-Sectional Comparison of Sleep-Disordered Breathing in Native Peruvian Highlanders and Lowlanders,” err in applying the rules of normal sleep parameters from lowland to highland environments. With this approach, data from highlanders will obviously be categorized as “abnormal,” because human respiratory physiology is hugely different at low and high altitudes.
The authors state that they found a significant increase in the apnea/hypopnea index in highlanders because of increased central apneas. In our research on infants at 2560 m (Ucrós et al., 2015) and 3200 m above sea level (Ucrós et al., 2017), we have demonstrated that the observed increase in the central apnea index (CAI) is not real, but rather a reflection of periodic breathing (PB); it is known that PB is a normal feature at high altitude in adults (Bloch et al., 2010) as well as in children (Ucrós et al., 2015). Our studies show that when central apneas associated with PB are discounted, the CAI does not change significantly when altitude increases. This fact has already been reported by Parkins et al. (1998).
Furthermore, the authors maintain that an important increase in the oxygen desaturation index (ODI) occurs in highlanders rather than in lowlanders. Our data show that the gap between the oxygen saturation as measured by pulse oximetry (SpO2) 5th and 95th percentiles increases as the altitude increases (Fig. 1), and for this reason, the ODI established for lowlands cannot be applied at high altitudes, because SpO2 dips are much more frequent.
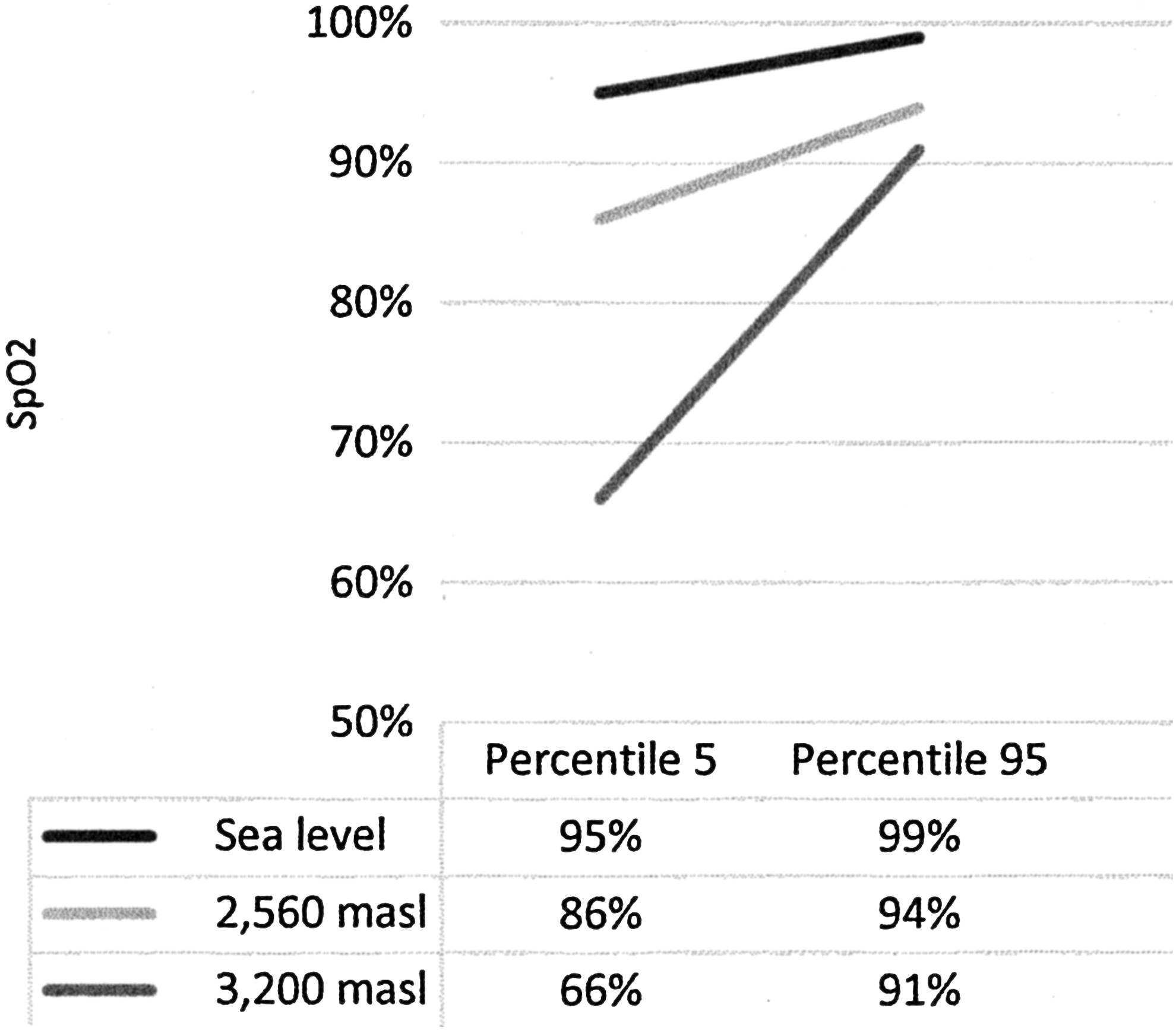
Oxygen saturation. Percentiles 5th and 95th for sea level, 2560 m, and 3200 m, in infants aged 1–4 months old during sleep.
In their discussion section, Pham et al. conclude that Our study demonstrated substantial increase in the prevalence and severity of SDB in highlanders, compared to lowlanders…. This conclusion cannot be supported in my view, because what the study really shows is that normal parameters during sleep are different for lowlanders than for highlanders, as would be expected.
In Figure 1, the authors postulate a vicious cycle in which hypoxia supposedly induces sleep-disordered breathing (SDB). In research we have conducted in infants, we do not find a correlation between PB and SpO2, and it was not found either in adults by Bloch et al. (2010). With the current evidence, I do not consider it possible to claim that hypobaric hypoxia characteristic of high altitude induces SDB.
The main conclusion of their study, stating …hypoxic exposure at altitude places highlanders at risk for the development of clinical sequelae of SDB…, is not adequately supported. Pham et al. consider altitude itself pathological, based on an incorrect analysis.