
Abstract
Abstract
Baniya, Santosh, Christopher Holden, and Buddha Basnyat. Reentry high altitude pulmonary edema in the Himalayas. High Alt Med Biol. 18:425–427, 2017.—Reentry high altitude pulmonary edema (HAPE), a subset of HAPE, is a well recognized, life-threatening illness documented almost exclusively in the North and South Americans, who live at high altitude (>2500 m) and return to their homes after a brief sojourn of days to months at lower altitude. This phenomenon has not been reported in Sherpas or other people of Tibetan origin in Nepal or India. And it has rarely been reported from Tibet. In this study we document a case of reentry HAPE in Manang region (3500 m) of Nepal in a 7-year-old Nepali boy of Tibetan ancestry who fell ill when he ascended to his village (Manang, 3500 m) from Besisahar (760 m) in 1 day in a motor vehicle after spending the winter (December to March) at Besisahar with his family. With more motorable road access to high altitude settlements in the Himalayas, reentry HAPE may need to be strongly considered by healthcare professionals in local residents of high altitude; otherwise life-threatening complications may ensue as in our case report.
A 7-
On presenting to the HRA aid post, the patient was observed to be minimally responsive with globally reduced tone. Work of breathing was markedly increased with a respiratory rate of 55 breaths per minute, chest wall retraction, use of accessory muscles, and nasal flare. Oxygen saturation measured by portable saturation probe was 44%. Chest auscultation revealed good air entry, which was equal bilaterally, but with crepitations throughout the lung fields. Heart rate was 150 beats per minute, and temperature was 35.7°C. He was diagnosed with reentry high altitude pulmonary edema (HAPE) (Scoggin et al., 1977; Hultgren and Marticorena, 1978) and high altitude cerebral edema (Basnyat and Murdoch, 2003) and was treated with high-flow oxygen and 3 mg of dexamethasone. A helicopter rescue was organized to fly him to Kathmandu (1300 m).
In Kathmandu, the treating doctor found him to have improved markedly. He was oriented appropriately, his vital signs were within normal limits, and he was ambulating with a normal gait. His oxygen saturation was 94% in room air with bilateral crepitations. His blood count, routine urine, creatinine, and liver function tests were normal. The chest X-ray revealed heterogeneous opacities in the lower and mid zones bilaterally (Fig. 1). He was discharged to his hotel in Kathmandu with no medicines and followed up after 2 days. In his follow-up consultation he was noted to have normal vesicular breath sounds with no added sounds and his repeat chest X-ray was normal (Fig. 2). He continued to do well and we last followed up a month ago.
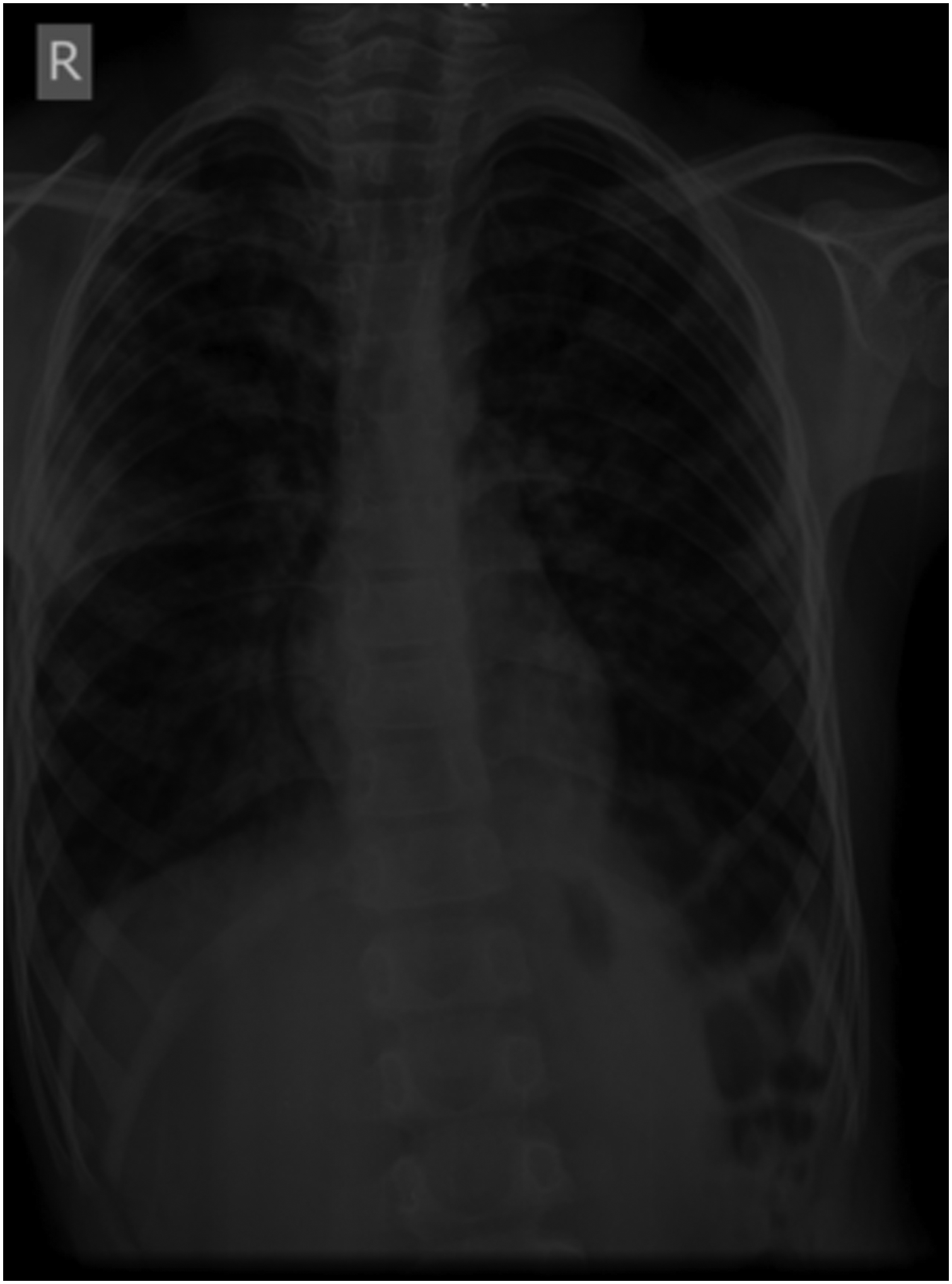
Chest X-ray of the patient at Kathmandu after helicopter evacuation. The X-ray reveals heterogeneous opacities in the lower and mid zone bilateral lung fields.
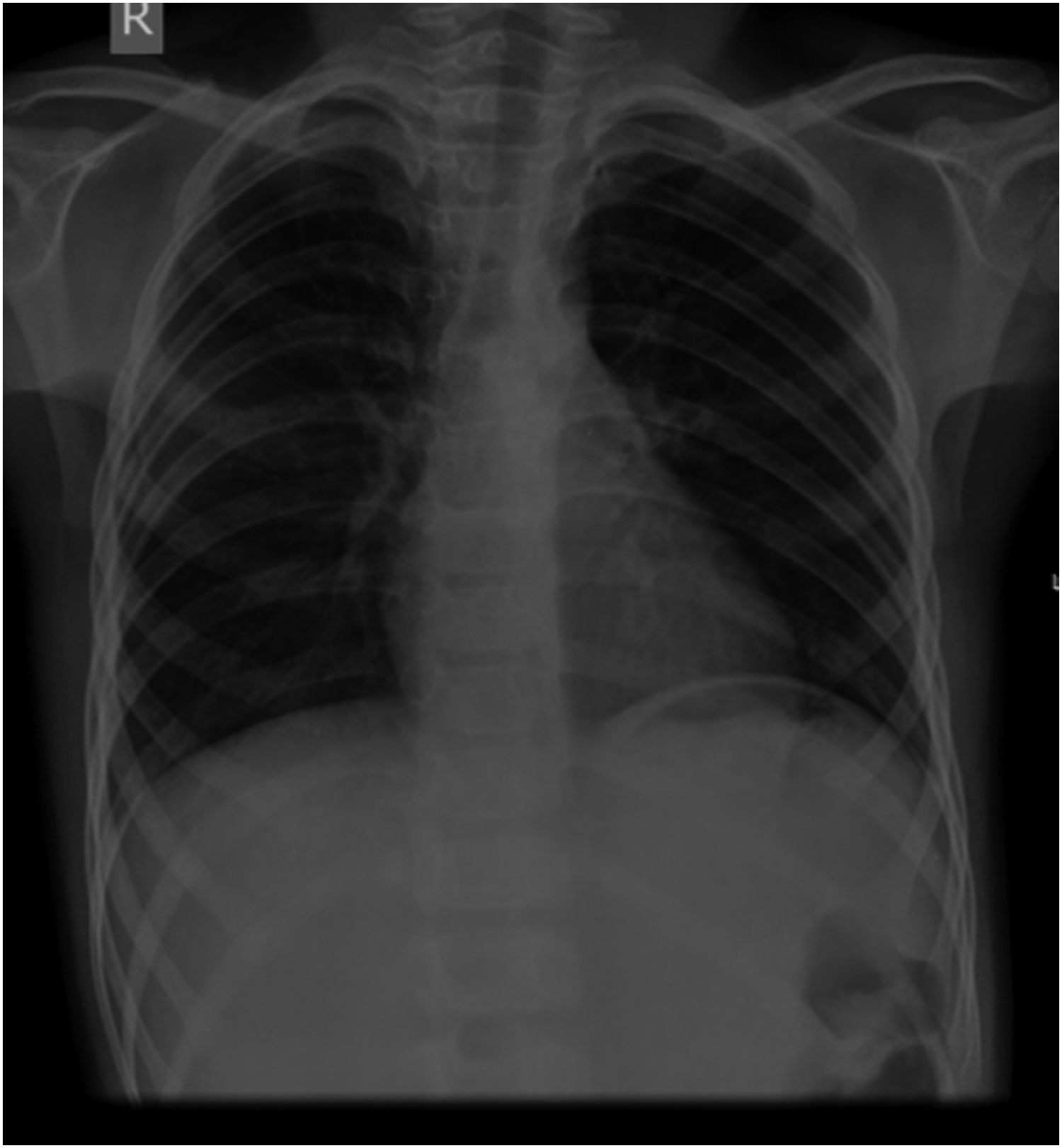
Follow-up chest X-ray after 72 hours in Kathmandu reveals resolution of the opacities.
HAPE is a medical emergency due to a noncardiogenic form of edema with elevated pulmonary artery pressures often seen in trekkers, mountaineers, and pilgrims who ascend (usually >3000 m) too high too fast (Basnyat and Murdoch, 2003). The pathophysiological mechanism of HAPE is primarily thought to be mechanical with patchy smooth muscle constriction of the pulmonary vasculature triggered by hypobaric hypoxia (Basnyat and Murdoch, 2003). Unlike, in the case of pneumonia where opacities or consolidation may remain for weeks on the chest X-ray, the prompt disappearance of the patchy opacities in our patient's chest X-ray within days is in keeping with HAPE (Zafren et al., 2009).
Reentry HAPE, which is a subset of HAPE, is a well-recognized life-threatening illness documented so far almost exclusively in the North and South Americas when people, who live at high altitude (>2500 m), return to their homes after a brief sojourn of days to months at a lower altitude setting (Scoggin et al., 1977; Hultgren and Marticorena, 1978; Niermeyer et al., 2009).
Reentry HAPE as described in our patient has not been reported in Sherpas or other people of Tibetan origin in Nepal or India. There has been only one report from Tibet (Wu, 2004). Children seem to be more susceptible to reentry HAPE than adults (Hultgren and Marticorena, 1978). A few explanations have been put forward to explain the lack of reentry HAPE in the Himalayan highlanders. Sevringhaus (1971) postulated that chronic hypoxia of high altitude causes increased muscularization of the pulmonary arterioles. This generates excessive pulmonary arteriole pressure on reascent to high altitude to which children may seem more predisposed to. Due to poorer adaptation to high altitude by the Andean native in comparison to the Tibetan-origin highlanders (Moore, 2001), this phenomenon may be more commonly seen in the South Americans. Another explanation suggests that reentry HAPE may be due to change in blood volume because prolonged exposure to high altitude results in increased blood volume (Wu, 2004). When the high altitude resident descends to lower altitude there is decrease in red cell mass resulting in compensatory rise in plasma volume which may predispose to pulmonary edema on return to high altitudes.
We suggest that another explanation for the rarity of this illness in Himalayas relative to that in South America (e.g., Peru where this phenomenon is well described) (Hultgren and Marticorena, 1978) is that historically a lack of roads in the high altitude Himalayas has largely prevented rapid reentry for high altitude residents sojourning after a temporary stay at lower altitudes. Lack of such roads may have previously protected children from reentry HAPE since rapid reascent is known to be an important risk factor in this disease. Now road building in the region, including the road recently completed from Besisahar to Manang, along which this patient traveled, may contribute to an increased prevalence of reentry HAPE (Reisman et al., 2017).
In addition, health workers at high altitudes in Nepal where reentry HAPE is unknown may select an alternate diagnosis as clearly happened in our patient. This may easily lead to a fatal outcome, as may have happened in this case had it not been for the prompt diagnosis and treatment by the HRA aid post doctors. Proper awareness regarding reentry HAPE in Himalayan high altitude natives needs to be created in high altitude population in this region, including in high altitude health workers. In this way, proper diagnosis and treatment with oxygen and rest or, if necessary, descent can be carried out promptly for effective treatment of reentry HAPE.
Footnotes
Acknowledgments
The authors sincerely thank Mr. Gobinda Bashyal of the HRA who helped with diagnosis, treatment, and helicopter rescue of the patient at the Manang aid post. The authors also thank the other staff members of the Himalayan Rescue Association and the Nepal International Clinic for generously helping out in the care of this patient.
Author Disclosure Statement
No competing financial interests exist.