
Abstract
Abstract
Horiuchi, Masahiro, Tadashi Uno, Junko Endo, Yoko Handa, and Tatsuya Hasegawa. Impact of sleeping altitude on symptoms of acute mountain sickness on Mt. Fuji. High Alt Med Biol. 19:193–200, 2018.
Aims:
We sought to investigate the factors influencing acute mountain sickness (AMS) on Mt. Fuji in Japan, in particular, to assess the effects of sleeping altitude, by means of a questionnaire survey. This study involved 1932 participants who climbed Mt. Fuji, and obtained information regarding sex, age, and whether participants stayed at the mountain lodges. The AMS survey excluded the perceived sleep difficulties assessed with the Lake Louise Scoring (LLS) system for all climbers.
Results:
The overall prevalence of AMS was 31.6% for all participants (LLS score ≥3 with headache, excluding sleep difficulties). A univariate analysis revealed that overnight stay at Mt. Fuji was associated with an increased prevalence of AMS, but that sex and age were not. For overnight lodgers, the mean sleeping altitude in participants with AMS was slightly higher than that in participants without AMS (p < 0.05). Moreover, participants who stayed above 2870 m were more likely to experience AMS than those who stayed below 2815 m (p < 0.001), but sex and age were not significantly associated with the probability of experiencing AMS.
Conclusions:
Staying overnight at a mountain lodge, especially one above 2870 m, may be associated with an increased prevalence of AMS on Mt. Fuji.
Introduction
P
Mt. Fuji, the highest mountain in Japan, with a height of 3776 m, has been registered as a UNESCO World Heritage site in 2013, and ca. 250,000 people, of various ages and both sexes, visit it annually (Ministry of the Environment, 2017). As previously described in the literature (Horiuchi et al., 2016), Mt. Fuji is unique for several reasons. First, there are 18 mountain lodges that can accommodate ∼4000 people, from the starting point of the climbing route (fifth station, at an altitude of 2305 m) to the top of Mt. Fuji (Fig. 1). Second, since roads and transportation networks are in a good condition from the base to the fifth station, almost all climbers reach the altitude of 2305 m from sea level within 1 hour using either their own vehicles or tour buses. These characteristics may be associated with a longer stay, including spending the night at high altitude, from the fifth station to the top of Mt. Fuji, and with a rapid ascent from sea level to the fifth station.
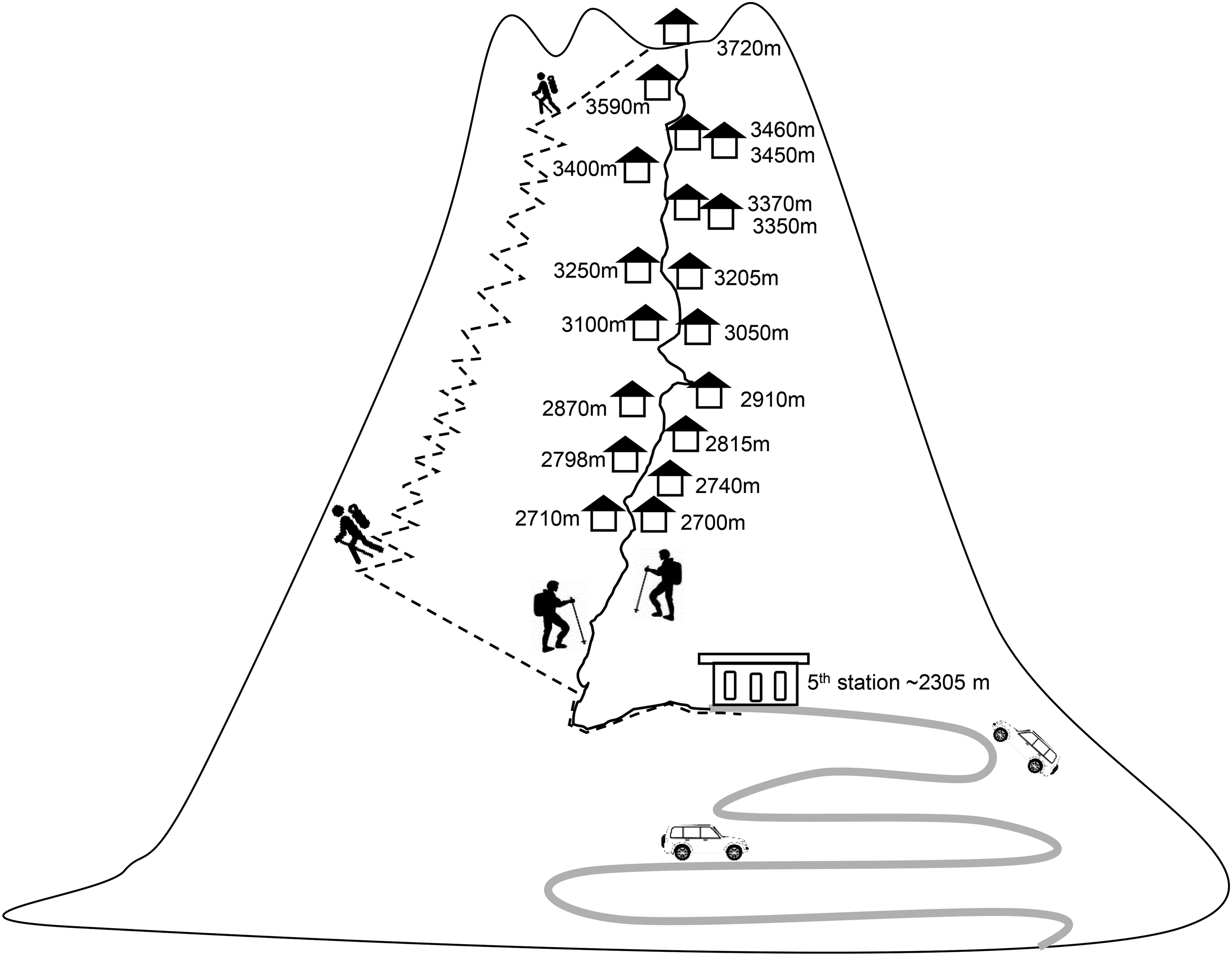
Illustration of locations of mountain lodges on the climbing road at Mt. Fuji. Gray bold line indicates driving road, black solid line indicates ascending road, and black dashed line indicates descending road.
Although AMS seems to be associated with several potential risk factors, sleeping altitude may be related to AMS. Indeed, a recent review suggested that, above ca. 2500 − 3000 m, individuals should not increase their sleeping altitude by 300–600 m (Luks et al., 2017). However, guidelines on the appropriate sleeping altitude that may reduce the risk of AMS are unclear. Recently, we have also reported that perceived worsening of sleep was associated with the prevalence of AMS in climbers who stayed overnight at a mountain lodge on Mt. Fuji (Horiuchi et al., 2016). However, in addition to the drawback of a relatively small sample size (ca. 300), data on several important aspects, such as sleeping altitude and detailed time schedule during mountain climbing, were lacking in that study. Therefore, we here investigated the effects of both sleeping altitude and rapid ascent, which are frequently experienced by climbers of Mt. Fuji, as well as the effects of demographic characteristics, that is, sex, age, and whether the climb was completed in a single day or included an overnight stay, on AMS in a larger population (ca. 2000) of climbers of Mt. Fuji. We hypothesized that participants who slept at higher altitude and/or climbed rapidly were more likely to develop AMS on Mt. Fuji.
Methods
Participants
This epidemiological study was approved by the ethics committee of the Mt. Fuji Research Institute in Japan, in accordance with the Declaration of Helsinki. It was conducted among climbers descending from Mt. Fuji, who had reached the fifth station (altitude: 2305 m). The study survey was conducted in the month of August in three consecutive years (2014–2016). Participants were surveyed between 8:00 a.m. and 1:00 p.m., and we confirmed that all climbers had reached the fifth station through their own vehicles or a tour bus, and that they had begun their descent during the early hours of the morning. We chose to use the trailhead sign, which could be reached in ∼20 minutes by walking from the fifth station, as the survey spot, as we sought to avoid volunteer bias against participants who were eager to leave the train and/or who were in a more recreational mood. To avoid several biases, that is, duplicate survey responses, or vague or rushed responses, we confirmed the following criteria for each participant: (1) whether participants responded to this survey for the first time and (2) whether they had sufficient time to complete the questionnaire carefully. After providing a detailed explanation of the study, informed consent was obtained from each participant. We included all participants irrespective of whether they summited, given the main aim of this study. Notably, on Mt. Fuji, mountain lodges are present only on the ascending road, and no lodges are available on the descending road. We confirmed that all participants stayed at a mountain lodge during their ascent and stayed there for only one night.
Questionnaires
All participants responded with the following information: (1) AMS scores using the Lake Louise Scoring (LLS) system, (2) single-day climbers or overnight lodgers, (3) sex, and (4) age. In addition, climbers who stayed at a mountain lodge were questioned regarding (5) their sleeping altitude (altitude of the mountain lodge) and (6) their detailed climbing schedule, that is, the departure time at the fifth station, arrival time at the lodge, departure time at the lodge, and arrival time at the top of Mt. Fuji. A total of 1644 participants stayed overnight at a mountain lodge. All participants reported their sleeping altitude; however, 756 individuals were excluded from further analysis of the climbing schedule because of a lack of information, due to recall issues, as reported in their self-assessment.
AMS assessment
All participants were surveyed using four of the five subscales, that is, “headache,” “gastrointestinal upset,” “fatigue/weakness,” and “dizziness/lightheadedness,” with exclusion of the “perceived sleep difficulty index” subscale. AMS was diagnosed based on a recent gain in altitude, at least several hours at the new altitude, and the presence of headache and at least one of the following symptoms: gastrointestinal upset (i.e., anorexia, nausea, or vomiting), fatigue or weakness, dizziness or lightheadedness, and difficulty sleeping with total LLS score ≥3. It should be noted that the perceived sleep difficulty item was excluded in comparisons of single-day climbers and overnight lodgers (Roach et al., 1993). In addition, we asked participants to respond in terms of the worst symptoms of AMS experienced during climbing.
Sample size
We calculated the required sample size according to the following equation:
where N is the number of climbers on Mt. Fuji, e is the margin of error, z is the confidence level as a z-score, and p is the percent value.
We used 250,000 as N, 3% as e, and 95 as z; we used 0.5 as the value for p, this is the value recommended when a survey is being conducted for the first time (Sample Size Calculator, 2017). We estimated 1063 participants as the required sample size. We collected 1932 valid responses from all participants, and 1644 from overnight lodgers. Furthermore, we obtained a detailed climbing schedule from the subset of participants (n = 888). In this case, this obtained sample size was equivalent to an e of 4% and a z of 95%. Thus, the valid responses obtained in this study had sufficient power to predict the prevalence and severity of AMS on Mt. Fuji. Moreover, our sample size (n = 2267) was much larger than those typically found in previous epidemiological studies (n = 130–827 participants) (Hackett et al., 1976; Maggiorini et al., 1990; Basnyat et al., 2000; Schneider et al., 2002; Vardy et al., 2005, 2006; Mairer et al., 2009, 2010), although one previous study had over 3000 participants (Honigman et al., 1993).
Statistical analysis
Statistical analysis was performed using Sigma Stat 3.5 software (Systat Software, Inc., Chicago, IL), and the free statistical software “R” (R for Windows, ver. 3.2.3). In the univariate analysis of those with AMS and those without AMS, a chi-squared test was used to compare categorical variables (i.e., staying overnight or not, sex, and sleeping above or below a given altitude), and an unpaired t-test was used to compare continuous variables (i.e., age, actual sleeping altitude, and detailed schedule during climbing). The Mann−Whitney U and Kruskal−Wallis tests were used to analyze the effects of staying overnight at the mountain lodge, sex, age, and sleeping altitude on the severity of AMS in participants with AMS. The LLS scores in participants with AMS are represented as means ± standard deviations (SDs) and as medians with interquartile ranges (IQRs), that is, 25 and 75 percentile. For the results from a chi-square test with a cross-tabulation table of two rows and two columns, and for those from a logistic analysis, we also present the odds ratio (OR) for the presence of AMS. We also show effect size, which is a quantitative measure of the strength of a phenomenon and is independent of sample size. We determined with Cohen's d-test for continuous variables and Cramer's V-test for categorical variables.
For the multivariate analysis, multiple logistic regression analysis was used to identify factors related to the prevalence of AMS (presence/absence; dependent variable). As independent variables, we used the following: (1) single day or overnight stay, (2) sex, (3) age, (4) sleeping altitude, and (5) detailed time schedule during climbing. We standardized all variables using the following equation:
Here, nominal variables, that is, “single day” or “overnight stay” and “male” or “female,” were defined as “0” or “1.” Thus, the mean value and the SD of all standardized values were 0 and 1, respectively.
Results
According to data from the Japan Meteorological Agency, the mean ambient temperature at the summit of Mt. Fuji was 5.9°C (range: 2.0°C–8.5°C) and the relative humidity was 79.7% (range: 49% −99%) on days in which the survey was conducted.
We obtained 2267 questionnaire sheets from participants who were older than 20 years. Of these, 335 were excluded from further analysis because of missing information or the presence of certain medications, such as acetazolamide, dexamethasone, or analgesics, which may influence AMS symptoms. We obtained valid responses from 1932 (85.2%) respondents. Of them, 154 (13 of the single-day climbers and 141 of the overnight lodgers) did not summit Mt. Fuji. The reasons included (1) diagnosis of AMS, (2) bad weather, and (3) lack of time for tour buses. Among all participants, 31.6% met our definition of AMS.
The number of participants with or without AMS and the severity of AMS in each category for all climbers are shown in Table 1. In terms of the prevalence of AMS, participants who stayed at mountain lodges were more likely to experience AMS (p = 0.046). There were no significant differences in the distribution of participants between males and females, and in mean age between participants with or without AMS (p > 0.05). In terms of the severity of AMS for all the participants who claimed symptoms of AMS, no differences were observed between single-day climbers and overnight lodgers or between male and female participants with AMS (p > 0.05).
Values of age and mean AMS score are means ± standard deviations (SDs).
ORs quantify how strongly AMS was present in overnight lodgers and in females. The criteria used for diagnosing AMS were as follows: total AMS scores ≥3, with headache, but excluding perceived sleep items, so that the maximum score was 12. The data on severity of AMS (mean AMS score and IQR of AMS score) were obtained only from participants with AMS in each category, that is, “single day and overnight,” “male and female,” and “age.”
Indicates that there were significantly fewer single-day climbers with AMS than expected from the residual analysis.
Indicates that there were significantly more overnight lodgers with AMS than expected from the residual analysis.
AMS, acute mountain sickness; IQR, interquartile range; 25% and 75% indicate the 25th percentile and 75th percentile, respectively; OR, odds ratio; 95% CI, 95% confidential interval; —, not applicable.
The distribution of sleeping altitudes for participants who stayed over in mountain lodges and the ratio of participants with AMS at each sleeping altitude are shown in Figure 2. It appears that the numbers of people who stayed at an altitude between 3205 and 3450 m were more intensely concentrated than at other altitudes. Moreover, the proportion of participants with AMS at each altitude was similar to the mean AMS prevalence value (32.5%; dashed horizontal line in Fig. 2) in participants who stayed above 2870 m, whereas this proportion was markedly lower than the mean value among participants who stayed below 2815 m (line graph in Fig. 2).
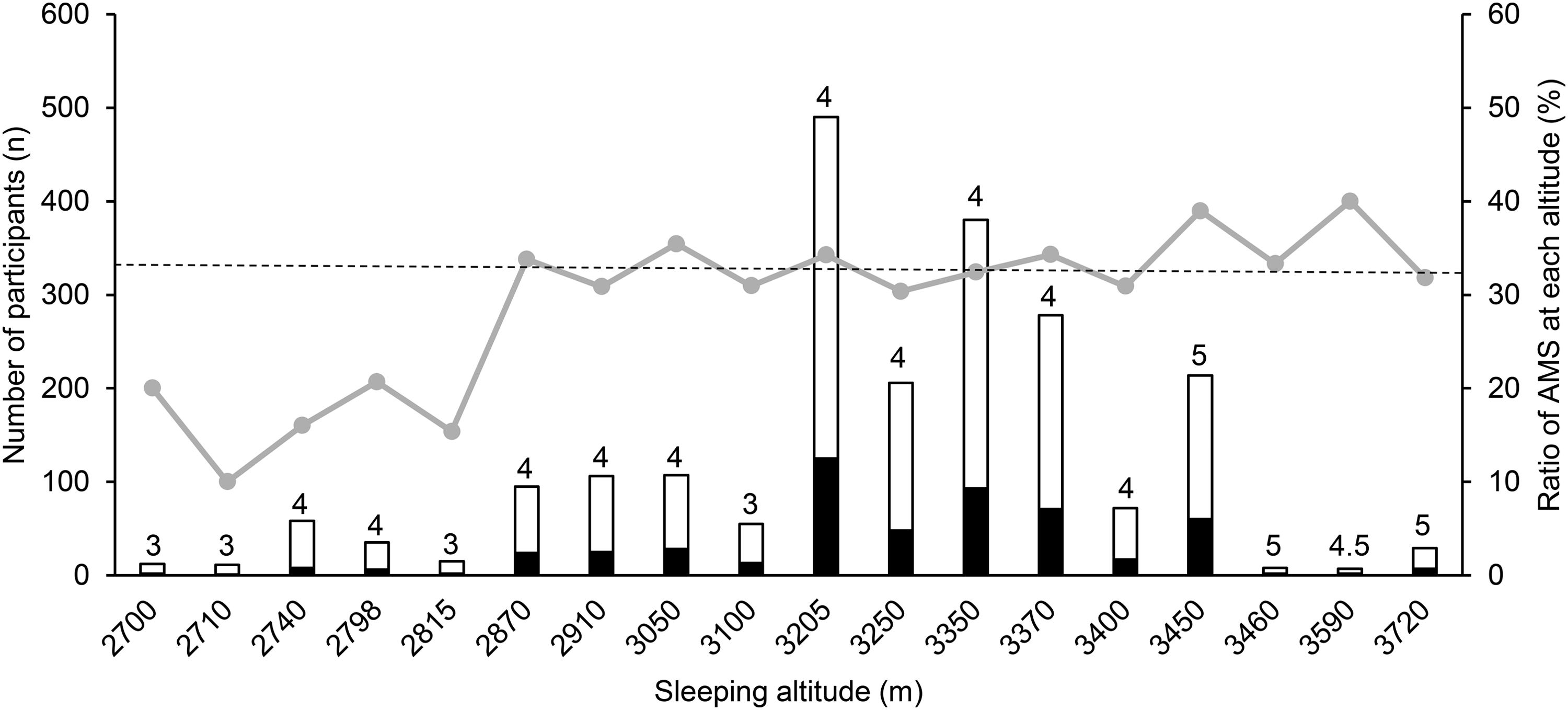
The number of participants at each mountain lodge (bar graph) and ratio of participants with AMS at each altitude (line graph). White bars indicate participants without AMS and black bars indicate those with AMS. Numbers above the white bar graph indicate median values at each altitude with AMS. The criteria for AMS is a total score ≥3 with headache, but excluding the sleep item. The dashed line indicates the prevalence rate of AMS in all overnight lodgers (n = 1644). AMS, acute mountain sickness.
The number of participants with or without AMS and the severity of AMS in each category for overnight lodgers are shown in Table 2. The mean sleeping altitude in participants with AMS was slightly higher than that in participants without AMS (p < 0.05). Moreover, the participants were divided into two groups depending on the different sleeping altitudes, that is, below 2815 m or above 2870 m. Participants who stayed above 2870 m were more likely to experience AMS than those who stayed below 2815 m (p < 0.001). However, there was no significant effect of sex or age (p > 0.05 for both) on the prevalence of AMS among overnight lodgers.
Values of age, sleeping altitude, and mean AMS score are means ± SDs.
Means and IQRs of AMS score are shown as in Table 1. ORs quantify how strongly AMS was present in females and in participants who stayed above 2870 m.
Indicates that unpaired t-tests revealed significant differences between participants with and without AMS.
Indicates that there were significantly fewer participants with AMS than expected from the residual analysis.
Indicates that there were significantly more participants with AMS than expected from the residual analysis.
Table 3 shows the detailed time schedule during climbing in the subset of overnight lodgers between participants with or without AMS. Ascending speed on day 2 in participants with AMS was slightly slower than in those without AMS (p < 0.05), while no significant differences were observed for other variables (all p > 0.05).
Values are means ± SDs.
Indicates significant differences between participants with and without AMS. Ascent speed was calculated by following equation: Ascent speed (m/h) = Acquired altitude on day 1 or 2 (m)/Ascending time on day 1 or 2 (minutes) × 60 min/h.
For all participants (n = 1932), overnight stay at a mountain lodge was found to predict a higher prevalence of AMS (Table 4). Similarly, for only overnight lodgers (n = 1644), a higher sleeping altitude was determined to predict a greater prevalence of AMS (Table 4). For a subset of overnight lodgers (n = 888), being female was found to predict AMS, while other factors were not found to predict AMS (Table 4). Mean LLS scores for participants with AMS were similar when examining all participants (4.5 ± 1.7), overnight lodgers (4.5 ± 1.7), and the subset of overnight lodgers (4.5 ± 1.6). Furthermore, these subgroups had similar IQRs for AMS scores (3–5; median: 4).
Total staying time means the total time from the start of ascending at the fifth station to the start of descending from the summit. Speed on day 1 or 2 was calculated using the following equation: Speed on day 1 (or 2) = (Acquisition altitude on day 1 [or 2])/(the time required on day 1 [or 2]) × 60.
Discussion
In this study, we hypothesized that higher sleeping altitude and/or rapid ascent is related to the prevalence of AMS among climbers of Mt. Fuji. Among overnight lodgers, those who stayed over at a mountain lodge at a higher altitude were more likely to experience AMS. Moreover, based on the analysis of a subset of participants, rapid ascent may not affect symptoms of AMS. We found that an overnight stay was related to an increased prevalence of AMS, irrespective of sex and age (Table 1). Generally, symptoms of AMS are observed 6 − 12 hours after rapid ascent to a new high altitude, and the severity of AMS symptoms peaks during the initial 1–2 days after ascent (Berghold, 1998). Therefore, it is possible that overnight lodgers were exposed to high altitude longer compared to single-day climbers. However, in addition to the marginal significance, for example, an OR of 1.34 and a narrow 95% confidence interval of 1.01–1.78 (Table 1), at this stage, we do not have direct evidence to account for this hypothesis. Further studies are required.
Effect of sleeping altitude
It has previously been established that sleeping altitude should not be increased by more than 300–500 m per day to prevent AMS (Bartsch et al., 2004; Luks, 2012). Moreover, the proportion of participants with AMS at each sleeping altitude was higher (>2870 m) or lower (<2815 m) than the mean prevalence of AMS in overnight lodgers (32.5%) in this study. Thus, we detected the cutoff point for sleeping altitude as ca. 2815 m. Our results indicated that increases in sleeping altitude of more than about 500 m may increase the prevalence of AMS among climbers of Mt. Fuji about 2.5-fold (Table 2), which is consistent with the findings of previous studies (Bartsch et al., 2004; Luks, 2012). It is plausible that sleeping at higher altitudes causes hypoxemia, and several studies have found that hypoxemia is associated with AMS (Erba et al., 2004; Koehle et al., 2010; Nespoulet et al., 2012; Nussbaumer-Ochsner et al., 2012). Recently, we reported that arterial oxygen saturation gradually decreased when sleeping overnight at a high altitude, ca. 3776 m, and did not recover by the morning, suggesting that hypoxemia was exacerbated during sleep (Horiuchi et al., 2017). In addition, previous studies have demonstrated that impaired sleep quality is related to the prevalence and severity of AMS (Burgess et al., 2004; Nespoulet et al., 2012; Nussbaumer-Ochsner et al., 2012). Together, our results may have important clinical implications, such as a pertinent choice of sleeping altitude for reducing the prevalence and severity of AMS among climbers of Mt. Fuji.
Effect of rapid ascent
It is known that a rapid ascent to higher altitude is one of the most important risk factors for developing AMS (Honigman et al., 1993), while a slow ascent reduces the risk of high-altitude illness (Hackett and Roach, 2001; Bloch et al., 2009). Considering these facts, we investigated the detailed time schedule in a subset of overnight lodgers and found no effect of climbing speed on days 1 or 2, or of longer exposure to a high altitude. These results did not agree with the findings of previous studies (Honigman et al., 1993; Schneider et al., 2002). Unfortunately, our survey comprised a recall model, rather than a real-time assessment. Thus, we could not obtain a detailed time-schedule from all participants and were dependent on data based on the participants' memory. It remains possible that a slower ascending speed was due to the development of AMS, while participants who ascended more rapidly did not have AMS. It should be noted that the risk of driving from sea level to the fifth station at 2305 m (i.e., the starting point) within ∼1 hour may outweigh all other factors, including climbing schedule, in predicting the prevalence of AMS. However, we must acknowledge that these explanations are highly speculative. To clarify the effect of the detailed climbing schedule on AMS, a global positioning system device should be used in future studies.
Effect of demographic issues (sex and age)
Numerous previous studies showed reduced effects of sex (Hackett et al., 1976; Maggiorini et al., 1990; Schneider et al., 2002; Vardy et al., 2006; Wang et al., 2010) and age (Schneider et al., 2002; Vardy et al., 2005; Wang et al., 2010) on AMS, but some studies found a higher risk of AMS in women (Honigman et al., 1993) or men (Johnson and Rock, 1988), and in younger adults (Hackett et al., 1976; Honigman et al., 1993) or the elderly (Maggiorini et al., 1990). Our results suggest that sex and age differences are of little importance in terms of the prevalence and severity of AMS among climbers of Mt. Fuji apart from a subset of overnight lodgers (n = 888), for whom the multiple regression analysis showed a higher prevalence in women (Table 4). These results may be confusing, but it should be noted that these results were obtained from only a subset of our participants and we found no influence of sex on the prevalence of AMS among all participants (n = 1932). Although future studies may be necessary, we could not completely rule out any statistical errors, such as type I errors. Moreover, as most of these studies were conducted for different ethnic groups, further explanation is difficult; however, a previous study demonstrated that sex and age differences did not affect the prevalence of AMS among Taiwanese (Asian ethnicity) climbers of Jude Mountain (Wang et al., 2010). Therefore, although future studies are required, sex and age differences were of little importance in terms of the prevalence and severity of AMS in the Japanese population climbing Mt. Fuji.
Limitations
There are several limitations to interpreting our results. First, our survey study was a recall model, not a real-time assessment. Thus, we could not clarify when the highest scores were observed in each participant, such as before or after sleeping at mountain lodges, or at the top of Mt. Fuji. Similarly, participants might have had different symptoms at different time points (e.g., only headache at one point, but dizziness without headache at another point). Although we carefully explained the definition of AMS and asked participants to respond based on the AMS criteria, recall bias might have affected our data. Moreover, as we surveyed climbers between 8:00 a.m. and 1:00 p.m. at the fifth station, we might have missed some climbers who descended before or after the survey window. Although future studies are required, our sample size of ∼2000 climbers was quite large. Second, we did not assess sleep quality directly. Although the LLS subscales include a subjective sleep quality index, a recent study (Anderson et al., 2017) of high-altitude sleep (∼3200 m) reported no significant differences in sleep efficiency, desaturation, or apnea-hypopnea index scores between people who reported good sleep on the LLS sleep quality subscale and those who reported poor sleep. This indicates that subjective assessments on the LLS sleep difficulty subscale may not reflect actual sleep conditions, so we did not use that subscale. Thus, future studies should implement a more robust sleep questionnaire, for example, the Groningen Sleep Questionnaire and/or direct polysomnography assessments. Third, due to the relatively small numbers of questionnaire items, the effect of other potential candidate factors, such as a history of previous AMS, migraine (Richalet et al., 2012; Canouï-Poitrine et al., 2014; Vinnikov et al., 2014), body mass index (obesity) (Beidleman et al., 2013), physical activity level (Beidleman et al., 2013), physical exertion (Roach et al., 2000), current smoking status (Beidleman et al., 2013; Vinnikov et al., 2014), cardiorespiratory responses to hypoxia (Oliver et al., 2012; Richalet et al., 2012; Canouï-Poitrine et al., 2014), and hydration status, including drinking habits (Mairer et al., 2009; Oliver et al., 2012), which have been investigated previously, on AMS in this population remains uncertain. Although future studies that include these items are warranted, our results clearly demonstrated that sleeping altitude may play an important role in increasing the prevalence and severity of AMS.
Conclusions
Our results suggested that participants who stayed overnight at a mountain lodge, in particular, above 2870 m (i.e., increased their sleeping altitude by more than about 500 m) are more likely to develop AMS. These results may be informative for populations who plan to climb and stay overnight at Mt. Fuji, particularly from the viewpoint of making appropriate choices regarding their sleeping altitudes and climbing tactics.
Footnotes
Acknowledgments
The authors thank all participants for their time and effort. We also thank Dr. Taisuke Yasuda, Dr. Atsuhi Owaki, and Dr. Sachiko Kikuchi for their suggestion regarding the statistical analyses. We also thank the students in Dr. Kiyotatsu Yamamoto's seminar at Iwate University for their assistance of collecting data. This study was supported by a Grant-in-Aid of the Japan Society for the Promotion of Science (No. 26440268 to M.H., Japan).
Author Disclosure Statement
No competing financial interests exist.