
Abstract
Abstract
Summerfield, Douglas T., Kirsten E. Coffman, Bryan J. Taylor, Amine N. Issa, and Bruce D. Johnson. Exhaled nitric oxide changes during acclimatization to high altitude: a descriptive study. High Alt Med Biol. 19:215–220, 2018.
Aims:
This study describes differences in the partial pressures of exhaled nitric oxide (PeNO) between subjects fully acclimatized (ACC) to 5300 m and those who have just arrived to high altitude.
Methods:
PeNO was determined in eight subjects newly exposed and nonacclimatized (non-ACC) to high altitude and compared with that in nine subjects who had ACC to high altitude for 1 month. In addition, systolic pulmonary artery pressure (sPAP) and arterial oxygen saturation (SaO2) were measured in all participants. These measurements were repeated in the non-ACC group 5 and 9 days later.
Results:
PeNO levels on day 1 were significantly higher in the non-ACC versus ACC cohort (8.7 ± 3.5 vs. 3.9 ± 2.2 nmHg, p = 0.004). As the non-ACC group remained at altitude, PeNO levels fell and were not different when compared with those of the ACC group by day 9 (5.9 ± 2.4 vs. 3.9 ± 2.2 nmHg, p = 0.095). Higher sPAP was correlated with lower PeNO levels in all participants (R = −0.50, p = 0.043). PeNO levels were not correlated with SaO2.
Conclusions:
As individuals acclimatized to high altitude, PeNO levels decreased. Even after acclimatization, PeNO levels continued to play a role in pulmonary vascular tone.
Introduction
I
Pulmonary vasculature production of NO is catalyzed by nitric oxide synthases, both endothelial eNOS and inducible iNOS. These enzymes oxidize
Prior groups have found that HAPE-susceptible subjects who sojourn to high altitude show lower eNO levels and higher systolic pulmonary artery pressures (sPAPs) than controls (Duplain et al., 2000). Furthermore, higher sPAP and lower eNO were associated with the formation of pulmonary edema in a subset of HAPE-susceptible subjects, potentially suggesting increased hypoxic pulmonary vasoconstriction in these individuals (Duplain et al., 2000). The reduced level of eNO seen in HAPE-prone individuals is the basis for treatment of HAPE with inhaled NO (iNO), which has been shown to improve decreased oxygen saturation associated with HAPE (Scherrer et al., 1996). Interestingly, the administration of exogenous iNO decreased PAPs and increased arterial oxygen saturations (SaO2) only in HAPE-prone individuals exposed to hypobaric hypoxia. In non-HAPE-prone subjects, it actually worsened oxygenation (Scherrer et al., 1996).
Although changes in sPAP and eNO have been well described with ascent to high altitude, they have not been monitored as subjects acclimatize. Thus, it is not known what, if any, further changes occur during adaptation to high altitude. Our aim was to investigate associations between eNO, sPAP, Hgb, and SaO2 during acclimatization to hypobaric hypoxia.
Methods
Subjects
Seventeen healthy nonsmoking adult lowlanders (two female) with no history of cardiorespiratory or metabolic disease participated in the study. Each participant gave written informed consent after being provided a detailed description of the study requirements. The experimental procedures were approved by the Mayo Clinic Institutional Review Board and were performed in accordance with the ethical standards of the Declaration of Helsinki. All study participants were prohibited from prophylactic administration of any medication to aid altitude acclimatization (e.g., sildenafil and acetazolamide). Moreover, no subject required emergent pharmaceutical treatment (e.g., dexamethasone) for high-altitude illness.
Expedition details and experimental procedures
All experimental procedures were performed at Mount Everest base camp (5300 m). To reach base camp, each participant traveled to Kathmandu, Nepal, (1400 m) before being transported by airplane to Lukla, Nepal (2860 m). From Lukla, the participants completed an 8- to 10-day hike at progressively increasing altitudes to reach base camp. The 17 participants were separated into two groups: Group 1 (n = 9, two female; acclimatized, “ACC”) arrived and stayed at base camp for ∼1 month before the arrival of Group 2 (n = 8, 0 female; nonacclimatized, “non-ACC”). Within 24 hours of arrival of the non-ACC group to base camp, eNO, sPAP, SaO2 (Nonin Medical, Inc., Plymouth, MN), and Hgb (Abbott iSTAT, Princeton, NJ) were measured. In addition, eNO and sPAP were measured on day 5 and day 9 at base camp in non-ACC.
Exhaled nitric oxide
eNO was measured in triplicate in parts per billion using a hand-held electrochemical detector (NIOX MINO Aerocrine, New Providence, NJ) according to standard procedures (Silkoff, 2005). In brief, subjects inhaled NO-free air to total lung capacity before exhaling for ∼10 seconds against a counter pressure of 5–20 cmH2O. By allowing closure of the soft palate, this technique isolates the small airways and prevents the measurement of NO from the nasal cavity (Silkoff et al., 1997, 1998; Pietropaoli et al., 1999). At the time of the study, all subjects were nonsmokers. In addition, each participant abstained from eating nitrogen-enriched foods for at least 3 hours before each measure of eNO.
When reporting eNO at altitude, it is necessary to convert eNO (ppb) to partial pressure of eNO (PeNO, nmHg) at normal temperature and pressure conditions so that eNO values can be accurately compared across studies and altitudes. Therefore, the correction factor determined by Hemmingsson et al. (2009) for the NIOX MINO at an altitude of 5000 m was applied, followed by conversion from ppb to nmHg, as follows:
For ease of comparability with other reported data, it should be noted that 1 nm Hg = 10−6 mm Hg = 1.333 mbar.
Systolic pulmonary artery pressure
sPAP was estimated from the peak velocity of tricuspid regurgitation (TRVMAX) using a modified Bernoulli equation as described previously (Yock and Popp, 1984). With participants in the left lateral supine position, the TR jet was located using 2D-color Doppler echocardiography in the four-chamber view. To determine TRVMAX, the continuous wave sampler was positioned within and parallel to the regurgitation jet and sPAP was computed as 4 × TRVMAX + right atrial pressure (RAP). RAP was estimated from the ratio between minimum inferior vena cava (IVC) diameter during a maximal sniff maneuver and maximum IVC diameter during normal respiration (Rudski et al., 2010). TRVMAX and IVC dimensions were measured in triplicate in each participant at each time point.
Statistical analyses
Independent samples t-test was used to compare absolute measures of PeNO, sPAP, and SaO2 between ACC versus non-ACC on day 1 at base camp. One-way repeated measures ANOVA was used to compare absolute measures of PeNO and sPAP across time (base camp day 1 vs. day 5 vs. day 9) in the non-ACC group. After significant main effects, planned pairwise comparisons were made using the Bonferroni method. In addition, Pearson's product–moment correlation coefficient (r) was computed to assess the relationships between PeNO and either sPAP, SaO2, or Hgb. The acceptable type I error was set at p < 0.05. Data are expressed as group means ± SD. Statistical analyses were performed using SPSS version 22.0 for Windows (IBM, Armonk, NY).
Results
Effect of high altitude on PeNO, sPAP, and SaO2
Upon arrival at base camp, group mean PeNO was greater in the non-ACC versus the ACC group (Fig. 1 and Table 1). Conversely, neither sPAP nor SaO2 was different between the non-ACC and ACC groups (Table 1). In the non-ACC group, PeNO was not different on day 5 but significantly lower on day 9 vs. day 1 at base camp (Table 1). Indeed, after 9 days at base camp, PeNO was not different in the non-ACC group compared with that in the ACC group 9 days prior (5.9 ± 2.4 vs. 3.9 ± 2.2 ppb, p = 0.095).
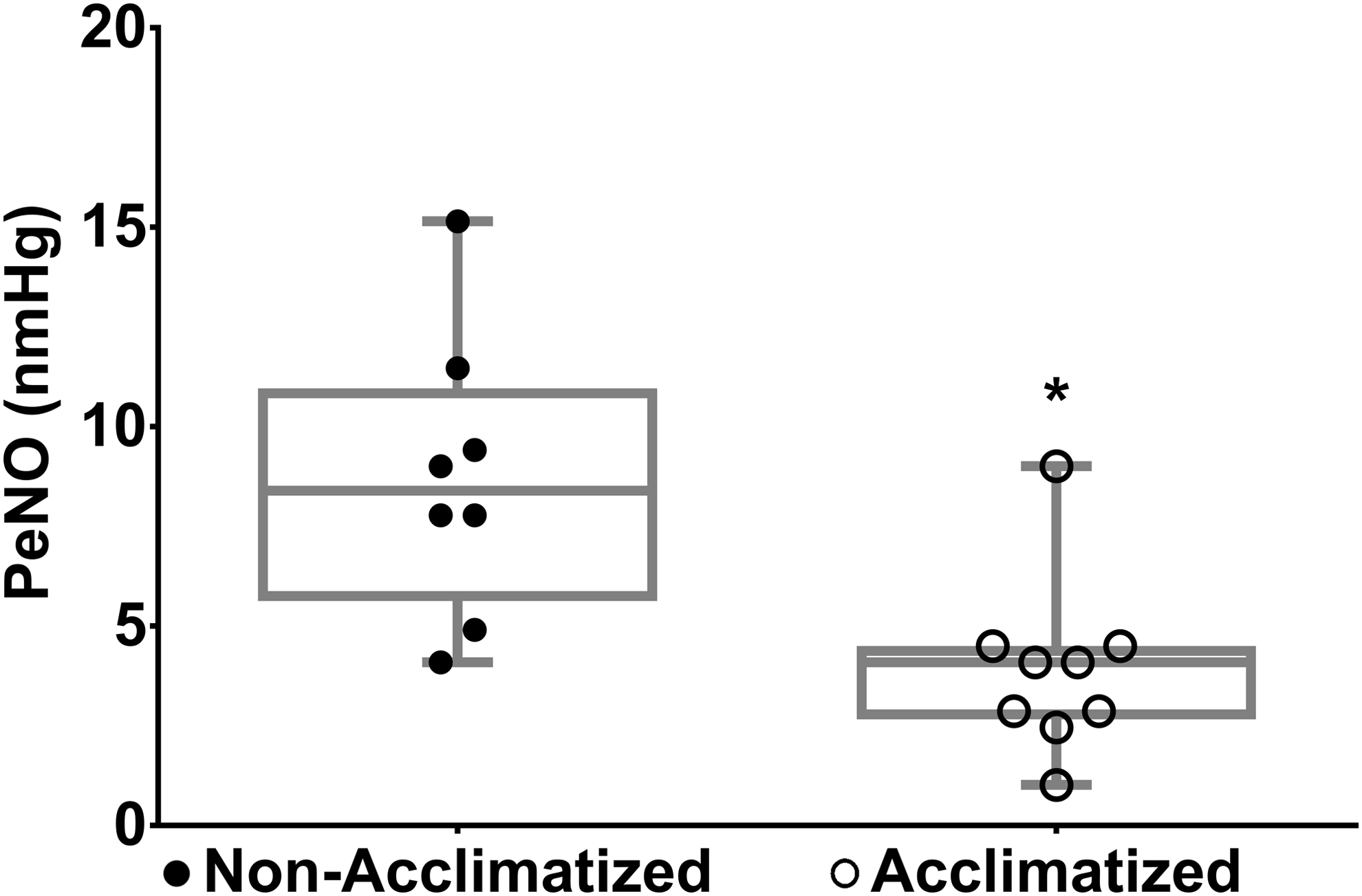
Individual PeNO levels for Non-ACC and ACC individuals at 5300 m at day 1 of arrival of the non-ACC cohort. Non-ACC individuals had greater PeNO levels versus the ACC cohort (8.7 ± 3.5 vs. 3.9 ± 2.2 nmHg, p = 0.004) when measured immediately upon arrival to altitude. 1 nm Hg = 10−6 mm Hg = 1.333 mbar. *p < 0.05 vs. Non-ACC. Non-ACC, nonacclimatized; ACC, acclimatized; PeNO, partial pressure of exhaled nitric oxide.
Significant effect of time, p = 0.032 (day 9 vs. day 1, p = 0.026).
Non-ACC, nonacclimatized; ACC, acclimatized; PeNO, partial pressure of exhaled nitric oxide; sPAP, systolic pulmonary artery pressure; SaO2, daytime oxygen saturation.
Associations between PeNO, sPAP, SaO2, and Hgb
Previous studies have also found a correlation between sPAP and PeNO levels. Figure 2 shows this relationship for all subjects combined. Indeed, higher PeNO levels were significantly correlated with lower sPAP (Fig. 2; R = −0.50, p = 0.043).
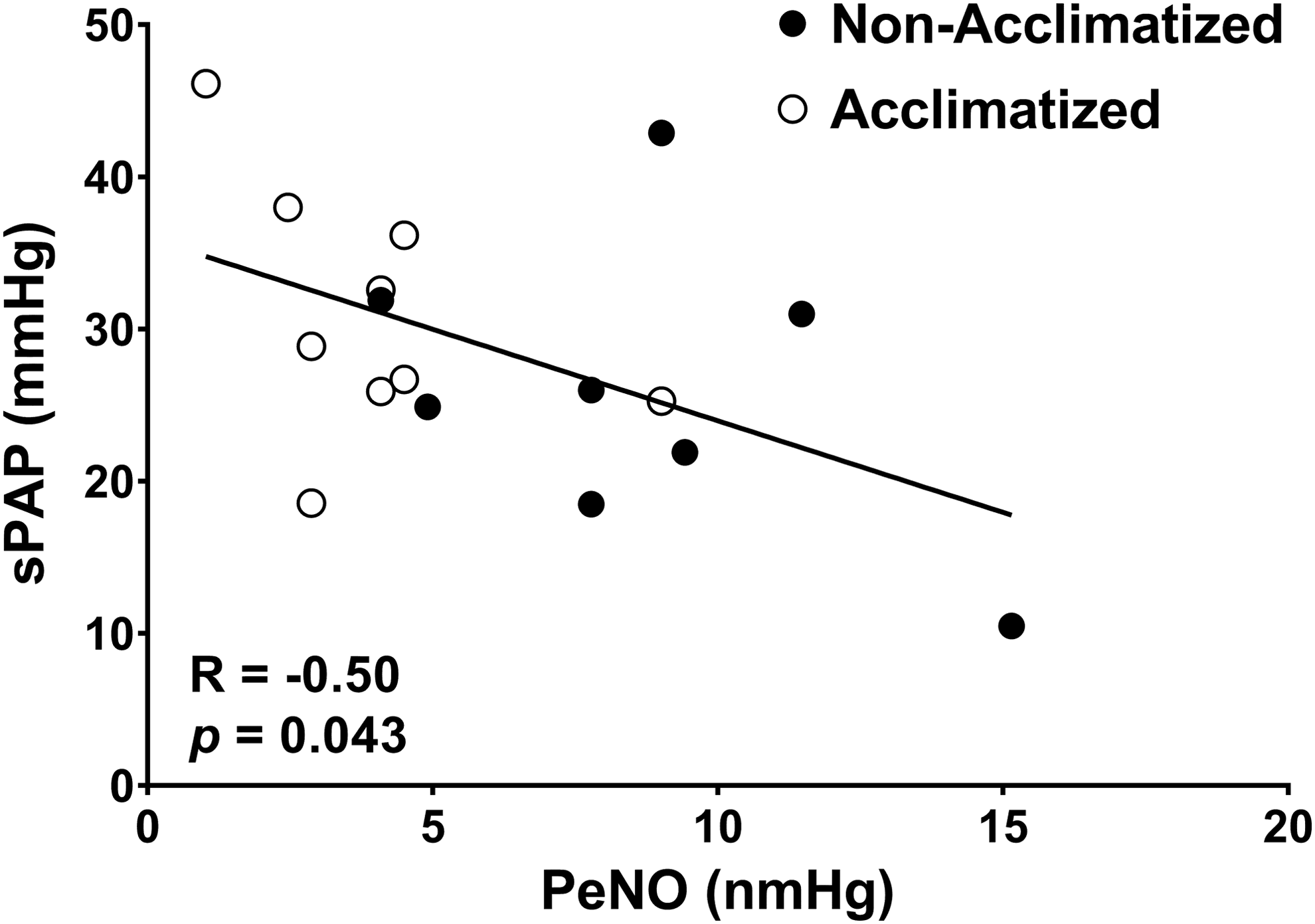
sPAP as a function of PeNO for all participants at day 1 of arrival of the non-ACC cohort. Similar to previous studies (8), subjects demonstrated a significant inverse relationship between PeNO levels and sPAP after exposure to high altitude. These data suggest that PeNO levels continue to play a role in pulmonary vascular tone even after acclimatization. 1 nm Hg = 10−6 mm Hg = 1.333 mbar. sPAP, systolic pulmonary artery pressure.
PeNO levels were also compared with resting daytime SaO2 for both groups (Fig. 3). There were no correlations between PeNO levels and daytime SaO2, in either the non-ACC or ACC groups, or combined. However, individual performances were also recorded. Interestingly, it was noted that the team member in the ACC group with the highest PeNO level and highest corresponding SaO2 was able to subsequently summit to a height of 8848 m without oxygen. Conversely, the member in the ACC group who had the lowest PeNO and the corresponding lowest SaO2 was unable to successfully complete the climb.
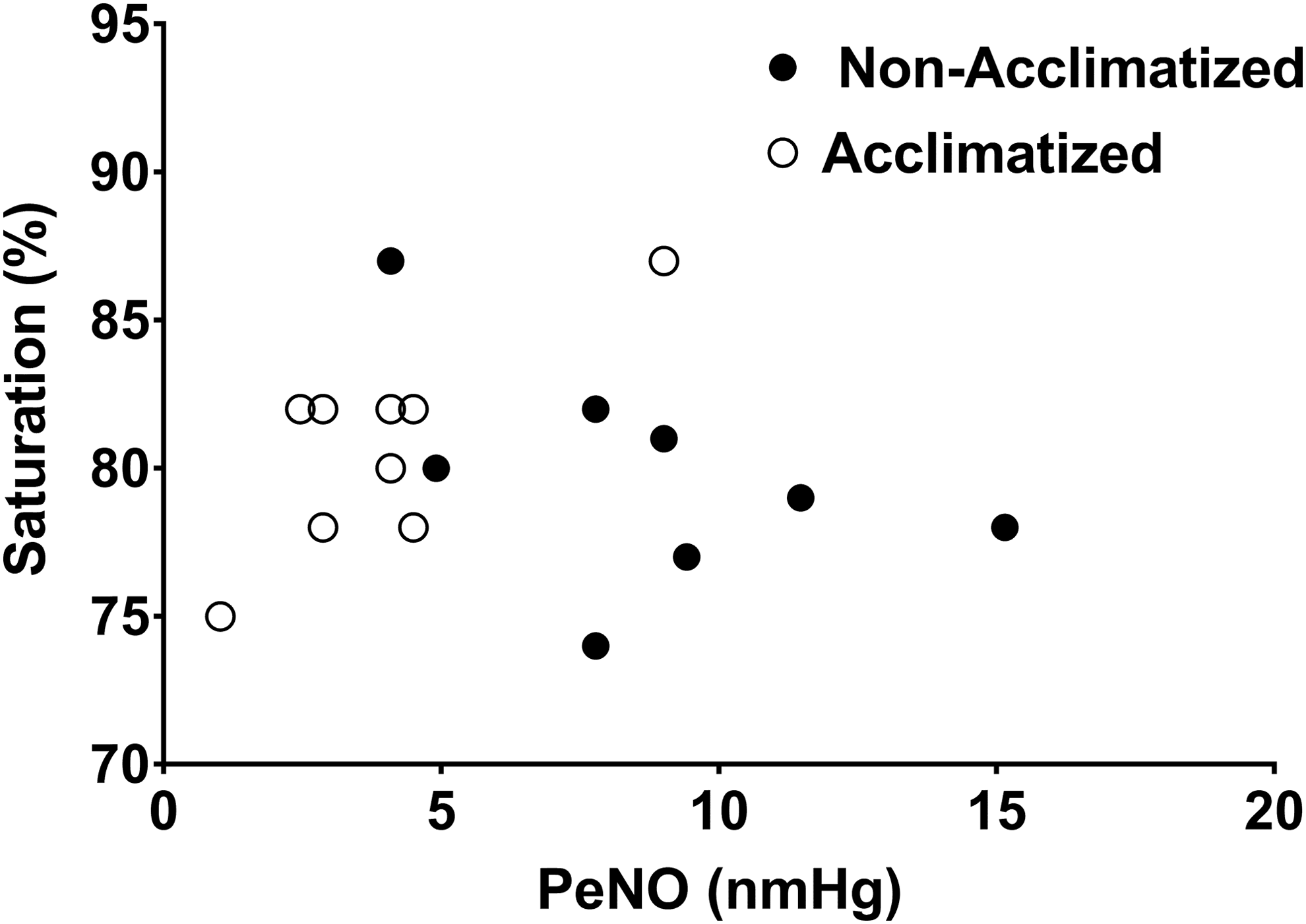
SaO2 levels as a function of PeNO levels in non-ACC and ACC subjects at day 1 of arrival of the non-ACC cohort. There was no correlation between PeNO and SaO2 in either group, or combined. 1 nm Hg = 10−6 mm Hg = 1.333 mbar.
Finally, Hgb levels were measured in all non-ACC subjects and a subset of ACC subjects on day 1 only. Although not significant, there was a trend toward a lower PeNO being associated with a higher Hgb level (Fig. 4; R = −0.56, p = 0.056).
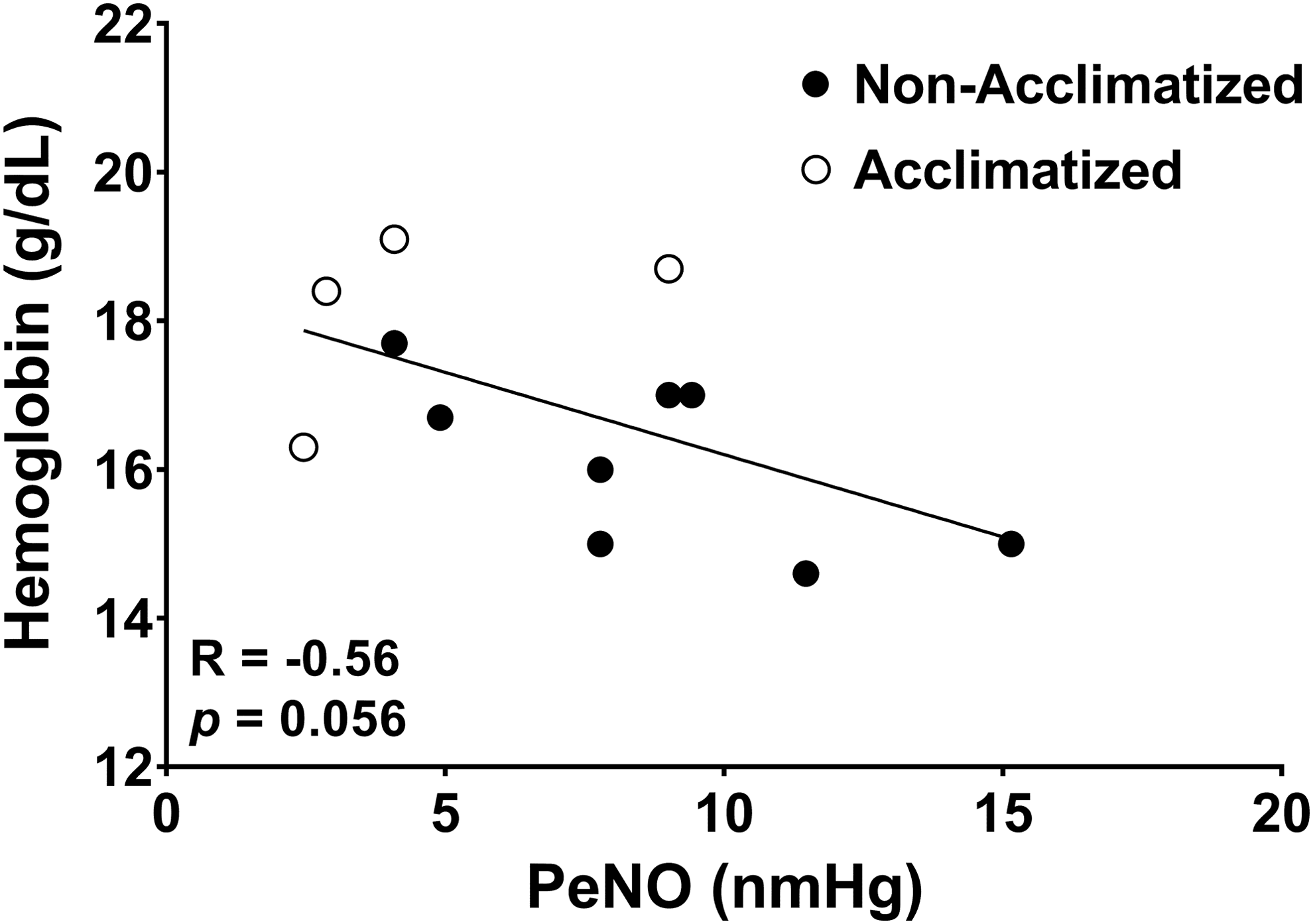
Hgb levels as a function of PeNO levels in non-ACC and ACC subjects at day 1 of arrival of the non-ACC cohort. Hgb levels could only be measured in a subset of the ACC cohort. Although not significant, there was a trend toward a lower PeNO level being associated with a higher Hgb level (R = −0.56, p = 0.056). This may be due to degradation of NO by nitrosylation during binding to hemoglobin. 1 nm Hg = 10−6 mm Hg = 1.333 mbar.
Discussion
Our results show that PeNO levels in subjects who have acclimatized to 5300 m are significantly lower than those who have just arrived to that altitude. In addition, the newly arrived group showed a significant decrease in PeNO levels after 9 days at high altitude, approaching levels seen in the ACC group. Our data are also consistent with prior work done by Duplain et al. that showed an inverse relationship between sPAP and PeNO when subjects are exposed to high altitude (Duplain et al., 2000). Furthermore, there was no correlation between PeNO and daytime oxygen saturations in either group or combined. Overall, these data demonstrate a fall in PeNO levels during the acclimatization process, but would suggest that PeNO is still important for continued regulation of pulmonary vascular tone.
There was also a trend toward a lower PeNO level being associated with a higher Hgb level. This trend could be explained by the fact that NO is rapidly inactivated within the pulmonary vasculature through nitrosylation during binding to Hgb. Thus, increased Hgb may hasten the inactivation of NO.
Previous studies have evaluated the role of pulmonary NO during acclimatization; however, these studies looked at changes across different altitudes as well as different subjects' ethnicity. Wu et al. examined both Tibetan and non-Tibetan infants born at 3658 m and compared them with non-Tibetan infants born at 16 m. They found that infants born at high altitude had increased levels of PeNO during their first week of life when compared with those born near sea level. Genetic differences were detected as well. Non-Tibetan infants born at altitude were more likely to require oxygen supplementation to improve their saturations, suggesting a genetic adaptation in those groups who permanently reside at altitude (Wu et al., 2016). In contrast to Tibetan adaptation, differences in adaptation of Andean adults may not be dependent on NO concentrations, thus suggesting genetic differences in adaptation. This was demonstrated by Schwab et al. Their research, performed in Bolivia, compared PeNO and sPAP of native Bolivians with gender-matched Caucasians exposed to 3600 m. They found no differences between the two groups when PeNO and sPAP were compared (Schwab et al., 2008). Gender differences in eNO levels may also exist, as Li found average fractional eNO (ppb) levels to be higher in male vs. female Tibetans (Li, 2014). In addition, Li also found eNO levels were inversely related to altitude, with higher altitude subjects demonstrating lower eNO levels (Li, 2014).
Other research, including ours, also demonstrated that PeNO levels decrease during exposure to altitude (Brown et al., 2006; Donnelly et al., 2011; Duplain et al., 2000). However, one must be careful in the reporting of eNO levels taken at altitude. In 2009, Hemmingsson et al. argued that altitude studies implementing the use of the NIOX MINO device may have errors and results should be reported as partial pressures rather than the fractional volume (parts per billion and typically termed exhaled or eNO levels) that the device detects. Their reasons for this recommendation are as follows: mass flow decreases with altitude, eNO fractional concentrations increase with decreasing mass flow, reduced ambient pressure leads to a proportionally lower pressure of NO, and finally that the electrochemical detector is more sensitive to NO at altitude. Thus, the displayed values would not reflect the true decrease in eNO at altitude (Hemmingsson et al., 2009).
Importantly, Hemmingsson et al's (2009) article details a conversion that can be used for eNO in reporting partial pressures at altitude. This conversion was applied to our subjects. Of note, the conversion factor depends on the study of a specific NIOX MINO device, and thus it is possible that the conversion factor may be different on the device used presently. This incorporates another limitation in that we were unable to calibrate the NIOX MINO at altitude. Thus, although the values were converted from ppb to nmHg, the values were not able to be verified while at altitude. Importantly, however, the measurements between the two cohorts were taken at the same altitude and at the same time. Thus, the differences seen between the two cohorts are comparable, even if the absolute values are not. All in all, consistency in reporting high-altitude eNO measurements is crucial to the ability to compare across altitudes and studies.
The mechanism for changes in PeNO at altitude and the subsequent development of HAPE in some individuals continue to be investigated. Duplain's work suggested that decreased eNO in HAPE-prone subjects may be due to a defect in pulmonary epithelial NO synthesis, which may lead to increased hypoxic pulmonary vasoconstriction and subsequent pulmonary edema (Duplain et al., 2000). Pulmonary blood flow appears to have an effect on both eNO and plasma concentrations themselves. This was demonstrated by Tworetzky et al. (2000) who measured eNO and plasma NO levels before and after atrial septal defects were repaired. After closure of the defect, both eNO and plasma levels fell within 30 minutes. This occurred without corresponding changes in either average pulmonary or systemic artery pressures (Tworetzky et al., 2000).
During our study, PeNO levels in the ACC group were lower; this may be due, in part, to the length of stay at altitude leading to an increased elimination of NO, which was also proposed by Hemmingsson (2009). It has also been speculated that lower bioavailability of its precursors would also lead to lower eNO levels. This was hypothesized by Schneider et al. (2001). Since NO is produced during the conversion of arginine to
In this unblinded study, physical performance of each subject could also be observed. The most striking observation made was within the ACC group, between the subject with the highest PeNO level and the subject with the lowest. The former also maintained the highest resting oxygen saturation with the latter achieving the lowest resting oxygen saturation. Furthermore, the latter was unable to summit to 8848 m even on supplemental oxygen, whereas the former who maintained a higher PeNO level was able to summit without oxygen. This may be partially explained by work done in 2000 by Tsuchiya et al. They found that exhaled NO concentrations in lung healthy volunteers were positively correlated with PaO2 and negatively correlated with the alveolar–arterial (A-a) oxygen gradient (Tsuchiya et al., 2000). Larger A-a oxygen gradients would be expected to be seen in subjects with underlying diffusion problems.
Previously, MacInnis et al. have shown a correlation between altitude sickness and low baseline FENO levels (MacInnis et al., 2012). However, future research should seek to validate and use PeNO levels as a performance predictor for those traveling to high altitude, either before travel or during the journey itself. Conceivably an individual attempting to operate at high altitude and who might be at risk for performance degradation or the development of HAPE could be identified with falling PeNO levels before they were affected. Mitigation strategies for these individuals, such as the use of supplemental oxygen earlier or removal from the exposure through descent, could also be implemented. In addition, in the future it may be possible to preselect individuals who are well suited for high-altitude exposure. This would benefit those interested in high-altitude experiences in an elective nature such as a sport climber, as well as those required to function at high altitude such as some military personnel operating in these environments.
Footnotes
Acknowledgments
This study was part of a larger Everest Expedition funded by The North Face Company, The National Geographic Society, and Mayo Clinic through a grant from the Leslie and Lou Gonda families. This expedition was the 2012 Legacy Climb led by Conrad Anker to celebrate the 50th anniversary of the 1963 American Mt. Everest Expedition. The authors thank Mr. Andrew Miller, Mr. Alex Kasak, and Mrs. Kathy O'Malley for their help with participant recruitment and data collection.
Author Disclosure Statement
This study was funded by The North Face (VF Corporation), The National Geographic Society, and Mayo Clinic. B.J.T. was supported by AHA grant 12POST12070084.