
Abstract
Abstract
Berger, Marc Moritz, Franziska Macholz, Peter Schmidt, Sebastian Fried, Tabea Perz, Daniel Dankl, Josef Niebauer, Peter Bärtsch, Heimo Mairbäurl, and Mahdi Sareban. Inhaled budesonide does not affect hypoxic pulmonary vasoconstriction at 4559 meters of altitude. High Alt Med Biol 19:52–59, 2018.—Oral intake of the corticosteroid dexamethasone has been shown to lower pulmonary artery pressure (PAP) and to prevent high-altitude pulmonary edema. This study tested whether inhalation of the corticosteroid budesonide attenuates PAP and right ventricular (RV) function after rapid ascent to 4559 m. In this prospective, randomized, double-blind, and placebo-controlled trial, 50 subjects were randomized into three groups to receive budesonide at 200 or 800 μg twice/day (n = 16 and 17, respectively) or placebo (n = 17). Inhalation was started 1 day before ascending from 1130 to 4559 m within 20 hours. Systolic PAP (SPAP) and RV function were assessed by transthoracic echocardiography at low altitude (423 m) and after 7, 20, 32, and 44 hours at 4559 m. Ascent to high altitude increased SPAP about 1.7-fold (p < 0.001), whereas RV function was preserved. There was no difference in SPAP and RV function between groups at low and high altitude (all p values >0.10). Capillary partial pressure of oxygen (PO2) and carbon dioxide as well as the alveolar to arterial PO2 difference were decreased at high altitude but not affected by budesonide. Prophylactic inhalation of budesonide does not attenuate high-altitude-induced pulmonary vasoconstriction and RV function after rapid ascent to 4559 m.
Introduction
P
A recent randomized, placebo-controlled trial showed that oral intake of the corticosteroid dexamethasone (8 mg twice per day) lowered systolic PAP (SPAP) and prevented HAPE in a susceptible population after rapid ascent to 4559 m (Maggiorini et al., 2006). In that study, the vasodilatory effect of dexamethasone was comparable to that of the selective pulmonary vasodilator tadalafil (a phosphodiesterase-5 inhibitor). The mechanisms underlying this favorable effect of dexamethasone remain unclear but may be related to an improvement in endothelial function, increased production of cyclic guanosine monophosphate, and increased nitric oxide synthase activity (Asoh et al., 2000; Murata et al., 2004). In addition, dexamethasone may decrease sympathetic activity (Scherrer et al., 1993) and decrease pulmonary vascular permeability, possibly by preventing an inflammatory response to hypoxia (Stenmark et al., 2005) as indicated by the lack of increase in C-reactive protein and interleukin-6 in HAPE-susceptibles receiving dexamethasone (Maggiorini et al., 2006).
The present placebo-controlled, randomized, and double-blind study investigated whether inhalation of the corticosteroid budesonide at two different doses (200 and 800 μg twice/day) during active, rapid ascent (<20 hours) from 1130 to 4559 m lowers SPAP and might have the potential to prevent HAPE. If effective, budesonide inhalation may serve as a new and safer pharmacological agent for prophylaxis against HAPE, because it avoids the potentially serious side effects associated with systemically applied corticosteroids. In addition, we performed serial echocardiographic examinations by using recent Doppler imaging techniques to investigate whether the altitude-induced increase in SPAP with and without inhalation of budesonide affects RV function. These data were obtained in a study (Berger et al., 2017) that did not confirm a protective effect of inhaled budesonide against acute mountain sickness (AMS) that has been previously reported (Zheng et al., 2014; Chen et al., 2015).
Materials and Methods
Study approvals and registration
The study was performed in accordance with the Declaration of Helsinki and its current amendments, and it was approved by the Ethical Committee Salzburg, Austria, by the Ethical Committee of the University of Torino, Italy, and by the Competent Authority (BASG), Vienna, Austria. The study was registered at ClinicalTrials.gov. (NCT02811016), and it was conducted as a prospective, randomized, double-blind, and placebo-controlled trial, with group stratification according to gender, age, and physical fitness. The study was part of a trial investigating the effect of inhaled budesonide on AMS (Berger et al., 2017).
Subjects and group assignment
Fifty-one healthy, non-smoking, and non-acclimatized native lowlanders provided written informed consent and were included in the study. None of these subjects spent time at altitudes >2000 m within the past 4 weeks before the study, and none took any regular medication. Because one participant withdrew after baseline measurements, the analysis is based on data sets of 50 subjects.
Subjects were randomized to receiving 200 μg budesonide twice/day (group B200, n = 16), 800 μg budesonide twice/day (group B800, n = 17), or lactose-monohydrate (placebo group, n = 17). The capsules of all study groups looked identical. During the low-altitude tests, subjects were instructed on the correct use of the single-dosed capsules in the inhaler (Cyclohaler®; PB Pharma, Meerbusch, Germany). Inhalations were performed at 7 a.m. and 7 p.m. starting 1 day before ascent and continued until the end of the study. Complete emptying of the capsules was visually verified, and at high altitude all inhalations were performed under supervision to ensure correct inhalation technique. Both the participants and the investigators were blinded with respect to the study drug. Other personal medication was not allowed.
Study protocol
Baseline measurements were performed at an altitude of 423 m (Salzburg, Austria). They consisted of a physical examination, an echocardiographic assessment of SPAP and RV function, and lung function testing.
Between 2 and 4 weeks later, subjects traveled to Alagna (1130 m), Valsesia, Italy, and ascended in groups of 10 accompanied by licensed mountain guides to 4559 m within 20 hours. The ascent consisted of transportation by cable car to 3275 m, and a 90-minute climb to 3611 m (Capanna Giovanni Gnifetti), where subjects spent the night. On the next morning, they climbed to 4559 m (Capanna Regina Margherita, Monte Rosa) in about 4 hours. All examinations were performed 7, 20, 32, and 44 hours after arrival at 4559 m. However, due to logistic reasons, RV function could not be assessed after 32 hours.
Diagnostic criteria for and treatment of subjects with AMS are detailed elsewhere (Berger et al., 2017).
Echocardiography
After participants had rested for 5 minutes in supine position, transthoracic echocardiography was performed by using a commercially available ultrasound system (Philips CX50; Phillips Medical Systems, Andover, MA) with a 1.0–5.0 MHz sector array transducer (Philips S5-1; Phillips Medical Systems). All measurements were made by the same experienced echocardiographer with the subject lying in the left lateral decubitus position. All images were recorded in a raw digital imaging and communications in medicine format on a mass storage device and analyzed offline.
Assessment of SPAP
As previously shown, Doppler echocardiography represents an accurate and reproducible method for estimating SPAP at high altitude and correlates well with invasive measurements (Allemann et al., 2000). For the determination of SPAP, peak-flow velocities of tricuspid valve regurgitation jets using continuous-wave Doppler were measured in the RV inflow projection of the parasternal long-axis view, the parasternal short-axis view, or the apical four-chamber view. The highest coherent boundary of the spectral wave was used to calculate the right atrial to RV pressure gradient by using the modified Bernoulli equation (Rudski et al., 2010). For calculation of SPAP, 5 mmHg was added as an estimate for right atrial pressure (Yock and Popp, 1984). All measurements were evaluated offline by two independent echocardiographers blinded to clinical and experimental data.
Assessment of functional RV parameters
Considering the complex structure, asymmetrical shape, and contraction pattern of the RV, multiple parameters of RV function were assessed as recommended (D'Alto et al., 2015) and obtained according to recent international guidelines (Rudski et al., 2010).
Tricuspid annular plane systolic excursion (TAPSE), a measure of longitudinal RV systolic function, was assessed by placing an M-mode beam through the lateral tricuspid annulus and the highest amount of RV longitudinal motion of the annulus at peak systole was obtained from a standard apical four-chamber window (Rudski et al., 2010).
Peak tricuspid lateral annular systolic velocity (S′), a measure of global RV systolic function, was assessed by placing the pulsed-wave Tissue-Doppler sample volume in the lateral tricuspid annulus of the RV free wall by using a standard apical four-chamber window. Special attention was paid to proper alignment of Doppler beam with RV free wall longitudinal excursion. The velocity S′ was read as the highest systolic velocity without over-gaining the Doppler envelope (Rudski et al., 2010).
The RV myocardial performance index (MPI), a global estimate of both systolic and diastolic RV function and also known as Tei index, was assessed by using the same pulsed-wave Tissue-Doppler image as S′ and calculated as the sum of RV isovolumic contraction and relaxation times divided by ejection time (Rudski et al., 2010).
The RV fractional area change (FAC), a global estimate of systolic RV function, was assessed by tracing the endocardial RV border in an RV-focused apical four-chamber view at end-diastole and end-systole. Trabeculation, tricuspid leaflets, and chords were included in the chamber and FAC was calculated by using the formula: (end-diastolic area − end-systolic area)/end-diastolic area × 100 (Rudski et al., 2010).
Further measurements
After 5 minutes of rest in supine position, heart rate and peripheral oxygen saturation (SpO2) were measured by pulse oximetry (Covidien Nellcor, Mansfield), and blood pressure was measured non-invasively by analyzing brachial artery waveforms (Pulsecor®, Auckland, New Zealand).
Because budesonide inhalation might affect lung function, oxygenation, and, consequently, SPAP and RV afterload, spirometry (EasyOne Spirometer, ndd Medizintechnik, Zürich, Switzerland) and capillary blood gas analysis (Siemens, RapidPoint 500, Germany) were performed to assess these potential confounders. Forced expiratory volume in one second (FEV1) and the forced vital capacity (FVC) were expressed as percent of the predicted value according to the global lung function 2012 equations (Quanjer et al., 2012). Subjects were familiarized with the breathing maneuvers before baseline measurements.
Blood gas analysis was performed in samples collected from the hyperemic ear lobe and immediately analyzed for partial pressures of oxygen (PO2) and partial pressure of carbon dioxide (PCO2). The alveolar to arterial PO2 difference (AaDO2) was calculated from the alveolar gas equation (Fenn et al., 1946) assuming a respiratory exchange ratio of 0.85 (West et al., 1983) and that alveolar PCO2 was equal to capillary PCO2.
Statistical analyses
Normal distribution of the data was tested by using the Kolmogorov–Smirnov test. Effects of altitude and treatments were analyzed by two-way repeated-measures analysis of variance. Pairwise multiple-comparison procedures were made by using the Student–Newman–Keuls test. The relationship between pairs of variables was expressed with the Pearson Correlation Coefficient (R). Data are expressed as mean values ± standard deviation. A p value of ≤0.05 (two-sided) was considered significant. Statistics were performed by using the SigmaStat® software package (SPSS, Inc., Chicago, IL).
Results
Baseline characteristics and drug intake at high altitude
The baseline characteristics did not show statistically significant differences between the three study groups (Table 1).
There were no significant differences between the study groups. B200 and B800 indicate budesonide inhalation at 200 and 800 μg twice/day.
As detailed elsewhere (Berger et al., 2017), there were no differences between the study groups regarding the incidence and severity of AMS. Due to very severe AMS, one subject of the B800 and three subjects in the placebo group were treated with oxygen, acetazolamide (250 mg), and oral dexamethasone (4 mg) after 9, 10, 21, and 35 hours at high altitude. In these four subjects, final measurements were performed before treatment was initiated and data collection was terminated thereafter.
Systolic PAP
Ascent to high altitude increased SPAP in all three study groups by about 1.7-fold (p < 0.001 vs. low altitude, Fig. 1). SPAP remained unchanged throughout the 48 hours at high altitude. Neither at low altitude nor at any time point at high altitude was there a significant difference in SPAP between groups (p = 0.419; Fig. 1).
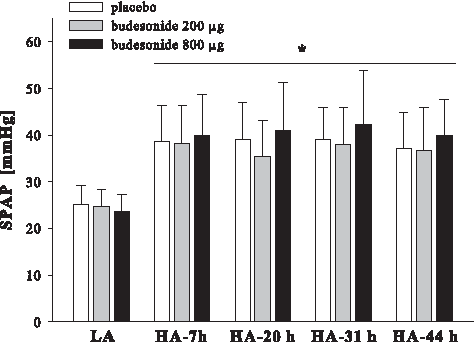
SPAP. LA, low altitude (423 m, Salzburg, Austria). HA, high altitude (4559 m). Data are displayed as mean ± SD; *p < 0.001 versus low altitude. Ptime = 0.288; Pgroup = 0.419; Ptime × group = 0.360. SD, standard deviation; SPAP, systolic pulmonary artery pressure.
RV function measurements
TAPSE (Fig. 2A) and S′ (Fig. 2B) were increased at high altitude (p = 0.005 and p < 0.001, respectively), whereas the global RV parameters MPI (Fig. 3A) and FAC (Fig. 3B) did not change at high altitude. None of the parameters was affected by budesonide inhalation. The increase in SPAP from baseline to the first examination at high altitude did not significantly correlate with the change in functional RV parameters: TAPSE (R = 0.10, p = 0.51), S′ (R = 0.03, p = 0.86), MPI (R = −0.07, p = 0.65), and FAC (R = 0.21, p = 0.19).


Lung function and hemodynamic measurements
Table 2 shows that FVC and FEV1 decreased slightly (p < 0.001) at high altitude but remained within normal limits. The ratio between FEV1 and FVC remained unchanged. There were no differences among groups at any time point. Heart rate and diastolic blood pressure increased at high altitude, whereas systolic blood pressure remained unchanged. None of these parameters was affected by inhalation of budesonide (Table 2).
Statistics: two-way repeated-measures ANOVA.
LA, low altitude (423 m, Salzburg, Austria); HA, high altitude (4559 m); B200 and B800 indicate budesonide inhalation at 200 and 800 μg twice/day; Pt = difference over time, Pgroup = difference between groups (B200, B800, placebo) and Pt × group = degree of interaction between factor A (time) and B (group).
ANOVA, analysis of variance; BP, blood pressure; diast, diastolic; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; pred, predicted; syst, systolic.
Blood gases
Capillary PO2 and PCO2 as well as SpO2 and AaDO2 were decreased at high altitude (p < 0.001), without a significant difference between study groups (Table 3). SPAP correlated inversely with capillary PO2 (R = −0.58, p < 0.001).
Statistics: two-way repeated-measures ANOVA.
AaDO2, alveolar to arterial PO2 difference; cap, capillary; PCO2, pressure of carbon dioxide; PO2, pressure of oxygen; SpO2, peripheral oxygen saturation.
Discussion
This prospective, randomized, double-blind, and placebo-controlled study on healthy, non-acclimatized lowlanders demonstrates that prophylactic inhalation of budesonide at 200 and 800 μg twice/day did not reduce the increase in SPAP after rapid ascent to 4559 m when compared with placebo. The results further show that the altitude-induced increase in SPAP did not attenuate RV function.
Effect of inhaled budesonide on high-altitude pulmonary hypertension
The ascent to high altitude increased SPAP to about 40 mmHg, which is in line with previous studies (Allemann et al., 2000; Berger et al., 2009; Bailey et al., 2010). The lack of an SPAP-lowering effect of budesonide cannot be attributed to the dosing, since typical doses used in the clinical setting range from 100 to 800 μg twice/day (Clearie et al., 2011). Even the high budesonide dose of 800 μg twice/day had no effect on the extent of high-altitude-induced pulmonary vasoconstriction, indicating that the concentration of inhaled budesonide reaching the vasculature, that is, vascular endothelial and smooth muscle cells, was not high enough to induce vasodilation. It cannot be excluded that the particle size of about 4 μm delivered by the Cyclohaler (Sebti and Amighi, 2006) was too big to allow budesonide molecules to reach small resistance vessels located around the alveoli. However, since we cannot exclude that budenoside particles did reach their target, it remains unclear as to whether the action of glucocorticoids on the pulmonary vasculature is related to a local enhancement of nitric oxide synthase activity or its systemic effects on neurohumoral activity and inflammation. Indeed, in the present setting, no suppression of plasma adrenocorticotropic hormone—reflecting hypothalamic-pituitary-adrenal axis suppression—was observed (Berger et al., 2017). Therefore, and in contrast to oral dexamethasone, inhaled budesonide is also unlikely to attenuate the exaggerated increase in SPAP of HAPE-susceptibles and, thus, to prevent HAPE. Together with the lack of effect of inhaled budesonide on AMS (Berger et al., 2017), our results indicate that inhaled budesonide cannot be recommended for the prevention of acute high-altitude illness.
RV function and effect of inhaled budesonide
The RV is challenged at high altitude due to the increased afterload resulting from hypoxic pulmonary vasoconstriction (Naeije and Dedobbeleer, 2013). The few studies that have assessed changes in RV function at high altitude have considerable differences between the echocardiographic variables, leading to conflicting results (Huez et al., 2005; Reichenberger et al., 2007; Hanaoka et al., 2011). Some variables such as the TAPSE explore systolic function only, whereas variables such as the MPI and FAC are affected by both systolic and diastolic function. To characterize possible changes, we obtained multiple echocardiographic variables of RV function and further investigated whether these are affected by prophylactic budesonide inhalation.
Variables of global RV function, that is, MPI and FAC, did not change at high altitude, indicating that global RV function was preserved and not attenuated by the increase in SPAP. In addition, the longitudinal parameters of RV systole, that is, TAPSE and S′, were slightly elevated at 4559 m, which can be interpreted as systolic adaptation of the RV to the increased afterload (Naeije and Dedobbeleer, 2013) and/or to the positive inotropic effect of hypoxia-induced sympathetic nervous system activation (Duplain et al., 1999). However, the changes in RV parameters did not correlate with the changes in SPAP, indicating that the pattern of adaption was not directly related to the degree of pulmonary vasoconstriction.
Our findings are in line with a previous study in normobaric hypoxia that also showed no alteration of global RV performance (MPI) in HAPE-resistant subjects with an SpO2 of 75%–80% (Hanaoka et al., 2011). Also, Huez et al. (2005) found that parameters of systolic RV function (FAC, TAPSE, S′) were not affected by 90 minutes of hypoxic breathing corresponding to an altitude of 4500 m. In contrast, Reichenberger et al. (2007) observed an increase in RV-MPI, indicating impaired RV contractility in healthy volunteers at 3440 and 5245 m, respectively, that was partially reversed by administration of the pulmonary vasodilator sildenafil. However, as in our study, TAPSE was not reduced. Considering that hypoxia has been shown to slow myocardial relaxation in animal studies (Silverman et al., 1997) and that echocardiographic-derived data have indicated that functional changes induced by hypoxia predominate in the RV during diastole (Huez et al., 2005), our results suggest that global RV function is preserved in hypoxic conditions due to positive inotropic effects that counterbalance negative lusitropic (i.e., diastolic) effects.
Before the study, it appeared possible that budesonide attenuates RV function by lowering SPAP and RV afterload. However, budesonide had no effect on any of the measured RV parameters. This finding is in line with the lack of effect of budesonide on SPAP and RV afterload and further indicates that inhalation of corticosteroids does not directly improve myocardial performance under hypoxic conditions.
Effect of inhaled budesonide on lung function and gas exchange
Budesonide is one of the most frequently prescribed inhaled corticosteroids worldwide that has been used in the long-term management of chronic obstructive pulmonary disease and asthma for many years (Melani, 2012). To assess possible effects of budesonide on lung function, FVC and FEV1 were measured. In this study, ascent to high altitude decreased FVC and FEV1. These findings are in line with previous studies reporting a reduction in the predicted (Basu et al., 1996; Senn et al., 2006) and absolute (Pollard et al., 1996; Hashimoto et al., 1997; Mason et al., 2003) values of FVC and FEV1 at altitudes up to 5300 m. In our study, budesonide inhalation was started 48 hours before arrival at 4559 m to ensure a long enough intake for improving lung function (Edmonds et al., 2012; Mendes et al., 2014). However, even the highest dose of budesonide did not improve pulmonary function tests. A possible explanation for this finding is that the observed decrease in FVC and FEV1 was caused by a reduced effort due to fatigue or symptoms of AMS that may impair the maximum effort that is critical to adequate pulmonary function testing and/or by increased lung water content (Cremona et al., 2002; Senn et al., 2006; Dehnert et al., 2010; Clarenbach et al., 2012). Whether budesonide inhalation might exert beneficial effects in patients with pre-existing pulmonary disease traveling to high altitude remains unknown.
In line with the lack of effect on lung function and SPAP, budesonide inhalation had no effect on oxygenation and ventilation, that is, on the altitude-induced decrease in SpO2, capillary PO2, and PCO2. It is well established that AaDO2 decreases as the PO2 falls and that an impairment of pulmonary diffusion increases AaDO2 (Wagner et al., 1987; Grocott et al., 2009). On the other hand, a decreased AaDO2 indicates improved pulmonary diffusion. In this study, AaDO2 decreased at high altitude without being different between the three study groups. This finding indicates that inhaled budesonide had no effect on interstitial and alveolar water content, ventilation-perfusion ratio, shunting, or a hypoxia-mediated change in lymphatic drainage, all of which might affect pulmonary diffusion capacity (Petersson and Glenny, 2014; Wagner, 2015) and, consecutively, oxygenation and SPAP. However, we cannot exclude that the lack of effect was caused by the size of the inhaled budesonide particles, which may have impeded that budesonide reached the alveolar epithelial cells.
Limitations
We used a respiratory exchange ratio of 0.85 for the calculation of AaDO2 (West et al., 1983) and assumed that end-tidal CO2 equals capillary PCO2. For accurate measurements of AaDO2, the direct measurement of end-tidal CO2 and of the respiratory exchange ratio would be required. Unfortunately, measurements of ventilation and respiratory gases were not possible in this study. Although a difference between absolute and calculated values of the AaDO2 has been reported (Bartsch et al., 2002), changes at altitude appear small, and our basic conclusion of a lack of effect of budesonide on alveolar O2 diffusion should not be affected.
We did not investigate HAPE-susceptible individuals who are known to have an exaggerated increase in SPAP at high altitude that is probably caused by a reduction in endothelial nitric oxide synthase activity (Busch et al., 2001; Berger et al., 2005). Since the action of dexamethasone may rely on increasing nitric oxide availability, it is possible that under these circumstances it has no effect on pulmonary vascular tone. Thus, to characterize differences between oral dexamethasone and inhaled budesonide with respect to their effect on SPAP, HAPE-susceptible individuals should be studied.
We did not apply the comet-tail technique of chest ultrasonography that has been described for the diagnosis and monitoring of HAPE (Fagenholz et al., 2007). This approach may have helped to detect extravascular lung water and interstitial pulmonary edema (Jambrik et al., 2004). However, the lack of differences in oxygenation parameters indicates that no significant differences in extravascular fluid content existed between the study groups.
Conclusion
This study shows that inhaled budesonide did not reduce the degree of high-altitude-induced pulmonary vasoconstriction after active and rapid ascent to 4559 m. Moreover, the results show that the altitude-induced increase in RV afterload did not attenuate RV function.
Footnotes
Acknowledgments
The authors are grateful to all the mountaineers who took part in the study, and the mountain guides from the Scuola di Alpinismo Corpo Guide Alagna Valsesia for their excellent, trustful work. They also thank the hut keepers, the RifugiMonterosa, and the Sezione Varallo of the Club Alpino Italiano for providing an excellent accommodation and research facility at the Capanna Regina Margherita. They thank Simone Wurm (Department of Anesthesiology, Perioperative and General Critical Care Medicine, Salzburg General Hospital, Paracelsus Medical University, Austria), as well as Sonja Engelhardt and Christiane Herth (Department of Internal Medicine VII, Division of Sports Medicine, University Hospital Heidelberg, Germany) for excellent technical assistance.
Author Disclosure Statement
No competing financial interests exist.