
Abstract
Abstract
Gorjanc, Jurij, Shawnda A. Morrison, Rok Blagus, and Igor B. Mekjavic. Cold susceptibility of digit stumps resulting from amputation after freezing cold injury in elite alpinists. High Alt Med Biol. 19:185–192, 2018.
Aim:
The aim of the study was to assess whether previous freezing cold injury in fingers and/or toes might predispose alpinists to greater risk of further freezing cold injury, primarily due to a greater vasoconstrictor response to cold, resulting in a lower perfusion, reflected in lower skin temperature.
Methods:
Ten elite alpinists (N = 10; 8 male and 2 female) with amputations after freezing cold injury participated in a cold-water (8°C) immersion stress test of the hands and feet. Digit skin temperatures of amputated digits, their noninjured counterparts, noninjured digits of the affected side and noninjured digits of the corresponding side were measured. The skin temperatures were compared during three consecutive phases of the cold stress test: prewarming, cold water immersion, and passive heating.
Results:
Amputated toes cooled much faster compared to their uninjured counterparts (n = 26, p < 0.001), and attained lower skin temperatures during the cold exposure test (n = 26, p < 0.001). Higher cooling rate was observed in all the toes on the injured limb compared with the toes on the uninjured limb (n = 40, p < 0.001). In contrast to the toes, the fingers on the injured limb after freezing cold injury were warmer during cooling phase compared to uninjured fingers (n = 15, p < 0.001).
Conclusions:
The lower digit temperatures observed in affected toe stumps during the cold stress test compared to the nonamputated toes may indicate a heightened risk of future freezing cold injury with subsequent cold exposures, as a consequence of less perfusion, reflected in the lower skin temperature. This relationship was not confirmed in the fingers.
Introduction
Cold-induced vasodilatation
O
Risk for frostbite
The incidence of frostbite in cold regions is estimated very differently: between 18.1% (Mäkinen et al., 2009; McIntosh et al., 2012) and 56% in arctic regions (Hassi and Mäkinen, 2000; Némethy et al., 2015) and as high as 37% in alpinists (Harirchi et al., 2005). The great variability of incidence depends mainly on external factors (weather worsening), but could also be attributed to individual variability in susceptibility for frostbite (Daanen and van der Struijs, 2005). Frostbite as a clinical diagnosis is pathophysiologically regarded as a combination of freezing- and nonfreezing cold injury (Golant et al., 2008; Heil et al., 2016) (Fig. 1).
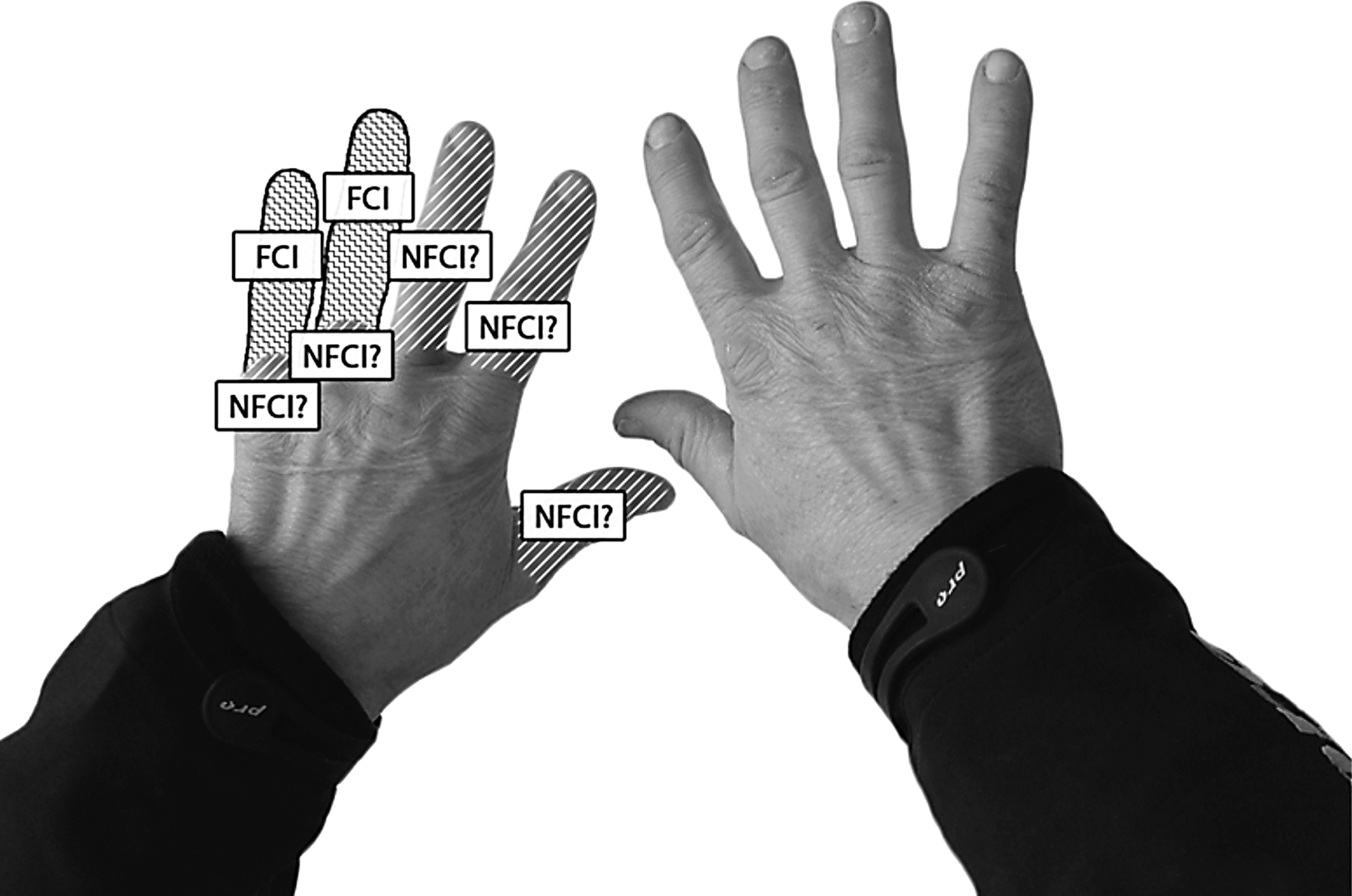
The hands of an alpinist who suffered frostbite of the fourth and fifth left fingers during a storm at an altitude 7600 m during his first attempt at skiing from the summit of Mt. Everest, in 1996. He later accomplished this feat, and he was the first to complete a ski descent of Mt. Everest from the summit to base camp in 2000. This latter attempt did not cause any additional frostbite. The photo and overlaying schematic demonstrates how cold injury may be manifest in the digits of this alpinist. FCI of the left hand required amputations. It is likely that the salvaged tissue of the left hand suffered NFCI. FCI, freezing cold injury; NFCI, nonfreezing cold injury.
Continued mountaineering among alpinists who have suffered freezing cold injury depends on the magnitude of the area affected and especially the degree of amputation that was required (Hassi and Mäkinen, 2000; Gorjanc et al., 2012; Morrison et al., 2015).
It is unclear to what extent freezing cold injury occurs due to the environmental conditions per se (i.e., subzero temperatures, hypoxia, etc.) and to what extent individual factors contribute to it, such as a subject's predisposition to cold susceptibility (Yoshimura and Iida, 1952; Daanen and van der Struijs, 2005), and/or previous cold injury (Morrison et al., 2014). Indeed, tissue that has been frequently exposed to subzero temperatures and/or those that may induce nonfreezing cold injury may be susceptible to further cold injuries (Ingram and Raymond, 2013). Some individuals report diminished sensitivity, or even pain, in digits that have suffered cold injury, but this does not necessarily imply greater susceptibility of these tissues to further cold injury (Ervasti et al., 2000; Ruijs et al., 2009, 2011). In contrast, individuals who are frequently exposed to local cold can have improved tissue perfusion, suggesting a degree of cold adaptation (LeBlanc et al., 1960; Nelms and Soper, 1962; Brändström et al., 2008). This evidence, however, is not unequivocal (Reynolds et al., 2007; Cheung and Daanen, 2012).
Accordingly, we tested the hypothesis that the remaining stumps of previously freezing cold-injured digits have impaired thermal responses to a cold stress test and, as a consequence, possibly reflect a greater predisposition to cold injury during subsequent cold exposures in this population.
Methods
Participants
Tests were performed at the Olympic Sport Centre Planica (Rateče, Slovenia). Active Slovene alpinists, who suffered freezing cold injury with digit amputation, were invited to participate in the study.
A total of 10 alpinists (8 male and 2 female) gave their informed consent to participate in the study. Their mean ± SD age was 44 ± 9.7 years, and body mass 77.7 ± 9.1 kg. Each had suffered severe freezing cold injury that required digit amputation, such that in total, the group had 32 amputated digits (6 amputated fingers and 26 amputated toes). Alpinists were free from any known cardiovascular, respiratory, or metabolic disease. They were all nonsmokers, and not on any medication. They were requested not to exercise or consume caffeinated and/or alcoholic drinks 24 h before the test. The nature of their freezing cold injuries is summarized in Table 1.
LH, left hand; RH, right hand; LF, left foot; RF, right foot; ⇩, partial length amputation; ⇳, full length amputation; F, finger; T, toe; 1–5, numbers of affected digits; FCI, freezing cold injury.
Experimental design
Digit skin temperature was measured on the dorsal surface of each nail bed using T-type thermocouples. The data were recorded and stored using an Almemo model 5990–2 data acquisition system (Ahlborn, Holzkirchen, Germany) at one-minute intervals throughout the cold water immersion protocol. Digit temperature was measured proximal to the injury site in the case of amputations (INJ), and an additional thermocouple was placed on the corresponding location of the uninjured digit (CORR) of the contralateral side. Additional thermocouples were attached to the nail beds of the noninjured digits of the injured limb (noninjured same side [NISS]) and to the corresponding tips of the contralateral limb (noninjured corresponding site [NICO]) (Fig. 2). The thermocouples were attached to the skin using a thin, breathable adhesive tape (Tegaderm™, 3M™; 3M Healthcare, St. Paul, MN). Once the subjects were instrumented, and completed a 5-min baseline measurement, they placed the test limb (either hand or foot) in a thin, plastic bag to avoid getting the skin wet during the water immersion using methods described elsewhere (Daanen and van der Struijs, 2005; Cheung and Mekjavic, 2007). The alpinists' hand or foot was then immersed in a circulated water bath, first for 5 min at 35°C to normalize digit temperature (prewarming), and then for 30 min in a cold water bath at 8°C (cold water immersion) (Mekjavic et al., 2013). Digit skin temperatures were also recorded for 10 min postimmersion to determine rates of recovery from the cold stress test (passive heating). In the case of injured limbs, both the injured and noninjured hand and/or foot were tested in random sequence.

Placement sites for the thermocouples on the hands of a representative subject. Drawing of thermocouple locations on injured digits and their noninjured counterparts. INJ, injured digit; CORR, corresponding noninjured digit on contralateral side; NISS, noninjured digit on the same side as the injured digit; NICO, noninjured digit on the corresponding noninjured side.
The study protocol was approved by the National Committee for Medical Ethics at the Ministry of Health of the Republic of Slovenia (approval Nr. 22p/04/10).
Statistical analyses
When analyzing digit temperature, the measurement site (INJ, CORR, NISS, and NICO), phase of the experiment (prewarming, cold water immersion, and passive heating), and their two-way interaction were used as covariates in the linear mixed effects model, where subjects were included as a random effect (random intercept) to account for the within-subject correlation of the repeated measures. Contrast analysis was performed to explore the predetermined effects. These included the comparison of CORR versus INJ, NISS versus NICO, and the mean of INJ and NISS versus the mean of CORR and NICO at different phases, and for the change in mean skin temperature between recovery and cold phases and between cold and prewarm phases. To adjust for the multiple testing problem, simultaneous tests for general linear hypotheses were performed (Hothorn et al., 2008), and 95% confidence intervals are reported for the estimated effect sizes. Separate analyses were performed for fingers and toes. When analyzing the wave probability a similar analysis was performed, using a random effects logistic regression model and considering only the cold phase.
A p-value of less than 0.05 was considered as significant. All analyses were conducted with R language for statistical computing (version year 2014).
Results
In contrast to finger temperatures, more significant differences were observed in mean toe temperatures between digit stumps (INJ) and the corresponding location (CORR) (Tables 2 and 3).
Bold represents statistical significance (p < 0.05).
CORR, corresponding location of the uninjured digit; NISS, noninjured same side; NICO, noninjured corresponding site.
Bold represents statistical significance (p < 0.05).
Prewarming phase
The injured toes had a 0.9°C higher skin temperature than the corresponding sites on the uninjured digits during immersion in 35°C water in the prewarm phase (n = 26, p = 0.009). Skin temperature of the toes on the same side as the amputated toes (but not amputated, NISS) were 1.5°C warmer than the corresponding sites on the digits of the contralateral side to the injury (n = 14, p < 0.001).
Cold water immersion phase
During the cold stress test, average injured toe temperature was significantly colder by ∼1.5°C than the corresponding noninjured digits on the contralateral side, representing an average decrease of ∼13% (n = 26, p < 0.001). Also, injured toes cooled much faster compared to their noninjured counterparts (n = 26, p < 0.001); the same tendency of faster cooling was observed in all the toes on the injured limb compared with the toes on the uninjured limb (n = 40, p < 0.001). In contrast, the fingers of the injured limb (INJ+NISS) were significantly warmer than the fingers on contralateral side (CORR+NICO) (n = 15, p < 0.001).
Passive heating phase
There were no statistically significant differences in mean finger or toe recovery temperatures between the injured and corresponding digits. The injured toes rewarmed faster than the corresponding noninjured toes (n = 26, p = 0.015). In the rewarming phase, fingers on the noninjured side (CORR+NICO) rewarmed significantly faster than the stumps and fingers on the injured hand (n = 15, p = 0.003) (Fig. 3).

Digit skin temperature responses (mean values of all fingers/toes for every minute) during the three phases of the cold stress protocol; NISS, noninjured digits on the affected side; NICO, noninjured digits on the corresponding (noninjured) side; all mean temperature values were averaged of several digits: for hands (nINJ or CORR = 6, nNISS or NICO = 9); for feet (nINJ or CORR = 26, nNISS or NICO = 14); n = number of digits.
Number of CIVD waves
The number of CIVD waves in injured toes was not significantly different from the average number of CIVD waves in the alpinists' corresponding toes (1.5 vs. 1.07; p = 0.33). The low number of CIVD waves in toes in the NISS group vs. NICO group (0.38 vs. 1.23; p = 0.01) did not result in a significantly different average temperature (Tmean) of these toes during the cold water immersion phase, suggesting that this magnitude of difference in number of CIVD waves, although significant, is not physiologically relevant (Table 4). There was no statistically significant difference in the number of CIVD waves between both groups of immersed fingers.
n, number of fingers or toes; nCIVD, number of CIVD waves in digits; nwaves/toe or finger, number of CIVD waves/digit; *indicates a significant difference between the pooled digits (p < 0.05). CIVD, cold-induced vasodilatation.
Discussion
The principal finding of this study is that during the cold water immersion phase of the cold stress test, the injured toes were colder by ∼1.5°C than the corresponding noninjured toes on the contralateral side, and also that these injured toes were able to rewarm more quickly than the noninjured toes. Injured toes were also warmer during prewarming phase. The cooling rate of all the toes of the injured (INJ+NISS) side was significantly greater than that of the corresponding noninjured (CORR+NICO) toes.
Thermal responses observed in the toes
Although freezing and nonfreezing cold injury are not categorized as pain syndromes, [known clinically as complex regional pain syndrome (CRPS)], the vasomotor responses described in the CRPS syndrome have similar characteristics to those observed in the injured digits, in this study. Using a water perfused suit to initiate cooling and warming of the body of individuals suffering CRPS, Wasner et al. (2001) reported that in CRPS-impaired limbs, skin temperature is colder during cooling and warmer during controlled warming compared with the contralateral healthy counterpart, due to higher and lower sympathetic drives, respectively. We observed these same characteristic thermal responses in the amputated toes of the alpinists, but without pain symptoms. The toe skin temperature changes in our study indicate a reduction in perfusion of the digits during the cold water immersion phase, and a greater increase in perfusion of injured digits compared to healthy counterparts during the prewarming phase.
According to Wasner et al. (2001), previous nerve injury can be considered a cause for such impaired thermoregulatory patterns. According to them, injured limbs (or digits) may cool faster during higher sympathetic activity (cold phase or cold weather) and rewarm faster under warm conditions that is, lower sympathetic activity. As the principal mechanism of freezing cold injury is freezing of tissue and vascular injury during the cold exposure (similar to the cold phase in the cold stress test), we may conclude that the responses observed during the cold phase have greater clinical importance than those in the rewarming (or recovery) phases (Gorjanc, 2006; Golant et al., 2008). Moreover, the fact that the skin of the injured digits also rewarms faster might be a sign of greater vasoreactivity of injured areas to the different thermal stimuli (cold or warm). Although the observed difference in vasoreactivity between the injured and noninjured digits was statistically significant, the width of the confidence interval suggests that the magnitude of these differences, which could in part be attributable to measurement error, are most likely physiologically irrelevant.
Thermal responses observed in the fingers
Although we did not observe any impairment of cold tolerance in the stumps in fingers, most likely due to the limited number of injured fingers (N = 6) included in the study, Ervasti et al. have described symptoms and clinical signs of impaired thermal responses in cold injured fingers. In contrast to the greater injured toe-rewarming rate compared to noninjured toes, the rewarming rate of the injured fingers was slower compared to the noninjured fingers. This has also been observed by Ruijs et al. (2009, 2011), who compared rewarming rates of healthy fingers with that of fingers after nerve injury.
It has previously been suggested that thermal responses to cold water immersion is similar for all digits (Daanen HA and van der Struijs, 2005), and therefore a cold water immersion test of one finger could predict the responses in other fingers and even toes. On this basis, the cold water immersion test of one finger has been promoted as a potential screening test for individuals that would be susceptible to cold injury in the fingers and toes. Our data confirm the conclusions of Cheung and Mekjavic (2007), that hands and feet behave differently after local cold exposure and that the CIVD response is variable across the fingers, and is not a generalizable effect across digits or limbs. This could also explain the differences in the Tsk responses during the cold stress test between the finger and toe stumps. Similarly, our data confirm recent observations of Norrbrand et al. (2017) and Kounalakis et al. (2017) that the patterns of spontaneous rewarming in fingers and toes differ as well.
Behavioral factors also significantly contribute to the etiology of finger and toe frostbite (Ervasti et al., 2004). Raza et al. (2010) observed differences in incidence of cold injury in Pakistani highlanders. On the basis of a survey of injured (chillblain) and noninjured (controls) natives, they concluded that regular hand and feet washing and reduced tea consumption was associated with greater risk of cold injury in winter months. In our sample of finger stumps, all alpinists could describe a clear reason for the development of frostbite in their hands, while they could not find any specific reason for frostbite in feet (Table 1). The number of amputated fingers compared to toes was low in our study.
Cold-induced vasodilatation
The exact role of CIVD wave frequency during cooling is not completely understood (Cheung, 2015). The Hunting response, as described almost a century ago, is a spontaneous vasodilatation pattern that may periodically establish a higher digit tissue temperature, and has therefore been suggested to be a protective mechanism against cold injury. The average temperature (mean) of injured toes (INJ) was lower than Tmean in the corresponding toes (CORR) after the cold phase, despite a higher incidence of CIVD wave/toe in INJ toes (1.5 vs. 1.07). Similarly, significantly lower incidence of CIVD waves in the NISS toes compared to NICO toes (0.38 waves/toe vs. 1.23 waves/toe) did not result in significantly lower Tmean (9.66°C vs. 9.96°C). Thus, although significant, the magnitude of the difference in the number of CIVD waves between the INJ and CORR toes, and between the NISS and NICO toes, was such that it did not influence digit Tsk and was therefore physiologically irrelevant.
Methodological issues
In some subjects, the CIVD response can be quite substantial, and it is for this reason that research has focused on factors that may augment the response. Several factors have been reported to affect the CIVD wave frequencies: cold training (Daanen et al., 2012), short term acclimatization to altitude (Daanen and van Ruiten, 2000; Felicijan et al., 2008), winter military training (Brändström et al., 2008), hypoxia (Kounalakis et al., 2017). From a methodological perspective, it has also been reported that the temperature of the water during the cold water immersion test will also affect the response (Cheung and Mekjavic, 2007). In the absence of any specific guidelines regarding the manner in which the CIVD test is performed, we used an 8°C water bath and defined a CIVD as having a minimum amplitude of 0.5°C amplitude, and lasting a minimum of 2 min (Tyler et al., 2015). The large degree of variability in the results reported by different studies could, in part, be due to the differences in the test protocols. An appropriately designed cold stress testing could be a useful clinical tool to assess the predisposition of individuals to upper or lower extremity freezing cold injury, nerve problems, or occupational injury, including those associated with vibration injury, repeat cold exposure, or people climbing to high altitude.
An issue that may also vary among studies is the site for the placement of the temperature sensors on the digits. In our study we placed thermocouples at the level of the nail bed instead of digit pad, in accordance with the suggestion of O'Brien (2005), who showed similar patterns of blood flow response between nail bed and digit pad, but the reproducibility of skin temperature responses during CIVD was better in the nail bed than in the digit pad.
Nonfreezing cold injury
Nonfreezing cold injury as an isolated injury is considered a clinical syndrome that occurs when tissues are exposed to cold temperatures, that do not induce tissue freezing (i.e., above 0°C), for extended periods of time (Francis and Golden, 1985; Imray et al., 2011). In cases where freezing cold injury requires amputations of digits, it is quite likely that the salvaged digit tissue may have also suffered the nonfreezing type of injury, and bears all the consequences and characteristics of such injury (Felicijan et al., 2008). The long-term effect of injured digits is not completely clear. Sequellae with amputations are only a visible consequence of cold injury. Where amputations did not occur, nonfreezing cold injury may leave some impairment in blood flow regulation in apparently intact digits and stumps. From our data it may be concluded that the role of nonfreezing cold injury should not be neglected. Toes of the injured limb were namely colder during the cooling phase by ∼0.7°C than toes on the noninjured side (n = 40, p < 0.001). Also, the cooling rate of the toes on the injured side was greater (by 2.1°C in 30 min) compared to the noninjured toes on the contralateral side (n = 40, p < 0.001). These changes, however, could not be found in the fingers. In fingers, the sample size was small and there may have been a greater behavioral pattern of frostbite occurrence in fingers compared to toes (e.g., alpinists are more aware of their fingers than of their toes, that are bound by footwear; frostbite in fingers occurs many times after taking off gloves for climbing maneuvers). Moreover, during cooling, the skin of the fingers of the affected limb cooled less than their counterparts in the noninjured contralateral limb. This suggests that in fingers, sequellae after injury without amputation do not represent increased risk for further cold injury. Furthermore, based on expedition documentation, it is known that some of the alpinists in our study received first aid and emergency medical treatment and hospital treatment after cold injury. The role of frostbite treatment on cold injury-sequellae and on results of further cold stress test are not known. Cold injury in hands may drive a greater urgency for any kind of treatment, thus further reducing the incidence of frostbite-amputations in hands compared to feet (Gorjanc, 2006). Any treatment of cold injury might not just reduce the probability of amputations, but also the extent of the regions with nonfreezing cold injury. Due to a hypothesized difference in the physiology of fingers and toes (Cheung and Mekjavic, 2007; Cheung, 2015) separate analyses were performed. The two analyses had substantially different sample sizes (26 INJ +26 CORR toes and 14 NISS +14 NICO toes, 6 INJ +6 CORR fingers and 9 NICO +9 NISS fingers), which could also explain the lack of statistically significant findings for fingers.
Gender and CIVD
In our study, each of the two female alpinists suffered frostbite with amputations in toes. Both of them are classified as elite climbers with international UIAA category (UIAA-International federation for climbing and mountaineering). Differences in peripheral blood flow in men and women are well known. Generally, women have lower finger blood flow due to increased vasomotor tone (Cooke et al., 1990). Additionally, in women, enhanced vascular reactivity of peripheral skin after cold exposure is attributed, in part, to estrogen. However, after total body heating in men and women, these differences disappear and peripheral blood flow is even greater in women than in men (Bartelink et al., 1993). CIVD onset and intensity in women did not show any differences in comparison with men. (Daanen, 2003). No significant differences in finger temperature response were described after testing eskimo men and eskimo women for reactions to cold air (Miller and Irving, 1962). In our two female subjects, the mean temperature values in all phases of the cold stress test (prewarming, cold water immersion, passive heating) did not differ substantially from the averages for the whole group of toes (n = 26). Moreover, the stumps (INJ) of these two alpinists during the cold phase were even slightly warmer than the average (10.3°C and 10.2°C vs. 9.93°C [Tmean], however, at the same time their noninjured counterparts [CORR]) were slightly colder than the average (11.1°C and 10.6°C vs. 11.42°C [Tmean]), but given a limited sample size, we could not test for the statistical significance of these differences.
Conclusions
We found significantly lower skin temperature of injured toes (by ∼1.5°C) compared with uninjured counterparts during the cold water immersion of the cold stress test. All toes of the injured limb showed statistically significant faster cooling during the cold phase compared to toes of the uninjured limb. Better rewarming of injured stumps in toes may be a sign of greater vasoreactivity of preinjured tissue, but this was not confirmed in the fingers. Despite significant differences in the thermal responses of the injured and noninjured toes during the cold stress test, these differences are not considered of such magnitude that they could indicate unequivocally a predisposition to cold injury. It should be noted that the cold stress test in the present study does not mimic the temperatures (subzero) and durations of exposures experienced by alpinists during climbing expeditions. The slight differences in skin temperature responses between the injured and noninjured toes observed at 8°C may be substantially augmented in more extreme environments. Thus, the differences in cold susceptibility of toe stumps, found in our study, might have greater clinical importance during cold exposure in extreme alpine climbing.
In contrast, finger stumps after freezing cold injury tended to be warmer during cooling phase compared to uninjured fingers of the contralateral side, therefore, there may not exist a greater cold injury risk for finger stumps for alpinists exposed to future cold environments.
Footnotes
Acknowledgments
The authors would like to thank the tested alpinists for participating in these tests. Without their passionate participation the project could not have been successfully concluded. We also like to thank Prof. Metka Milčinski for her help.
Author Disclosure Statement
No competing financial interests exist.