
Abstract
Abstract
Noh, Sang Jae and Ho Lee. Rapidly progressing fatal high-altitude illness in a patient with hyperthyroidism. High Alt Med Biol. 19:288–290, 2018.—High-altitude illness (HAI) refers to a broad spectrum of diseases ranging from acute mountain sickness to high-altitude cerebral and pulmonary edema that are induced by high-altitude hypoxic stress. In this study, we present a case of a rapidly progressing fatal HAI (high-altitude cerebral edema and pulmonary edema) in a patient with hyperthyroidism. The victim is a 20-year-old female being treated for Graves' disease, who died after visiting a high-altitude region for travel. The autopsy examination showed cerebral and pulmonary edema, and right ventricular enlargement. A postmortem thyroid function test revealed thyrotoxic status; thyrotoxicosis may have contributed to the rapid progression of the HAI.
Introduction
H
Case Report
The victim is a 20-year-old Korean female, who had been treated for hyperthyroidism caused by Graves' disease for 2 years. She visited China to attend an educational program and stayed at a low altitude area for 3 weeks. After 3 weeks, she visited a high-altitude region, Jiuzhaigou in China, for travel; Jiuzhaigou is located at an altitude of ∼3500 m. She did not receive any preventive medication for HAI, except for a Rhodiola extract compound; a Chinese herbal drug used for prevention of mountain sickness. She moved to the high region by a bus without any prior acclimatization; and the altitude change was from 500 to 3500 m. When she arrived at the high-altitude region, she started complaining of nausea and vomiting. Ten hours after arrival, she lost consciousness, and respiratory arrest occurred during sleep at the place where she stayed. Although emergency treatment and resuscitation were carried out, she died before arriving at the hospital. The victim was sent back to Korea and a medicolegal autopsy was performed.
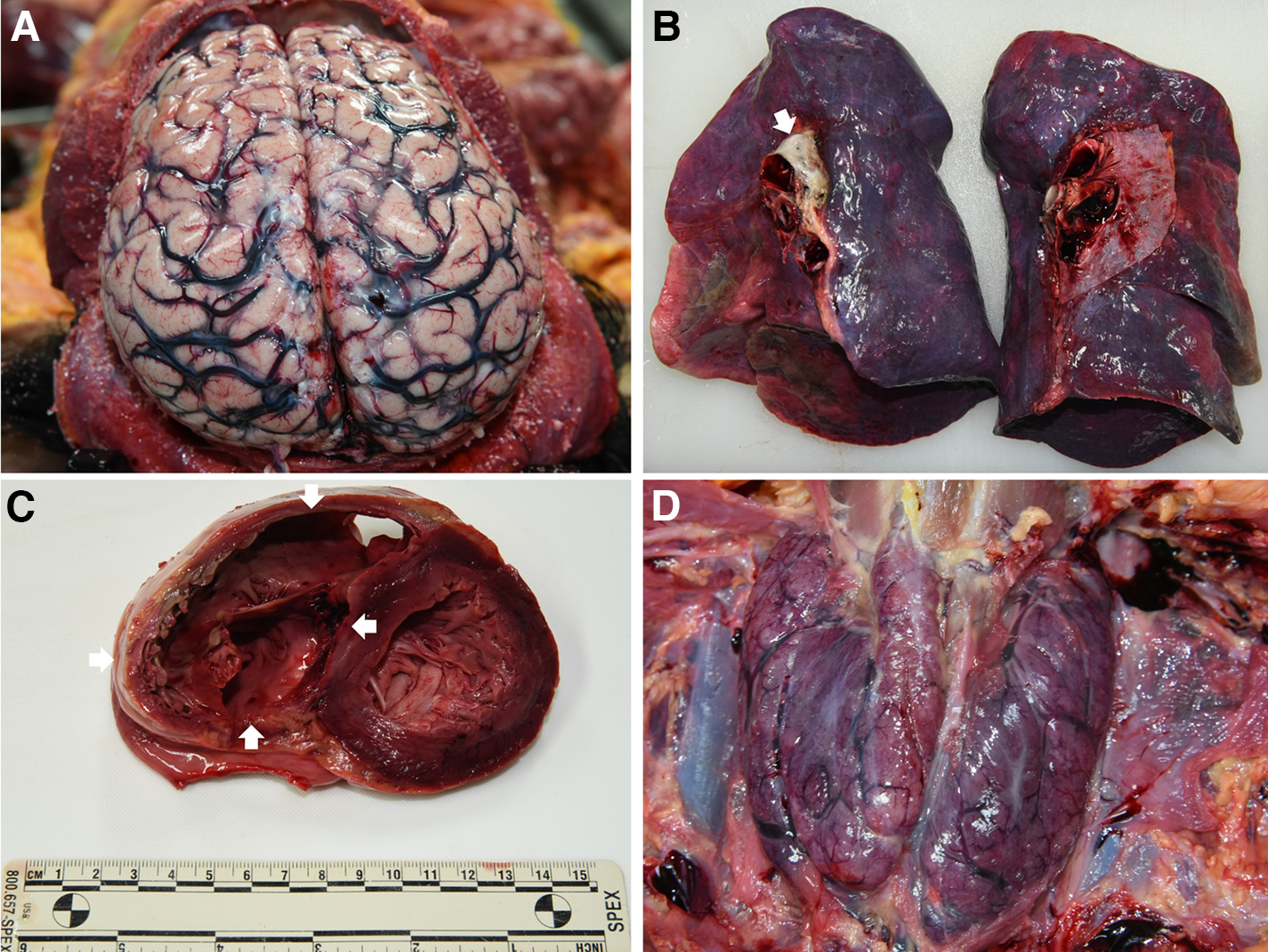
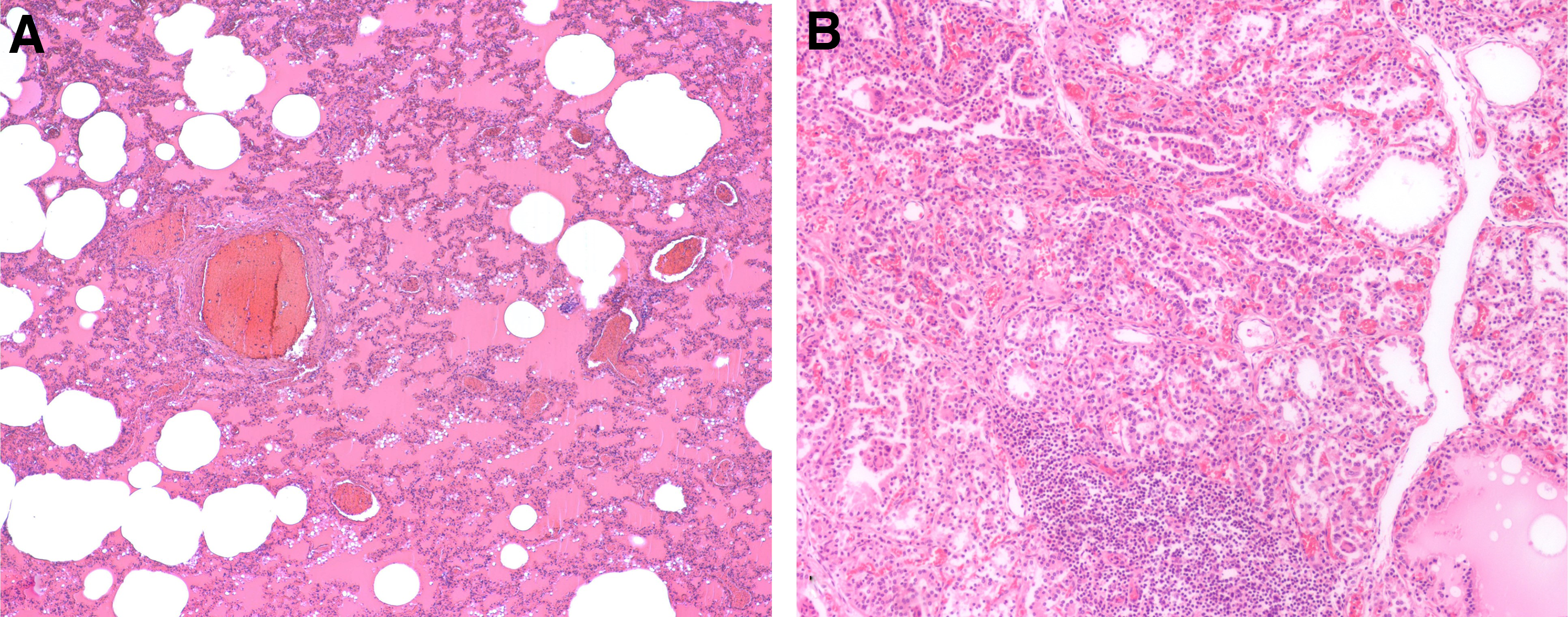
In the autopsy examination, diffuse and bilateral swelling of the brain with an effacement of the sulci was observed (Fig. 1A). Both lungs were edematous and expanded with edema froth formation in the trachea and bronchus (Fig. 1B). The heart weighed 397 g, and the right ventricular cavity was significantly dilated compared with the left ventricular cavity (Fig. 1C). Pathologic examination of the brain and lungs revealed interstitial edema, vascular congestion of the cerebral and pulmonary vasculatures, and intra-alveolar fluid accumulation (Fig. 2A). The thyroid gland was remarkably enlarged and weighed 66 g (Fig. 1D). Pathologic examination of the thyroid showed diffuse hyperplasia of the thyroid follicular epithelial cells; the histological features are consistent with Graves' disease (Fig. 2B). Because postmortem values of thyroid hormones are comparable with premortem clinical values (Edston et al., 2001), a postmortem thyroid function was tested with electrochemiluminescence immunoassay by using a femoral venous blood taken at autopsy. The thyroid function test revealed a thyrotoxic status: free T4, 35.78 nmol/L (normal range, 9.0–16.0 nmol/L); total T4, 123.57 nmol/L (normal range, 70–151 nmol/L); total T3, >9.0 nmol/L (normal range, 1.2–2.1 nmol/L); and thyroid-stimulating hormone (TSH), <0.001 mIU/mL (normal range, 0.34–4.25 mIU/mL). Anatomic and pathologic examinations showed no evidence of encephalitis, myocarditis, congenital heart disease, valvular heart disease, pneumonia, or pulmonary thromboembolism. In addition, other possible lethal diseases, infection, or injuries were ruled out as the cause of death. Based on the patient's history and autopsy findings, we made a diagnosis of sudden death from HAI (HACE and pulmonary edema) in a patient with hyperthyroidism.
Discussion
In general, individuals who travel to places with altitudes >2500 m are at risk for HAI (Zafren, 2014). As previously mentioned, HAI is classified into AMS, HACE, and HAPE according to the clinical manifestations of the affected organ. AMS and HACE are a series of disease processes with the same pathophysiologic etiology and can be classified according to the severity of the disease. AMS is the most common form of HAI. AMS is characterized by nonspecific symptoms such as nausea, vomiting, anorexia, headache, malaise, fatigue, dizziness, and sleep disturbance, and can progress to fatal HACE (Basnyat and Murdoch, 2003; Bärtsch and Swenson, 2013). HACE is characterized by neurologic signs and symptoms, including ataxia, severe lassitude, progressive deterioration of mental function, and coma, and without descent or treatment death can result from brain herniation (Basnyat and Murdoch, 2003; Bärtsch and Swenson, 2013). HAPE is the most common cause of death from HAI and generally begins with a subtle and nonproductive cough and exertional dyspnea. The incidence rate of HAPE ranges from ∼0.01% to 5% according to altitude (Hall et al., 2011). Progression from AMS to HACE usually takes 24–36 hours, although sometimes it only takes a few hours. In this case, the victim only presented with AMS symptoms, including nausea and vomiting at the early stage. However, the victim suddenly lost consciousness and died within 10 hours of arrival to the high-altitude region. AMS rapidly progressed to HACE, and the development of HAPE was extremely fast without prodromal respiratory signs. HACE and HAPE were proved at autopsy. Dilatation of the right ventricle also indicates pulmonary vasoconstriction, pulmonary arterial hypertension, and acute cor pulmonale (Lankford et al., 2014).
The risk factors for developing HAI include fast ascent, ascending to a high altitude, individual susceptibility, a history of HAI, residence at an altitude <900 m, exertion, lack of previous acclimatization, and preexisting cardiopulmonary conditions (Basnyat and Murdoch, 2003; Bärtsch and Swenson, 2013). The case of the victim was associated with multiple risk factors, including residence at a low altitude, fast ascent through a bus, and lack of proper acclimatization or drug prophylaxis.
An underlying medical condition can increase the risk for developing HAI, and an underlying medical condition can be adversely affected by the hypoxic environment at high altitude (Luks and Hackett, 2014). Physiologically, hypoxic conditions and cold exposure at high altitude induce the increase of thyroid hormone, including free and total T4 and T3, independent of TSH. Increased thyroid function plays a role in long-term adaptation to hypoxia and cold environment and could play a protective role against development of HAPE (Richalet et al., 2010; Richalet, 2014). According to the police record and the family's testimony, the victim was being treated for hyperthyroidism caused by Graves' disease, and her hyperthyroidism was well-controlled with a maintenance dose of methimazole before visiting China. However, during her 3-week stay in China, she took her antithyroid medication irregularly, and the postmortem thyroid function test revealed a status of hyperthyroidism. In this situation, the relapse of hyperthyroidism and accompanying thyrotoxic crisis should be considered. Hyperthyroidism is associated with increased oxygen consumption, and enhanced cardiac contractility and output, thus leading to increased cerebral and pulmonary blood flow, exaggerated capillary pressure, and subsequently edema formation. A thyrotoxic crisis is a rare, life-threatening medical emergency with exaggerated symptoms of thyrotoxicosis, and it is often precipitated by the unreliable use or discontinuation of an antithyroid drug, infection, acute illness, thyroid or nonthyroid surgery, trauma, and stress (De Leo et al., 2016). Tough environmental condition of the high altitude or accompanying HAI may promote the development of the thyrotoxic crisis; subsequent thyrotoxicosis may have contributed to the rapid progression of HAI.
Even if the clinical presentation and pathophysiology of HAI have been well documented, fatal HAI with rapid progression is extremely rare, and the effect of variable underlying medical conditions on the development and progression of HAI should be elucidated. This case report serves to highlight that HAI can rapidly progress, culminating in death, at even modest altitude. The coexistent thyroid condition with biochemical evidence of thyrotoxicosis at the time of death raises the possibility that this could have been a factor in the onset and/or rate of progression of the HAI.
Footnotes
Acknowledgment
The authors thank Dr. K.A. Lee for the review and advice of endocrinology.
Author Disclosure Statement
No competing financial interests exist.