
Abstract
Abstract
Lundeberg, Jenny, John R. Feiner, Andrew Schober, Jeffrey W. Sall, Helge Eilers, and Philip E. Bickler. Increased cytokines at high altitude: lack of effect of ibuprofen on acute mountain sickness, physiological variables or cytokine levels. High Alt Med Biol. 19:249–258, 2018.
Introduction:
There is no consensus on the role of inflammation in high-altitude acclimatization.
Aims:
To determine the effects of a nonsteroidal anti-inflammatory drug (ibuprofen 400 mg every 8 hours) on blood cytokines, acclimatization, acute mountain sickness (AMS, Lake Louise Score), and noninvasive oxygenation in brain and muscle in healthy volunteers.
Materials and Methods:
In this double-blind study, 20 volunteers were randomized to receive ibuprofen or placebo at sea level and for 48 hours at 3800 m altitude. Arterial, brain, and leg muscle saturation with near infrared spectroscopy, pulse oximetry, and heart rate were measured. Blood samples were collected for cytokine levels and cytokine gene expression.
Results:
All of the placebo subjects and 8 of 11 ibuprofen subjects developed AMS at altitude (p = 0.22, comparing placebo and ibuprofen). On arrival at altitude, the oxygen saturation as measured by pulse oximetry (SpO2) was 84.5% ± 5.4% (mean ± standard deviation). Increase in blood interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), interleukin-10 (IL-10), tumor necrosis factor-α (TNF-α), and granulocyte-macrophage colony-stimulating factor (GM-CSF) levels occurred comparably in the placebo and ibuprofen groups (all not significant, univariate test by Wilcoxon rank sum). Increased IL-6 was associated with higher AMS scores (p = 0.002 by Spearman rank correlation). However, we found no difference or association in AMS score and blood or tissue oxygenation between the ibuprofen and placebo groups.
Conclusions:
We found that ibuprofen, at the package-recommended adult dose, did not have a significant effect on altitude-related increases in cytokines, AMS scores, blood, or tissue oxygenation in a population of healthy subjects with a high incidence of AMS.
Introduction
E
Several studies have investigated the possible involvement of inflammation in the pathogenesis of high-altitude illnesses, both in terms of symptom development and pathophysiological components. Elevated levels of proinflammatory cytokines have been found in hypoxic subjects during ascent and sojourn at high altitude (Klausen et al., 1997; Hartmann et al., 2000; Boos et al., 2016; Song et al., 2016).
The reduction of AMS symptoms with anti-inflammatory agents such as steroids (e.g., dexamethasone) and nonsteroidal anti-inflammatory drugs (NSAIDs) supports a role for inflammation in AMS symptom pathogenesis (Hackett et al., 1998; Dumont et al., 2000; Gertsch et al., 2012; Lipman et al., 2012; Shideran and Sivaramakrishnan, 2018). Ibuprofen and acetaminophen equally reduce AMS incidence, suggesting that AMS prevention is multifactorial as symptoms are reduced both through anti-inflammatory inhibition of the arachidonic-acid pathway and mediation of nociception in the brain (Kanaan et al., 2017).
Ibuprofen, a commonly used NSAID, has been shown in two large studies to decrease incidence of AMS (Gertsch et al., 2012; Lipman et al., 2012). Both these studies used larger doses of ibuprofen than recommended on the over the counter package label (e.g., Motrin®; Johnson and Johnson, New Brunswick, NJ), and although these larger doses will have a stronger anti-inflammatory effect, their applicability to the casual traveler, who will probably use the recommended dosing, is uncertain. Furthermore, NSAIDs have recognized side effects of decreased renal function and gastrointestinal (GI) bleeding that may be more severe at higher doses. The GI side effects are relevant because gastric erosions and bleeding are associated with ascent to high altitude (Wu et al., 2007a, 2007b; Fruehauf et al., 2010). Based on these considerations, our study was designed to test the effect of standard dose ibuprofen (400 mg three times a day) on altitude-related symptoms and cytokines. This lower dose range of ibuprofen may have a benefit in reducing headache, and if so, it may lower AMS incidence or severity. We also wished to determine if the 400 mg three times a day dose of ibuprofen reduced cytokine levels.
In addition to causing symptoms of AMS, inflammation may play a key role in the increases in ventilation, driven by increased carotid body chemosensitivity, that accompany acclimatization to altitude. A number of studies have documented increased cytokines and cytokine gene expression in the carotid body during exposure to acute or chronic hypoxia (Lam et al., 2008; Liu et al., 2009; Kahlin et al., 2014). Consistent with this, administration of anti-inflammatory drugs prevents increased cytokine expression and increase in carotid body chemosensitivity in animals (Liu et al., 2009; Kahlin et al., 2014). Based on such observations, several studies have examined the effects of NSAIDs on ventilatory acclimatization to chronic hypoxia and high altitude in laboratory animals and humans. Popa et al. (2011) studied the effects of ibuprofen on hypoxic ventilatory response (HVR) in chronically hypoxic rats. The HVR is an increase in ventilation and considered a cardinal feature of acclimatization to hypoxia (West, 2004; Teppema and Dahan, 2010). Popa et al. (2011) found that the anti-inflammatory drug, ibuprofen, reduced the increase in HVR, in contrast to normoxic control rats where ibuprofen had no effect on ventilation. The same study found that ibuprofen blocked the elevation of inflammatory cytokine levels (interleukin-1β [IL-1β] and interleukin-6 [IL-6]) in the brainstem of rats exposed to chronic hypoxia. Basaran et al. (2016) studied the effects of package-recommended doses of ibuprofen (400 mg every 8 hours) on HVR in humans during acclimatization, finding a blunting of the normal increase in HVR during acclimatization. Taken together, information from previous studies suggests that although NSAIDs might alleviate AMS symptoms, reduction in inflammation from these agents might delay ventilatory acclimatization and negatively impact blood and tissue oxygenation during the acclimatization process.
The aim of this study was to investigate the effects of an NSAID (ibuprofen) on time-dependent changes in parameters related to acclimatization. The primary outcome was cytokine levels, with secondary outcomes AMS scores and incidence, cytokine gene expression, blood and tissue (leg muscle and brain) oxygenation, and heart rate (HR). Our hypothesis was that treatment with ibuprofen would result in reduced cytokine levels and AMS, but a lower oxygenation in peripheral blood, leg muscle, and brain tissue as a result of the previously demonstrated delay in augmentation of HVR by the same dose of ibuprofen during acclimatization.
Materials and Methods
Participants
This trial was performed on 20 healthy volunteers. Nine subjects were studied in 2014 and 11 different subjects were studied in 2016, under identical conditions and study protocol. The trial was approved by the Committee on Human Research at University of California, San Francisco (UCSF), and all subjects gave written informed consent. To be included in the study, the subjects needed to be between 18 and 65 years, considered healthy and fulfill the study criteria. The latter was determined through a brief medical history performed by a study physician. Questions included medical and surgical history, current medications and allergies, history of substance abuse, and history of difficulties during previous visits to high altitude. Exclusion criteria included the following: pregnancy, inability to take NSAIDs (e.g., allergy and inflammatory bowel disease), previous substance abuse, earlier episodes of severe high-altitude illness, and sojourn at altitude during the last 6 months. All subjects completed the study.
Study design
This randomized and double-blind placebo controlled clinical trial consisted of two cohorts (in 2014 and 2016) using the same study protocol except determination of gene expression for some specific cytokines in the 2014 study and the addition of leg muscle oximetry in the 2016 study. The high-altitude portions of the studies were executed at the Pace Laboratory at the Barcroft Station at the White Mountain Research Center located in the White Mountains in California, elevation 12,470 feet or 3800 m. The sea level portions of the studies were done at the UCSF, elevation 400 feet or 122 m (“sea level”). The study took place over 6 days for each participant: 4 days traveling and residing at altitude and 2 days at sea level ∼8 weeks after the altitude session.
A power analysis was performed based on the primary study endpoint of a reduction in cytokines by ibuprofen compared with placebo groups. The primary source for the assumptions involved was Song et al. (2016) who noted a pooled increase in tumor necrosis factor-α (TNF-α), IL-1β, and IL-6 of 80% from low altitude (540 m) to high altitude (3860 m). The pooled standard deviation (SD) of cytokine level increase was 36% of the means at 3860 m. The effect of ibuprofen on cytokines at altitude has not been studied. We therefore made the assumption that ibuprofen would have the same effect on cytokine levels as it does on AMS incidence, that is, a 40% reduction (from an incidence of 40.4%–24.4%), based on the study by Gertsch et al. (2012). Targeting a p value of 0.05, a reduction in cytokine levels with a one-tailed test, would therefore require a pool of about 20 total subjects to have an 80% chance of finding a significant effect of ibuprofen, assuming a 20% SD. Of note, Basaran et al. (2016) found that our dose of ibuprofen significantly prevented ventilatory acclimatization to altitude in a study of 15 subjects.
All study participants were randomly assigned to receive placebo or ibuprofen. Ibuprofen and placebo pills were placed in identical colored gelatin capsules to disguise the type of drug that was administered. The randomization was performed through coin toss and was blinded until data analysis. The dose of ibuprofen was set to 400 mg three times daily, which is the recommended adult dosage specified on the package insert. Participants were instructed to administer drugs at 8 am, 4 pm, and 10 pm for 2 days. Tests were executed at four time points at altitude and two time points at sea level. Tests included AMS scoring, clinical parameters, and venous blood sampling. The subjects were asked not to take any acetazolamide, corticosteroids, aspirin, or NSAIDs 48 hours before each part (altitude and sea level) and caffeinated beverages were limited to one cup of coffee or tea, after tests, each day.
The altitude ascent profile for all the subjects was identical. Participants ascended to altitude together by car from sea level to 1260 m elevation in about 6 hours, then from 1260 to 3800 m in 2 hours, all in the same day. Drug administration was initiated in Bishop, CA at 1260 m of altitude during ascent to Barcroft Laboratory. The tests at altitude were performed upon arrival at the Barcroft laboratory (3800 m) and after 12, 36, and 60 hours at altitude. Each participant was tested ∼1 or 2 hours after drug administration. The 60-hour altitude testing was performed after the discontinuation of drugs to investigate any possible effects of terminating ibuprofen while at altitude. Participants were instructed not to perform any extreme physical activity at altitude but were allowed to take short hikes. Sea level testing was done ∼8 weeks after descent. Tests were executed ∼18 and 36 hours after drug/placebo administration was initiated and an average of the results of the two sea level sessions was used as “sea level baseline” for all parameters.
Assessment of AMS symptoms
During each study session at altitude the subjects evaluated the presence and severity of AMS symptoms using the Louise Lake AMS Scoring System (Roach et al., 1993). At the first study session, upon arrival at altitude, there was no evaluation of sleep quality since the subjects not yet had slept at altitude. The subjects were asked to score the worst symptoms they experienced since the last study session. In line with the Lake Louise AMS Scoring System, a total score of 3 or higher, where headache was included, was considered as AMS.
Clinical measurements
To measure peripheral and cerebral oxygenation, we used a Radical-7 finger pulse oximeter (Masimo SET®, Irvine, CA) and a FORE-SIGHT® tissue oximeter (CAS Medical Systems, Branford, CT). LabVIEW® (v. 2013; National Instruments, Austin, TX) was used for data visualization, and each participant was recorded for ∼300 seconds. HR and respiratory rate were also documented. The pulse oximeter probe was placed on the same finger during all study sessions. The probe for cerebral oximetry was placed on the left side of the forehead. Leg muscle oxygenation was assessed in the 11 subjects during the 2016 study using FORE-SIGHT tissue oximeter (CAS Medical Systems). The oximetry sensor was placed over the tibialis anterior muscle. The leg was elevated to the level of the pelvis and was at rest during the 5-minute measurement period.
Cytokine analysis
At each time point of testing, a venous blood sample was drawn for later analysis of cytokine levels and cytokine gene expression. Six milliliters of blood were collected into a vacutainer tube containing lithium heparin. The tube was put on ice for 5 minutes before it was centrifuged for 12 minutes with a relative centrifugal force of 1690 g. Thereafter, 1 mL of plasma was collected and placed in a 1 mL Eppendorf tube, marked with initials and date, and immediately stored in a freezer. The samples were initially stored at −28°C at altitude, on dry ice during transportation and in a −80°C freezer at sea level. In addition, 3 mL of blood was collected in Tempus™ Blood RNA Tubes (Applied Biosystems), shaken for 10 seconds, and preserved in a −28°C freezer at altitude, with dry ice during transportation back to sea level.
For quantification of cytokines, we used the Discovery Assay Human Cytokine/Chemokine 11-plex Array from Eve Technologies (Calgary, Canada). The technique for the array was based on color-coded polystyrene beads. Bead coloration was achieved by utilizing different concentrations of red and infrared fluorophore dyes creating 100 uniquely colored bead sets. The assay involved a Bio-Plex 200 bead analyzer (Bio-Rad Laboratories, Hercules, CA), which includes a dual-laser system in combination with a flow-cytometry system. The amount of conjugate detected by the analyzer was in direct proportion to the amount of the target analyte. The cytokine levels from 2014 and 2016 were analyzed on separate but similar arrays. Only cytokines assayed on both arrays are reported, and these included the interleukins IL-1β, IL-6, interleukin-8 (IL-8), interleukin-10 (IL-10), as well as TNF-α, interferon gamma (IFN-γ), and granulocyte-macrophage colony-stimulating factor (GM-CSF). All samples were run singly and the results were quantified according to a standard curve. The Eppendorf tubes with frozen plasma were shipped on dry ice to Eve Technologies.
For analysis of cytokine gene expression from the 2014 study samples, a custom RT2 profiler polymerase chain reaction (PCR) array (SA Biosciences, Qiagen, Inc.) was used. The array estimated messenger RNA (mRNA) levels for a total of 12 genes. In addition to the previously specified cytokines IL-1β, IL-6, and TNF-α, mRNA levels for nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), two positive controls, two reverse transcription controls, and one human genomic DNA contamination gene was determined. Beta-2-microglobulin (B2M), glyceraldehyde-3-phosphate-dehydrogenase (GAPDH) and ribosomal protein large p0 (RPLP0) were housekeeping genes included in the array. These genes were chosen in line with SA Biosciences' current suggestions for arrays quantifying genes for cytokines as well as for hypoxia signaling pathways. Thus, the housekeeping genes were included to normalize the genes for NF-κB and the cytokines mentioned above. The PCR array plate format used was a 384-well plate, which allowed 32 samples per plate. For processing of stabilized blood and RNA purification Tempus Spin RNA Isolation Reagent Kit (Applied Biosystems) was used. The frozen samples in the Tempus Blood RNA Tubes were thawed at room temperature and kept on ice during processing and purification to prevent RNA degradation. RNA was converted to complementary DNA (cDNA) with assistance of RT2 First Strand Kit (SA Biosciences), and thereafter, cDNA was added to RT2 SYBR Green MasterMix (SA Biosciences) before the mix was aliquot into the custom RT2 profiler PCR arrays. For detection and quantification of mRNA levels, a 7900HT Fast Real-Time PCR system with a 384-well block module was used (Applied Biosystems, Life Technologies, Grand Island, NY). To avoid false patterns due to differences in plate quality, the samples were randomly located in the plates. The samples from altitude and sea level were allocated on separate plates. All samples were run in triplicate.
Statistical analysis
Descriptive statistics, including mean, SD, and median were used to visualize immediate trends and patterns. For univariate comparisons, Fisher's exact test was used to compare proportions between groups. Shapiro–Wilk test was used for test of distribution of continuous variable, and t-test or Wilcoxon rank sum was used to compare groups.
The primary statistical analysis was a two-way repeated measures analysis of variance (ANOVA), with repeated measures over time (day at altitude), the between-group comparison (placebo vs. NSAID), and the interaction. Results of one-way repeated measures ANOVA are also shown within groups and for the entire cohort. Tukey's HSD (Honest Significant Difference) test was used for all post hoc multiple comparisons. Spearman's rank correlation was used for simple correlations between AMS scores with physiological variables and cytokines.
Data are shown as mean ± SD, median (interquartile range) or number (percent) as indicated. Stata 14.2 (StataCorp, College Station, TX) and JMP 11.0 (SAS Institute, Cary, NC) were used for analysis. All statistical tests were two tailed. A p-value <0.05 was considered significant.
Results
Subjects were between 23 and 61 years old, with an average of 33 years, and subject characteristics were similar in the ibuprofen and placebo groups (Table 1). During sojourn at altitude, 17 out of 20 subjects scored positive for AMS at some point, with 9 of 9 subjects in the placebo and 8 of 11 in the ibuprofen group meeting the criteria. This was not different between groups (p = 0.22). Although the placebo group reported numerically higher AMS scores than the ibuprofen group at all points during the medication phase of the altitude exposure, this was not statistically significant for any points in time (Table 2). On arrival, the subjects had not yet slept at altitude and the sleep quality was scored as zero, so the total score only reflects the other symptoms. Upon arrival at altitude, 33.3% in the placebo group and 18.2% in the ibuprofen group had AMS (Table 2). The incidence of AMS was greatest after 60 hours of altitude (78% of placebo and 64% of ibuprofen subjects), which was 12 hours after the last dose of ibuprofen or placebo.
SD, standard deviation.
AMS evaluation method used was Lake Louise AMS Scoring System. A score ≥3 including headache as a mandatory symptom was considered as AMS. p-Value between groups by Fisher's exact test. p-Value (within) is from the repeated-measures ANOVA over time at altitude.
AMS, acute mountain sickness; ANOVA, analysis of variance.
Figure 1 contains information on the incidence of AMS score components at different times at altitude for the ibuprofen and placebo groups. Total AMS score varied significantly over time (pooled analysis, p = 0.03). Headache was higher numerically in the placebo group during drug treatment, although this did not reach statistical significance. The two-way repeated measures ANOVA for headache showed statistically significant differences over time (p = 0.007) but without significant interaction with treatment (Fig. 1, statistical summary in lower panel).
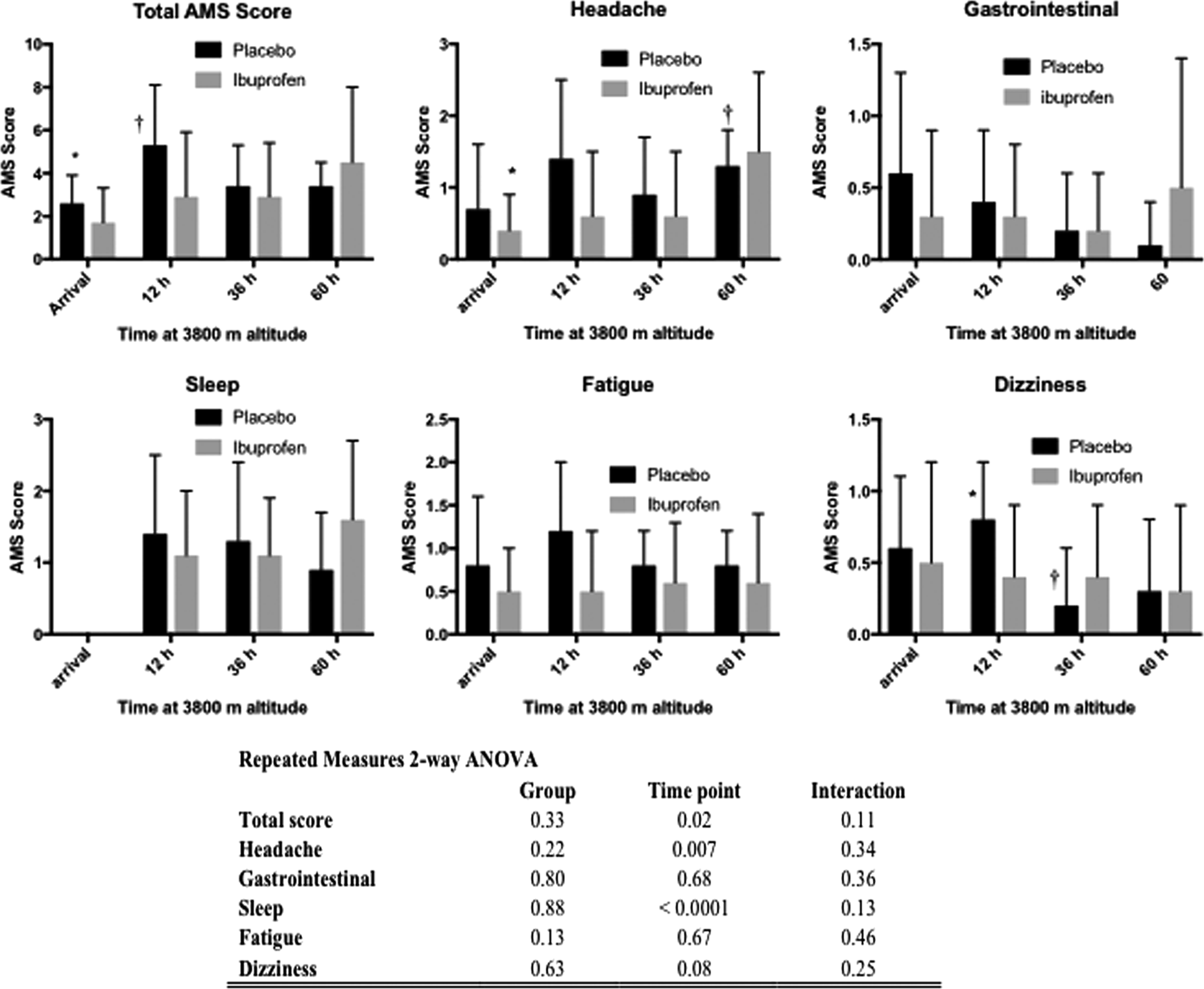
AMS scores at the Barcroft Station, 3800 m/12,470 feet) for the placebo (n = 9) and ibuprofen (n = 11) groups. Data are shown for the time points of arrival and 12, 36, and 60 hours at altitude. Data are mean ± SD. No statistically significant differences were found between the groups were found by univariate Wilcoxon rank sum tests. *Indicates statistically differs from † by repeated measures ANOVA over time within the groups, followed by multiple comparisons with Tukey HSD. The complete two-way repeated measures over time with between-group comparisons is shown in the table (inset). AMS, acute mountain sickness; ANOVA, analysis of variance; HSD, Honest Significant Difference; SD, standard deviation.
At high altitude, oxygen saturation was significantly lower than at sea level with an average reduction of 13.5% (p < 0.0001) and improved significantly over time at altitude in both the ibuprofen and placebo groups (Fig. 2). Significant increases in HR (increase of ∼9 beats per minute) and decreases in cerebral oxygenation (decrease of ∼4%) were also observed. However, there were no differences in peripheral oxygenation, cerebral oxygenation, leg muscle oxygenation, or HR between the placebo and ibuprofen groups at any time points in the study (Fig. 2, statistical summary in lower panel).

Physiological parameters at sea level and altitude (Barcroft Station, 3800 m/12,470 feet) for the placebo and ibuprofen treatment groups. Data are mean ± SD. p-Values between are from univariate test by Wilcoxon rank sum test and p values (within) are from repeated measures ANOVA over time within the column, followed by multiple comparisons with Tukey HSD. *Indicates statistically differs from † by repeated measures ANOVA over time within the groups, followed by multiple comparisons with Tukey HSD. The two-way repeated measures over time with between-group comparisons is shown in the table (inset). ScO2, cerebral oxygen saturation; StO2, muscle tissue oxygen saturation.
Increases in 6 of the 7 cytokines (IL-1β, IL-6, IL-8, IL-10, TNF-α, and GM-CSF) at altitude compared to sea level baseline were observed. Table 3 pools all study subjects at sea level and altitude, and Figure 3 presents cytokine levels at the various study time points for the ibuprofen and placebo groups. Only IFN-γ was not increased at altitude compared to sea level in at least one of the treatment groups. No significant difference in cytokine levels between placebo and ibuprofen groups was present at any of the time points at altitude or at sea level (nonparametric test or repeated measures one-way and two-way ANOVA). Table 4 contains information about the expression of cytokine gene mRNA at sea level and altitude for the 2014 study participants. Overall, relatively small fluctuations in mRNA levels for IL-1β, IL-6, TNF-α, and NF-κB1 were observed in the study, with no significant differences between the ibuprofen and placebo groups.
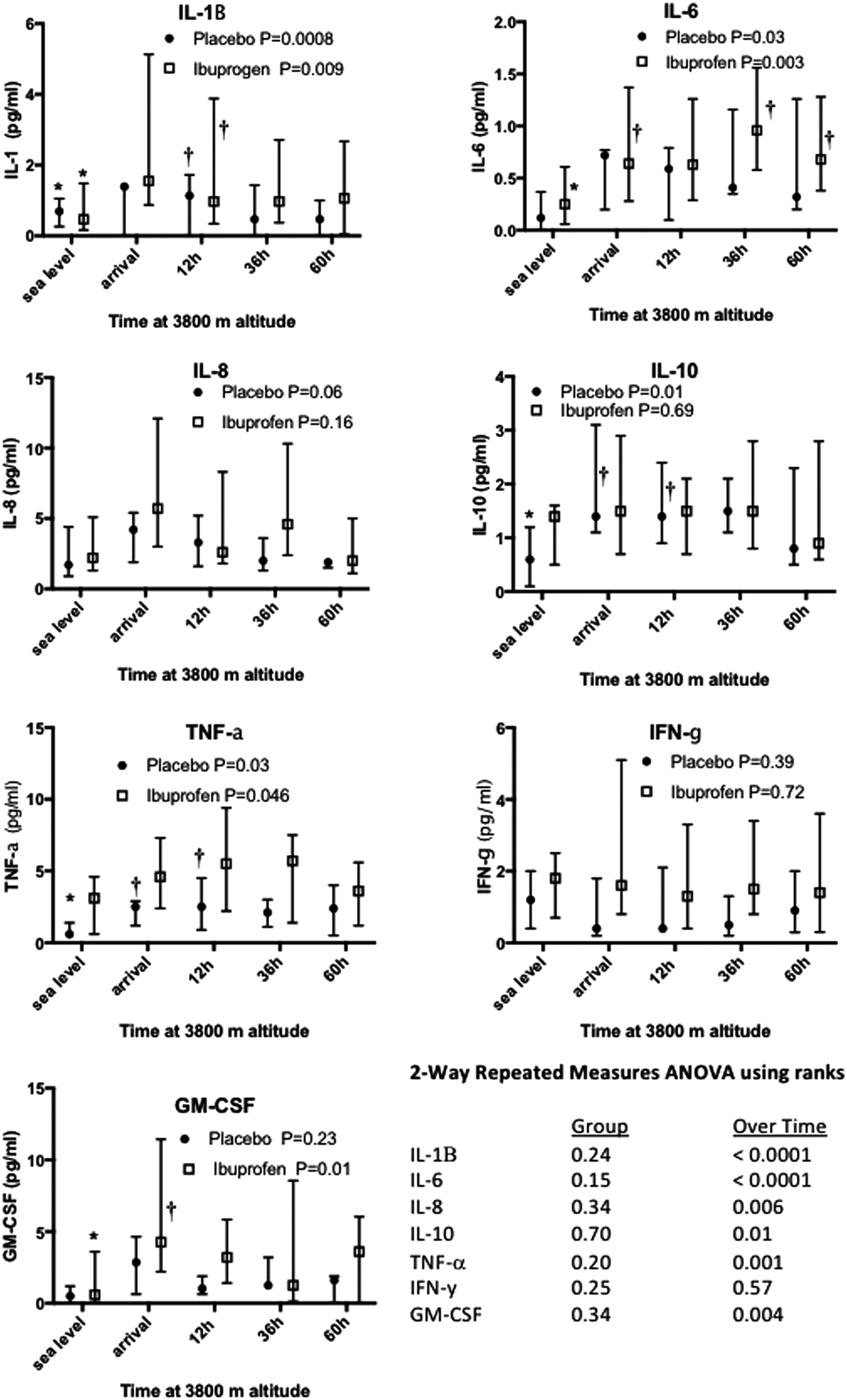
Cytokine levels in blood at specified time at sea level and altitude (Barcroft Station, 3800 m) in the placebo and ibuprofen groups. The data shown are median and interquartile ranges. There were no significant differences between the placebo and ibuprofen groups for any of the time points (univariate test by Wilcoxon rank sum). The p values shown with the legends are repeated measures ANOVA over time within groups, followed by multiple comparisons with Tukey HSD. *Indicates statistically differs from † by repeated measures ANOVA over time within the groups, followed by multiple comparisons with Tukey HSD. The two-way repeated measures over time with between-group comparisons is shown in the table (inset). GM-CSF, granulocyte-macrophage colony-stimulating factor; IL, interleukin; TNF, tumor necrosis factor.
Data are pooled values (pg/mL) for placebo and ibuprofen groups. Data are median (interquartile range). p-Values are from a repeated-measures ANOVA on rank data.
GM-CSF, granulocyte-macrophage colony-stimulating factor; IFN, interferon; IL, interleukin; TNF, tumor necrosis factor.
Data are median (interquartile range). p-Values between are from univariate test by Wilcoxon rank sum test. p-Values are from a repeated-measures ANOVA on rank data.
NF-κB1, nuclear factor kappa-light-chain-enhancer of activated B-cells.
Using Spearman's rank correlation test, we found a significant correlation between increased IL-6 and total AMS score (Spearman's rho 0.32, p = 0.002, pooling all subjects) and a negative association between GM-CSF and AMS (Spearman's rho −0.23, p = 0.03). The maximum values of IL-6 and AMS scores for each individual were also associated (Spearman's rho 0.48, p = 0.03). None of the other cytokines was related to AMS. Total AMS score was also related to both oxygen saturation as measured by pulse oximetry (SpO2; Spearman's rho −0.64, p < 0.0001) and HR (Spearman's rho 0.31, p = 0.001).
Discussion
The primary outcome of the study was cytokine levels at high altitude, and we report a positive association between AMS scores and IL-6. However, we did not find that ibuprofen changed cytokine levels. A number of previous studies have documented increases in proinflammatory cytokines at altitude, including IL-6 (Klausen et al., 1997; Boos et al., 2016; Song et al., 2016). Furthermore, higher levels of interleukin receptor antagonist (IL-RA), a highly competitive antagonist of the proinflammatory cytokine IL-1, have been found in AMS-resistant subjects but not in AMS-sensitive subjects (Julian et al., 2011). However, some argue that the elevation of cytokines occurs after onset of AMS and thus the time course of the inflammatory response argued against a role of inflammation in AMS (Hartmann et al., 2000). Furthermore, an older study shows unchanged concentrations of proinflammatory cytokines in response to hypoxia (Swenson et al., 1997). Hence, there are conflicting results on the inflammatory response at altitude. In this study, we observed increases in the cytokines IL-1β, IL-6, IL-8, IL-10, TNF-α, and GM-CSF at high altitude, but there was no difference in cytokine levels between the placebo and ibuprofen groups at altitude or sea level. Hence, the results suggest that although cytokine levels are increased at altitude, and at least in the case of IL-6 are correlated with AMS scores, a 400 mg three times a day dose of ibuprofen does not change that. However, it is likely that our study was underpowered to find such an effect. Based on clearly elevated plasma cytokine levels, correlation of IL-6 to AMS scores and upregulated gene expression of some specific cytokines, we conclude that there is a process of inflammation induced in response to ascent to altitude.
This study reports a high incidence of AMS. Out of 20 participants, 17 (85%) scored positive for AMS at some time point at altitude. Previous studies report incidence rates between 24% and 65%, depending on altitude reached and ascent profile (Honigman et al., 1993; Gertsch et al., 2012; Lipman et al., 2012). The high incidence in this study could to some extent be explained by the rapid ascent by car over only a few hours. For comparison between groups AMS incidence at certain time points was calculated and showed no significant difference between ibuprofen and placebo groups. Two large studies on AMS prevention have shown ibuprofen to effectively reduce incidence of AMS. Lipman et al. (2012) found statistically robust protection of AMS with a higher dose of ibuprofen (600 mg every 8 hours), and in the ASCENT (Altitude sickness in climbers and efficacy of NSAIDs trial) study by Gertsch et al. (2012), prevention of AMS with the same dose of ibuprofen was shown through intent-to-treat analysis. Kanaan et al. (2017) compared the efficacy in AMS reduction between ibuprofen 600 mg and acetaminophen 1000 mg and showed that AMS incidence was reduced by both substances (19% compared to historical incidence of 33%) but with no difference in incidence between groups. It is possible that this study was underpowered to detect differences in incidence between ibuprofen and placebo groups, with a 400 mg every 8-hour dosing. A post hoc power analysis for the observed effect of ibuprofen on AMS score reduction at the 12-hr at altitude time point (reduction in AMS score of 5.3 ± 2.8 to 2.9 ± 3.0) would require 23 subjects for 80% power and 31 for 90% power. This was a 43% reduction, but the SD was larger than anticipated in our initial power analysis.
Some subjects in the ibuprofen group were observed to experience an increase in AMS symptoms when ibuprofen was discontinued (Fig. 1). Although this was dramatic to the investigators and subjects, the changes in AMS scores were not statistically significant. In these subjects, the sudden aggravation of headache after termination of drugs suggests that the symptoms in the ibuprofen group were blunted by ibuprofen up until the fourth day. The masking of altitude sickness by ibuprofen (i.e., by reducing headache) has been raised by previous researchers (e.g., Gertsch et al., 2012), but to our knowledge, quantification of this effect after drug cessation at altitude has not been studied specifically. It should be taken in consideration that this study did not investigate the effects of ibuprofen for more than 48 hours in any subjects. Therefore, we should not disregard the possibility that the noted rebound phenomenon would have occurred despite continuation of drug administration, although this is considered unlikely. Hence, this might be an interesting target for future studies. If proven statistically significant, this phenomenon could result in a clinical recommendation that administration of ibuprofen should be continued throughout sojourn at altitude to prevent headache.
As expected, SpO2 decreased significantly in response to the hypobaric pressure at high altitude. This is in agreement with a large number of earlier studies, (O'Connor et al., 2004; Napoli et al., 2009; Wagner et al., 2012; Mandolesi et al., 2014). In this study, we found an association between AMS score and lower saturation, whereas other studies, at similar altitudes, did not (e.g., O'Connor et al., 2004). Our study had the advantage of multiple AMS and SpO2 measurements in the same subjects. We found relative protection of the brain's oxygenation during hypoxic exposure, with a mean decrease in brain saturation of only about 4%, whereas peripheral saturation decreased by over 13% (Table 4). We found no difference between blood or muscle oxygenation between the placebo and ibuprofen groups.
In contrast to our hypothesis, we did not observe a lower central or peripheral oxygenation in the ibuprofen group. The foundation for this hypothesis was that HVR was blunted by ibuprofen in rats (Popa et al., 2011) and humans (Basaran et al., 2016). Because the augmentation of HVR continues for a period of at least 12 days during acclimatization to altitude (Sato et al., 1994), it is possible that our study ended before an effect of augmented HVR on central or peripheral saturation would have been detectable. However, in line with our results on oxygenation, previous studies on ibuprofen show no effect on peripheral oxygenation (SpO2) of treatment with ibuprofen at altitude (Gertsch et al., 2012; Lipman et al., 2012), and even though ibuprofen blunted HVR in the study by Basaran et al. (2016), there was no significant difference on SpO2. This indicates that even though there is a blunting of HVR by ibuprofen at altitude, central and peripheral oxygenation may not be affected. We note that we did find a significant correlation between AMS scores and saturation and HR in analysis that pooled all subjects.
Limitations
It is possible that the ibuprofen dose may have been too low to change AMS scores or cytokine levels since previous studies have found a reduction in AMS scores with 600 mg doses of ibuprofen (Gertsch et al., 2012; Lipman et al., 2012). However, we studied the recommended package label ibuprofen dose to make our findings relevant to most travelers to high altitude. The matter of the efficacy of different doses of ibuprofen in reducing AMS symptoms will need to be resolved by a head to head trial. In addition, the same dose we studied was found to blunt the augmentation of HVR in humans (Basaran et al., 2016) and another of the primary objectives of this study was to determine the effect of ibuprofen on oxygenation. Even though we studied 20 subjects, a post hoc analysis shows that the study was underpowered for comparing AMS symptoms and physiological parameters at multiple time points. Given individual variation in responses to altitude, a crossover study design may have revealed differences in the effects of ibuprofen and placebo on altitude effects. The randomization procedure resulted in a preponderance of Caucasians in the ibuprofen group (Table 1). It is not clear what, if any, effect this had on the study outcome.
Correlation between AMS scores and cytokines were not corrected for multiple testing, so this should be considered preliminary, but may help guide further research.
Conclusions
Ascent to 3800 m was associated with increases in inflammatory cytokines in a population of healthy subjects with a high incidence of AMS. Ibuprofen, at 400 mg three-times a day dosing, did not have a significant effect on altitude-related increases in cytokines, peripheral or tissue oxygenation, or AMS.