
Abstract
Abstract
Orr, Jeremy E., Erica C. Heinrich, Matea Djokic, Dillon Gilbertson, Pamela N. Deyoung, Cecilia Anza-Ramirez, Francisco C. Villafuerte, Frank L. Powell, Atul Malhotra, and Tatum Simonson. Adaptive servoventilation as treatment for central sleep apnea due to high-altitude periodic breathing in nonacclimatized healthy individuals. High Alt Med Biol. 19:178–184, 2018.
Aims:
Central sleep apnea (CSA) is common at high altitude, leading to desaturation and sleep disruption. We hypothesized that noninvasive ventilation using adaptive servoventilation (ASV) would be effective at stabilizing CSA at altitude. Supplemental oxygen was evaluated for comparison.
Methods:
Healthy subjects were brought from sea level to 3800 m and underwent polysomnography on three consecutive nights. Subjects underwent each condition–No treatment, ASV, and supplemental oxygen–in random order. The primary outcome was the effect of ASV on oxygen desaturation index (ODI). Secondary outcomes included oxygen saturation, arousals, symptoms, and comparison to supplemental oxygen.
Results:
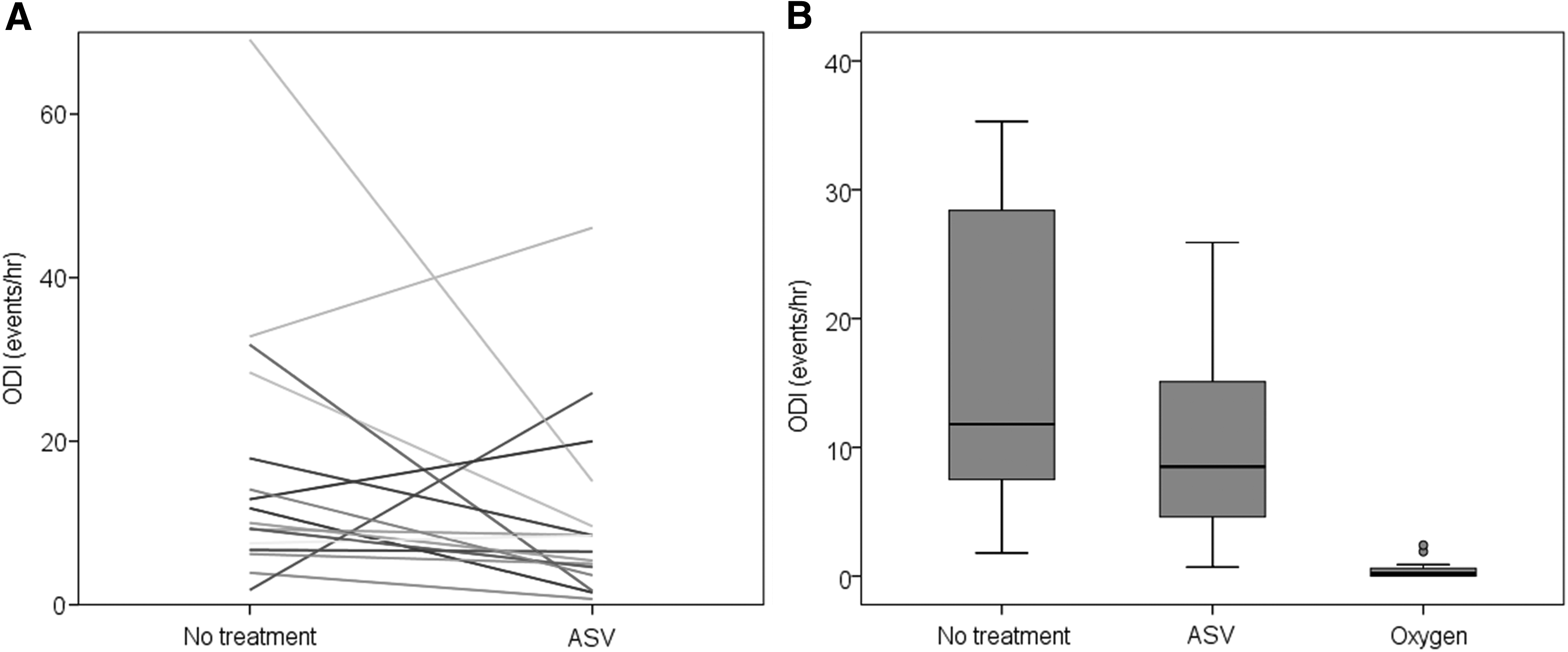
Eighteen subjects underwent at least two treatment conditions. There was a significant difference in ODI across the three treatments. There was no statistical difference in ODI between no treatment and ASV (17.1 ± 4.2 vs. 10.7 ± 2.9 events/hour; p > 0.17) and no difference in saturation or arousal index. Compared with no treatment, oxygen improved the ODI (16.5 ± 4.5 events/hour vs. 0.5 ± 0.2 events/hour; p < 0.003), in addition to saturation and arousal index.
Conclusions:
We found that ASV was not clearly efficacious at controlling CSA in persons traveling to 3800 m, whereas supplemental oxygen resolved CSA. Adjustment in the ASV algorithm may improve efficacy. ASV may have utility in acclimatized persons or at more modest altitudes.
Introduction
M
CSA-HAPB is characterized by unstable breathing; central apneas or hypopneas are followed by hyperventilation in a cyclical fashion with a cycle time of ∼30–45 seconds (Orr et al., 2017b). Generally, the mechanism underlying this respiratory pattern reflects conflicting dynamics between hypoxic stimulation of ventilation and suppression of respiratory output from ensuing hypocapnia (Lahiri et al., 1983). Arousal may contribute to and/or be a result of instability. The overall effect is high chemoreflex sensitivity and proximity to the apnea threshold. Ventilatory time constants and circulation time between lung and chemosensors result in phase offset, thereby producing a cyclical pattern of breathing.
Correction of hypoxemia or pharmacological suppression of ventilatory instability can improve CSA-HAPB. However, these therapies may have limitations, particularly as certain circumstances might preclude their use. For example, nocturnal supplemental oxygen use improves CSA-HAPB and sleep quality but might not be widely available, and use of sedatives might not be desirable. Furthermore, there is research interest in understanding the effect of hypoxemia during sleep–independently of sleep disturbance and desaturations–which would necessitate a therapy with the sole effect of stabilized breathing.
Adaptive servoventilation (ASV) is a noninvasive ventilation mode that aims to stabilize such respiratory cycling. ASV is highly efficacious in controlling central sleep apnea (CSA) accompanying congestive heart failure (Cheyne-Stokes respiration) and other etiologies (Carnevale et al., 2011; Sharma et al., 2012; Morgenthaler et al., 2014). The aim of this study was to determine whether ASV use during sleep can stabilize periodic breathing due to hypobaric hypoxemia at altitude. Some of the results of these studies have been previously reported in the form of an abstract (Orr et al., 2017a).
Methods
Subjects were recruited by word of mouth. Inclusion criteria were healthy individuals ages 18–65 years. Exclusion criteria were the presence of any known sleep disordered breathing, cardiopulmonary disease, chronic use of medications that might affect breathing (i.e., sedatives, narcotics, hypnotics) or acclimatization (i.e., anti-inflammatories, diuretics), a history of smoking, travel to high-altitude (>2500 m) within the preceding 3 months, and any previous instances of high altitude pulmonary or cerebral edema.
Before participating in the study, all subjects provided written informed consent. The study protocol was approved by the University of California San Diego Institutional Review Board. Subjects underwent baseline polysomnography before ascent, or at least 2 weeks after the sojourn, to confirm the absence of sleep disordered breathing (apnea-hypopnea index <10/hour).
During September and October 2016, subjects were transported in a single day from near sea level (San Diego, California) to the Nello Pace Laboratory at the White Mountain Research Center Barcroft Station, a high-altitude research station located at 3800 m elevation in Mono County, California. Subjects were asked to abstain from analgesics, alcohol, or other sedating medications during the study. Caffeine consumption was prohibited after 12:00 pm each day. During the day, subjects were permitted to participate in activities ad lib, including moderate exercise, but did not descend from altitude. Subjects were instructed to adhere to their normal sleep schedule.
Subjects were instrumented each night with a limited channel polysomnogram (Respironics Alice PDx, Murraysville, PA) consisting of nasal pressure (except during ASV use), finger pulse oximetry, thoracic and abdominal effort bands, snore sensor, electro-oculogram, two channel electroencephalogram, and chin electromyogram. In addition, each subject was fitted with a WatchPAT device, consisting of fingertip peripheral arterial tonometry and pulse oximetry (Itamar Medical, Caesarea, Israel). In the event of a failure from the AlicePDx device, the oximetry from the WatchPAT was used. Studies were scored by a Registered Polysomnographic Sleep Technologist using American Academy of Sleep Medicine criteria for scoring and Chicago Criteria for events.
Starting with the first night at altitude, the following conditions were performed for each individual in randomized order. (1) No treatment: Subjects slept with only polysomnography. (2) ASV: A ResMed S9 VPAP Adapt (ResMed, San Diego, CA) was set to expiratory positive airway pressure (EPAP) 4 cm and pressure support 3–10 cm water; settings were not adjusted during the night. Patients wore a nasal mask or pillows that was individually fitted before bed. (3) Supplemental oxygen: A NewLife AirSep oxygen concentrator (Chart Industries, Inc., Buffalo, NY) provided a flow of 2 L/min or higher if needed to maintain awake seated saturation >95% via a nasal cannula.
The primary outcome was a difference in the oxygen desaturation index (ODI) between ASV and no treatment. Secondary outcomes included (1) differences in ODI across the three treatment conditions, (2) differences in other polysomnographic parameters such as arousal index, sleep stages, and oxygen profiles, and (3) differences in sleep quality by the Stanford Sleep Questionnaire (Hoddes et al., 1973), and Lake Louise Acute Mountain Sickness (AMS) Score (Roach et al., 1993).
The potential confounding effect of acclimatization was analyzed by examining the change in ODI and other oxygen profiles, and arousal index and sleep quality over the three nights. In addition, morning awake oxygen saturation (SpO2) after each night was examined as a marker of acclimatization, a process that occurs within days to weeks at altitude. Total ventilation is augmented with acclimatization, with a resulting increase PaO2 and decrease in PaCO2 that leads to a rise in SpO2 (Ainslie et al., 2013).
Statistical analysis was performed in SPSS 24 (IBM Corp, Armonk, NY). Differences across those who completed all interventions were performed using generalized linear modeling with repeated measures ANOVA. Paired or between-group differences were performed using Student's t-test, with a Bonferroni correction for three pairwise comparisons corresponding to each variable of interest. Demographic data are reported as mean ± standard deviation, and comparisons are reported as mean ± SEM. A p-value of 0.05 was deemed statistically significant. As a pilot study, no formal power calculation was performed.
Results
Out of 20 subjects enrolled, two were excluded because they only completed the supplemental oxygen condition. The remaining 18 enrolled subjects completed at least two treatment conditions. The mean age was 29 ± 4 years, 12 men and 6 women, body mass index 24.4 ± 2.6 kg/m2, and baseline (near sea level) apnea-hypopnea index 2 ± 2/hour. Data were obtained from the no treatment condition on 17 subjects (1 missing sleep data), ASV condition on 17 subjects (1 missing sleep data), and supplemental oxygen condition on 16 subjects (2 with oxygen concentrator malfunction). All three conditions were completed by 14 subjects. All data were from the polysomnogram except four subject-nights from which WatchPAT oximetry data were incorporated. No adverse events were reported.
Oxygenation
Among the 14 subjects completing all treatment conditions, there was a significant difference in ODI across treatments (No treatment 15.2 ± 4.6/hour vs. ASV 8.3 ± 2.0/hour vs. oxygen 0.5 ± 0.2/hour; p < 0.004 for linear trend). There was also a significant difference in nadir saturation (No treatment 71 ± 2% vs. ASV 73 ± 1% vs. oxygen 92 ± 1%; p < 0.001) and mean saturation (No treatment 79 ± 1% vs. ASV 81 ± 1% vs. oxygen 96 ± 0%; p < 0.001). Pairwise comparisons between treatments are shown in Table 1. Individual data comparing ASV to no treatment, and data for all treatment conditions are shown in Figure 1.
Data shown as mean ± SEM.
Significant using Bonferroni correction for three comparisons.
ASV, adaptive servoventilation; ODI, oxygen desaturation index.
Sleep quality and symptoms
There was a significant difference in arousal index across treatments (No treatment 11.6 ± 1/hour vs. ASV 12.3 ± 1.7/hour vs. oxygen 7.9 ± 1.0/hour; p < 0.03). Pairwise comparisons between treatments are shown in Table 1.
There were significant differences in non-rapid eye movement (NREM) stage 1 sleep across treatments (No treatment 9.8 ± 1.1% vs. ASV 10.2 ± 1.6% vs. oxygen 6.2 ± 0.6%; p < 0.04) but no statistically significant differences were detected in percent NREM stage 2, stage 3, or rapid eye movement (REM) sleep.
There was no significant difference between no treatment, ASV, or supplemental oxygen on the AMS score recorded on the evening following treatment (2.4 ± 0.5 vs. 2.1 ± 0.3 vs. 1.4 ± 0.4; p > 0.25). There was also no significant difference between no treatment, ASV, or supplemental oxygen on the Stanford Sleepiness Scale (3.4 ± 0.4 vs. 3.2 ± 0.4 vs. 2.8 ± 0.5; p > 0.45).
Acclimatization
There was no significant overall change in ODI across the 3 nights in the 14 patients who completed all treatments (Night 1 12.9 ± 5.0/hour vs. Night 2 5.4 ± 1.7/hour vs. Night 3 5.6 ± 1.5/hour; p > 0.19). Similarly, there was no difference in nadir saturation (p > 0.89), mean saturation (p > 0.78), or arousal index (p > 0.08). Pairwise comparisons between nights of treatment are shown in Table 2. There was no significant change in awake morning SpO2 over 3 nights across all 18 subjects (89.3 ± 0.8% vs. 89.7 ± 1.0% vs. 90.3 ± 0.8%; p > 0.43).
Data shown as mean ± SEM.
Significant using Bonferroni correction for three comparisons.
There was no significant difference in mean ODI for subjects who received each specific treatment on night 1, 2, or 3 (no treatment: p > 0.81, ASV: p > 0.40, and oxygen: p > 0.36).
ASV compliance
Compliance data from the ASV device were available on 11 subjects. Mean use of 7:01 ± 1:53 hours, with two subjects using <4 hours and the remaining using >6 hours. There was an inverse correlation between hours use and ODI on the ASV night (Rho = −0.667; p = 0.050).
Discussion
The main result of this study is that we did not observe ASV to be consistently efficacious for controlling CSA-HAPB in nonacclimatized persons traveling to an altitude of 3800 m. In addition, we did not see improvement in other measures of oxygenation, sleep quality or symptoms other than a small improvement in mean nighttime saturation. In contrast, supplemental oxygen was effective at controlling periodic breathing with resulting improvement in arousals as well, a finding expected a priori but which has not been previously documented by electroencephalography.
The reason for the suboptimal performance of ASV is unclear, but there are several possible explanations. First, the ASV algorithm attempts to maintain constant breath-by-breath ventilation based on measures from the past several minutes. Hyperventilation related to discomfort, arousal, or anxiety–particularly in these ASV naïve subjects–can therefore lead the device to a high ventilation “target.” The patient's return to the lower true eupneic ventilation would then be opposed by the device, which would react by increasing pressure support. A possible example of this phenomenon is shown in Figure 2. Acclimation to wearing the device before use at altitude might improve this issue.
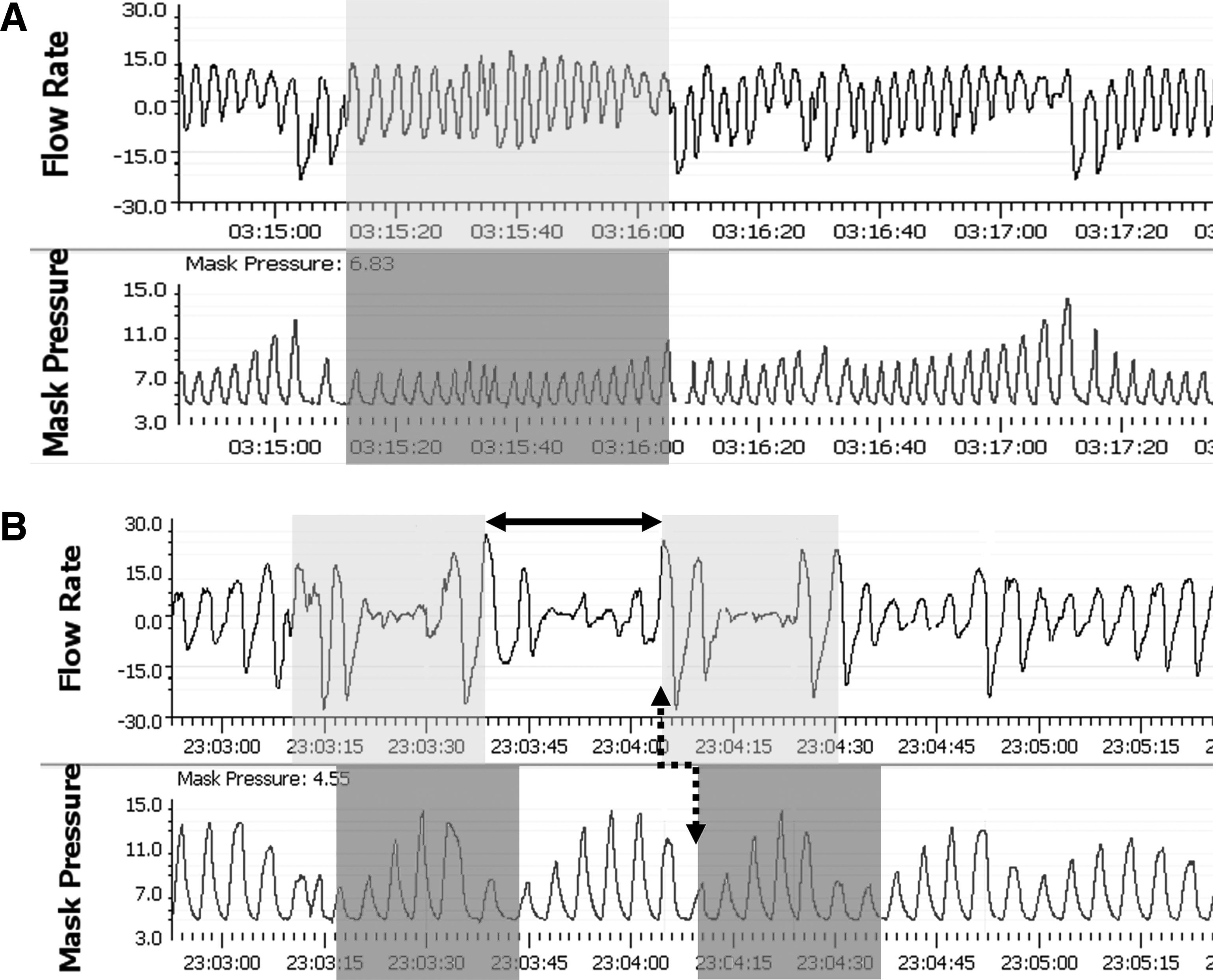
Examples of flow and mask pressure over time during sleep in ASV treated study subjects.
Second, the characteristics of respiratory control instability at altitude might also be important. Hypoxia-induced hyperventilation places CO2 levels near the apneic threshold. Since ASV provides further ventilation during periods of apnea or hypopnea to maintain stable breathing, mean ventilation may increase and therefore further decrease CO2 reserve (i.e., closer to apneic threshold). In theory, this process could result in a feed-forward mechanism, worsening instability. Although over time ASV appears to decrease the eupneic ventilation (Carnevale et al., 2011), such stabilizing effects may take time or not be observed in high altitude.
Another consideration is the short cycling time seen in high-altitude periodic breathing (as compared to systolic heart failure), which would require relatively rapid changes in pressure support to stabilize ventilation. An example from a subject is shown in Figure 2, in which the kinetics of the ASV response to hypoventilation results in increased pressure support when ventilation has already started rising. Such a phase offset can actually serve to further destabilize ventilation by driving hyperpneas (Orr et al., 2014). This particular issue may be amenable to improvement by adjusting the ASV algorithm, which is typically designed for longer time-scale fluctuations such as those seen in Cheyne-Stokes respirations (Hall et al., 1996). In principle, an ASV device could be adjusted according to circulation time, since the responsiveness required to stabilize breathing will likely differ depending on the etiology.
Finally, compliance was an issue among some subjects, and worsened usage might have decreased the efficacy. However, we cannot exclude the converse explanation that subjects in whom ASV was not effective at controlling periodic breathing were less likely to use the device.
We found a decrease in arousal index across the three nights, which may have important implications. Arousals may be a result of periodic breathing, but also can drive ventilatory instability by transiently increasing chemical drive to the higher levels seen during wakefulness and may also independently contribute to ventilation by a mechanism akin to a startle response, that is, state instability. Interestingly, we found no statistically significant improvement in periodic breathing over three nights, a finding consistent with other research demonstrating worsening, rather than improvement, of periodic breathing during acclimatization (Bloch et al., 2010; Andrews et al., 2012). Available data also suggest that periodic breathing persists when measured at sojourns lasting up to 1 year (Tellez et al., 2014).
In contrast, limited research and experience suggest that sleep quality does improve over time at altitude despite persistence of periodic breathing (Reite et al., 1975; White et al., 1987; Nussbaumer-Ochsner et al., 2012). Although mechanisms are unknown, this improvement may relate to time-dependent changes in the control of breathing during acclimatization (Pamenter and Powell, 2016), and plasticity of the threshold to arousal over time. If the contribution of arousal to CSA decreases over time, we suspect the efficacy of ASV may be substantially higher.
Other treatments for CSA at altitude have been examined, including oxygen and other therapies. Supplemental oxygen has been shown in the past to improve sleep apnea at altitude, both in nonacclimatized persons and long-term dwellers (Luks et al., 1998; Moraga et al., 2014). Our study adds to this data with the use of electroencephalographic assessments of sleep, which to our knowledge have not been previously reported.
Although in many ways supplemental oxygen is an ideal treatment, a few caveats are worth mentioning. First, oxygen concentrators are not always available or practical. An example is when power availability is limited; a concentrator typically consumes 150–300 watts whereas PAP devices use 20–50 watts. Second, higher FiO2 levels are needed to normalize PaO2 levels in hypobaric conditions. Local irritation can occur if delivered nasally, and over-supplementation, even at modest levels, might have important systemic effects. Finally, supplemental oxygen might delay acclimatization by reducing exposure to hypoxemia. A single night study has not found effects on hypoxic or hypercapnic ventilatory responses, but longer periods of study might be needed to appreciate an effect (McElroy et al., 2000).
Device treatments include “dead space” masks and bilevel ventilation with a backup rate, which have both been shown to improve periodic breathing at altitude (Johnson et al., 2010; Patz et al., 2013). The addition of deadspace has potential to worsen hypoxemia and requires “titration” to be effective without causing arousals. The success of bilevel ventilation, which in theory is less physiologic for treating ventilatory instability, suggests that with further adjustment ASV might be effective. Pharmacologic therapies such as acetazolamide and temazepam have been shown to be generally effective but may not be appropriate for all individuals and circumstances, or for long-term use (Nickol et al., 2006; Liu et al., 2017).
Further research in this area is warranted. As discussed above, adjustment of the ASV algorithm might render this treatment more efficacious. ASV might be more effective in acclimatized individuals or high-altitude dwellers, in whom persistent sleep apnea might have adverse consequences (Pham et al., 2017). From a research standpoint, the ability to separate the effects of sustained hypoxemia during sleep from intermittent desaturations and arousals is of interest for neurocognitive and metabolic studies. For example, reports of impaired cognitive function at high altitude may result from hypoxemia during testing and/or poor sleep quality on nights before testing.
Finally, recent data suggest that for those with obstructive sleep apnea, central apneas while on continuous positive airway pressure increase with higher altitude and appear to impact compliance (Pandey). The ideal treatment in this circumstance is unclear and management appears to vary (Latshang et al., 2012); however, our research indicates that the effectiveness of ASV for these patients is not a foregone conclusion.
Our study clearly had important limitations. Because of the labor-intensive nature of these studies, we had limited sample size. We had smaller than expected response to ASV, diminishing the power of the study. While a larger study might have shown statistical significance, such a modest effect of ASV is not likely to be clinically meaningful. Addressing the issues with ASV observed in this study would be more worthwhile. Polysomnography was unattended due to facility and technician constraints; titration of settings might have improved ASV efficacy. Similarly, EPAP was set to a fixed pressure, rather than tech- or software-titrated, although upper airway obstruction was not observed during no treatment conditions. Finally, the study design exposed subjects to acclimatization as a potential contributing variable to the outcomes of interest, which decreased our statistical power; however, we did not observe any substantial effect of acclimatization, so it is doubtful that this issue contributed to any type II error.
Conclusion
We did not observe consistent efficacy in the use of ASV for treatment of CSA due to high-altitude periodic breathing in nonacclimatized individuals ascending to 3800 m. In contrast, oxygen was highly efficacious during sleep verified by polysomnography with electroencephalography. Further research incorporating adjustment the ASV device algorithm toward high-altitude periodic breathing kinetics, and investigation of potential utility of ASV in other modest to high altitude scenarios is warranted.
Footnotes
Acknowledgments
The authors would like to thank the staff of the University of California White Mountain Research Center for facilitating these experiments.
Compliance with Ethical Standards
Author Disclosure Statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this article.