
Abstract
Abstract
Muratali Uulu, Kubatbek, Meerim Cholponbaeva, Melis Duishobaev, Aidana Toktosunova, Abdirashit Maripov, Akylbek Sydykov, and Akpay Sarybaev. A case of subacute infantile mountain sickness in a Kyrgyz child. High Alt Med Biol. 19:208–210, 2018.—Subacute infantile mountain sickness (SIMS) is a syndrome of severe pulmonary hypertension and right heart failure that develops in infants born in the lowlands and subsequently brought to live at high altitudes. Earlier postmortem studies have demonstrated significant remodeling of small pulmonary arteries as well as right ventricular hypertrophy and dilatation. In this report, we present a case of SIMS in a Kyrgyz child born to a native highlander mother evaluated by conventional echocardiography and tissue Doppler imaging. An echocardiogram showed severe pulmonary hypertension, a markedly dilated right ventricle with flattening of interventricular septum, and right ventricular dysfunction. To our knowledge, this is the first report of noninvasive imaging of pulmonary circulation and right ventricle in an infant with SIMS and confirmed the diagnosis using echocardiography.
Introduction
B
Right heart catheterization studies performed at moderate altitudes demonstrated sustained pulmonary hypertension in these patients (Wu and Miao, 2002). Postmortem pathological investigations showed significant remodeling of small pulmonary arteries as well as hypertrophy and dilation of the right ventricle (Sui et al., 1988; Heath et al., 1989). However, no imaging studies of the pulmonary circulation and the right ventricle in infants with SIMS have been reported so far. Therefore, we sought to present a case of SIMS in a Kyrgyz child born to a native highlander mother evaluated by conventional echocardiography and tissue Doppler imaging.
Case Report
A 1-year-old female infant was admitted to a local hospital located at 3000 m (Sary-Mogol, Kyrgyzstan) with complaints of dry cough and breathlessness. The infant's native highlander mother moved to the village located at 1540 m (Gulcho, Kyrgyzstan) after marriage where she gave birth to her daughter. When the baby became 4 months old, the mother entered university in Osh (Kyrgyzstan). Therefore, the infant was brought to her grandparents residing at 4200 m (Karakol, Tajikistan). At high altitude, the baby gradually developed dyspnea and dry cough. Therefore, after spending 7 months in Karakol, the grandparents brought the girl to Sary-Mogol located at lower altitude. As the symptoms did not improve after 1 month at lower altitude, the girl was brought to the local hospital.
Clinical assessment revealed cyanosis, accentuation of the P2 heart sound, tachycardia (150 bpm), and SpO2 (84%). Transthoracic echocardiography showed dilated right-sided chambers with bowing of the interventricular septum into the left ventricle (Fig. 1A). Right ventricular chamber dimensions including the basal and the mid-cavity diameters and the distance from the tricuspid valve annulus to the right ventricular (RV) apex in the apical four-chamber view at end diastole were measured as 3.48, 2.91, and 5.19 cm, respectively. The RV outflow tract at the proximal and at the distal level in the basal parasternal short-axis view was measured as 2.45 and 2.18 cm, respectively (Fig. 1B). There was significant tricuspid regurgitation with a maximal pressure gradient between the right ventricle and right atrium of 102 mmHg (Fig. 1C, D). The pulmonary artery was dilated with a diameter of 2.5 cm (Fig. 1E). The pulmonary flow pattern showed a midsystolic notching pattern with an acceleration time of 61 ms (Fig. 1F). A right ventricular systolic function was impaired with RV fractional area change of 18.8%, tricuspid annular plane systolic excursion of 1.22 cm, and peak systolic velocity at the lateral tricuspid annulus of 10.1 cm/s (Fig. 1G, H). The ratio of early tricuspid inflow to annular diastolic velocity E/Ea, as a noninvasive estimation of RV filling pressure, was increased to 5.1. The ratio of tricuspid peak early filling (E wave) and late diastolic filling (A wave) velocities was measured as 0.75 (Fig. 1I). The patient was found to have SIMS and prompt relocation to low altitude was recommended.
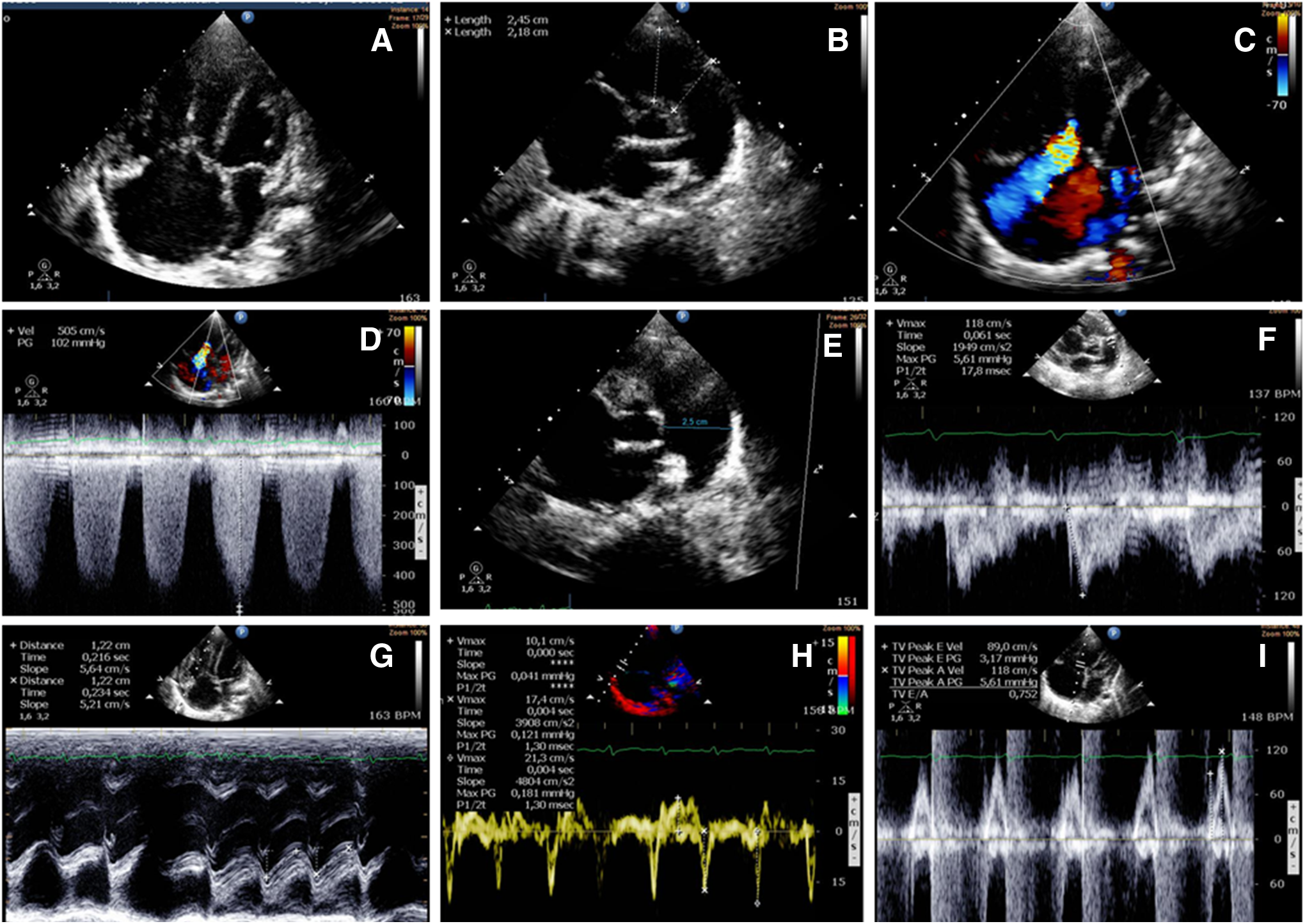
Echocardiogram in a child with subacute infantile mountain sickness.
Discussion
In this report, we present, for the first time, a case of a Kyrgyz infant with SIMS who was born at moderate altitude and developed severe pulmonary hypertension during residence at high altitude. In this patient, we evaluated the pulmonary circulation and the right ventricle by conventional echocardiography and tissue Doppler imaging. The echocardiogram showed severe pulmonary hypertension, a markedly dilated right ventricle with flattening of interventricular septum, and right ventricular dysfunction. To our knowledge, this is the first report of noninvasive imaging of the pulmonary circulation and the right ventricle in an infant with SIMS using echocardiography.
SIMS has been described in lowland infants of Han origin who were born or brought to live at altitudes >3000 m (Sui et al., 1988). However, this condition can also develop in infants born to native Tibetans, who migrated from an intermediate altitude to a much higher altitude (Wu and Miao, 2002). Interestingly, no further cases of SIMS have been reported since the first publications describing this condition. This may be due to the fact that Han mothers nowadays descend to lowland regions to give birth and do not bring their children to high altitude until they have reached >1 year of age (Wu and Miao, 2002). However, as this case illustrates, SIMS might be still a public health concern in other parts of the world. Implementation of clinical screening programs followed by echocardiography in high-altitude areas would help reveal patients with severe pulmonary hypertension. Given the important role of hypoxia in the pathogenesis of hypoxic pulmonary hypertension, relocating the place of residence to lower altitudes would cure the disease (Grover et al., 1966; Sime et al., 1971).
Footnotes
Acknowledgment
This work was supported by the Ministry of Education and Science of the Kyrgyz Republic (No. 0005823).
Author Disclosure Statement
No competing financial interests exist.