
Abstract

To the Editor
A
Indeed, acute exercise and brief exposure to inspiratory hypoxia have been shown to compound systemic free radical formation (Bailey et al., 2017) and corresponding activation of coagulation in healthy lowlanders although as indicated by a shortening of activated partial thromboplastin time (aPTT) during acute (i.e., nonacclimatized) exposure to normobaric hypoxia (12% O2) equivalent to a simulated altitude of ∼4500 m. Although clearly a less marked (hypoxic) stimulus to that encountered at terrestrial extremes of high altitude (HA) and notwithstanding the interpretive limitations associated with aPTT including inherent sensitivity to psychological stress, these findings nonetheless suggest that hemostasis may potentially be subject to redox regulation (Fall et al., 2015).
Despite this, an impressive 4000 people (and counting) have conquered the “summit of the gods,” Mt. Everest, since the first ascent by Sir Edmund Hilary and Sherpa Tenzing Norgay in 1953. This can be accredited, in part, to developments in equipment and modern weather forecasting, making these death-defying summit bids more accessible to increasingly diverse groups, including those having suffered post-traumatic lower limb amputation (TLLA). Indeed, May 15, 2006, marked the first ascent of Mt. Everest by a double amputee.
However, despite this extraordinary physiological feat, emerging evidence tentatively suggests that those with TLLA may potentially run an even greater risk of thrombotic complications during ascent to HA subsequent to (enhanced) free radical-mediated activated coagulation. The combined stress of psychological trauma, abnormalities of arterial flow proximal to the amputation site (shear stress, circumferential strain, and reflected waves), and increased autonomic activity has been collectively associated with a systemic elevation in free radicals, shorter activated aPTTs, lower antithrombin III, and higher fibrinopeptide A (FPA), implying increased (redox-regulated) coagulability that in the long term has been associated with atherothrombosis and increased morbidity/mortality rates to cardiovascular disease (CVD) (Modan et al., 1998). Furthermore, the elevated factor VII plasma concentrations reported among amputees in this study also imply a potential role for mechanical deformation/damage to the vessels and surrounding vasculature at the interface of the tissue and artificial limb that could either precede or at the very least contribute to peroxidation.
However, further research is encouraged to confirm these findings, given the minimal differences in aPTT and abnormally elevated concentrations of FPA reported in this study that likely reflect technical artifacts associated with inadequate quality control during sampling (e.g., poor venepuncture technique, use of ethylenediaminetetraacetic acid, and postsampling cooling). Although collectively these data do not make a strong case for activation of blood coagulation being an important risk factor for CVD in amputees, it is nonetheless conceivable that this already “primed” molecular cascade is likely to be further compounded by the unavoidable combination of hypoxia, exercise, and cold during physical ascent to terrestrial HA, potentially increasing the risk of an adverse (thrombotic) event as outlined in Figure 1.
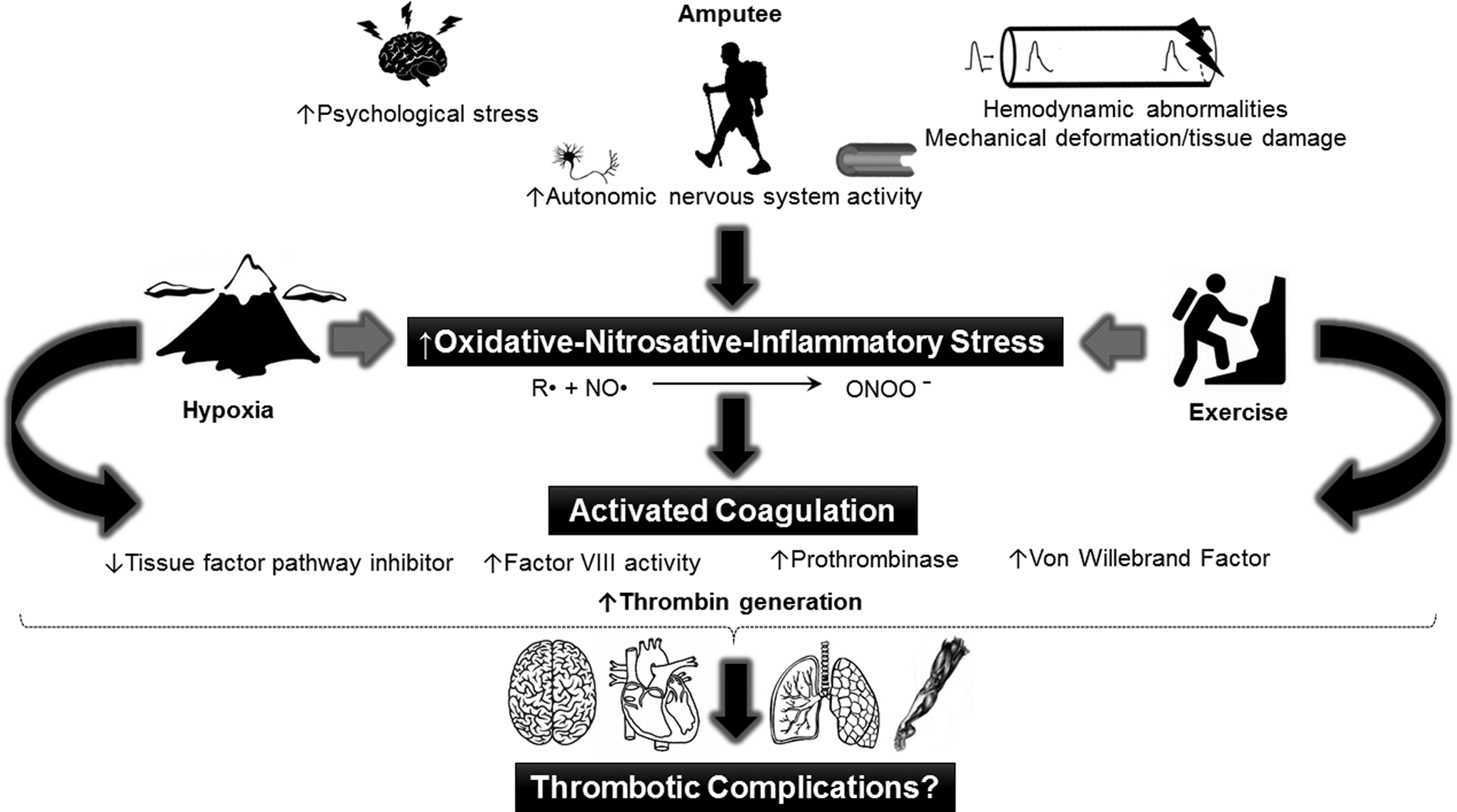
The “ascending amputee” and redox-regulated link to activated coagulation; cause for concern? The reaction schema defined by R• (free radical) + NO• (nitric oxide) → ONOO− (peroxynitrite) highlights the oxidative depletion of vascular NO bioavailability that could negatively impact vascular endothelial function to further compound thrombotic complications.
Surprisingly, there is a dearth of literature in this area and given the methodological limitations underpinning the assessment of coagulation to date, the combined application of novel analytical techniques including electron paramagnetic resonance spectroscopy for the direct detection and molecular characterization of free radicals, free oscillation rheometry for hemostasis, and imaging modalities that can assess mechanical deformation/damage at the interface of the tissue and artificial limb is encouraged to address this question and ultimately provide more informed mechanistic insight into a group of individuals who are likely to benefit from targeted pharmacoprophylaxis in the form of anticoagulation and/or antioxidant therapy. With regard to the latter, the weight of evidence supporting the benefits of antioxidant prophylaxis (although in the setting of CVD) is not overwhelming although there is considerable evidence linking oxidative stress to its pathophysiology (and indeed, physiology). Given the Janus Face of free radicals and associated ROS, notwithstanding the limitations/constraints imposed by diverse antioxidant compounds, dosage regimens, pharmacokinetic–pharmacodynamic properties, and genotypes, it is overly simplistic to assume that any “blanket” antioxidant strategy will likely be of benefit and the premise that one can “selectively” scavenge “pathological” versus “physiological” species with specific antioxidants is ultimately flawed. Clearly, further research is warranted to address our potential concerns in this defined clinical population.
Footnotes
Acknowledgments
D.M.B. is supported by a Royal Society Wolfson Research Fellowship (No. WM170007) and PhD studentship grant (for B.S.S.) from the Higher Education Funding Council for Wales.
Author Disclosure Statement
No competing financial interests exist.