
Abstract
Abstract
Nabrdalik, Katarzyna, Hanna Kwiendacz, Monika Gubała, Kinga Tyrała, Mariusz Seweryn, Andrzej Tomasik, Tomasz Sawczyn, Michał Kukla, Władysław Grzeszczak, and Janusz Gumprecht. Diabetes-related knowledge of Polish national mountain leaders. High Alt Med Biol. 19:237–243, 2018.—Mountain trekking is a popular activity for patients with diabetes. In Poland, mountain leaders often accompany organized groups to ensure their safety during treks; we aimed to evaluate their competency in caring for diabetic clients by assessing their diabetes-related knowledge. This was a cross-sectional study among Polish, certified, active mountain leaders carried out by means of an anonymous, standardized 41-item questionnaire adapted from a study by Wee et al. It was distributed through e-mail to 500 leaders. A total of 106 (21.2%) mountain leaders completed the questionnaire (males 60.4%) with a mean (standard deviation [SD]) age of 38.6 (13.5) years. Their mean (SD) length of experience acting as a mountain leader was 11.9 (10.2) years. The average score was 72.4% of the maximum possible (29.7 of 41 points). Results varied significantly depending on gender (p = 0.006). The percentage of correct answers among questions in each section varied between 23.6% and 100%. The main sources of diabetes-related knowledge identified by respondents were members of their family and their friends who suffer from diabetes (33%). First aid courses were indicated as sources of information by only 12.6% of the informants. Results of the questionnaire revealed that respondents did have a reasonable level of diabetes-related knowledge. There were topics in which the respondents achieved lower than an average score, demonstrating a need for further education.
Introduction
A
Few articles in medical literature describe the subject of mountain trekking undertaken by people affected by diabetes. To date, at least four patients with type 1 diabetes have managed to climb the world's highest summit—Mount Everest (8848 m) above sea level (Milewski, 2006). Recently, Gawrecki et al. reported that a group of 18 Polish patients with type 1 diabetes, treated with personal insulin pumps, successfully reached the summit of Mount Damāvand (5670 m). The altitude, where the trekking took place, did not have any serious negative effect on the course of diabetes. None of the participants experienced either severe hypoglycemia or metabolic decompensation (Gawrecki et al., 2016).
Similarly, in 2012, a group of 13 type 2 diabetic patients successfully climbed Mount Toubkal (4167 m) after 6 months of exercise training, which had a positive influence on their blood lipid profile, glucose, and fasting insulin concentration with no deterioration in glycemic control (De Mol et al., 2012). There are also reports on successful expeditions to Mount Kilimanjaro in Tanzania (Moore et al., 2001; Kalson et al., 2007), Cho Oyu in Tibet (Pavan et al., 2003), and Aconcagua in Argentina (Admetlla et al., 2001).
Despite the benefits of mountain trekking for diabetic patients, other hikers and mountain leaders participating in climbs with diabetics should be informed of their cohikers' condition and should possess some basic knowledge to deal with acute complications of diabetes, which may occur during the trip (Hillebrandt, 2003; Przybyłowski and Zieliński, 2004).
Diabetic patients should not be discouraged from taking part in mountain trekking as long as they can manage their blood glucose measurement, insulin, or insulin mimetic drug dose adjustment and undertake only a level of physical effort that is appropriate for them. For deeper insight into safety-related issues of mountaineering among patients with diabetes, comprehensive summaries can be found in review articles (Berghold and Lässer, 1988; Brubaker, 2005; Richards and Hillebrandt, 2013; de Mol et al., 2014; Mohajeri et al., 2015).
Hypoglycemia is potentially a major problem for diabetic patients on maintenance insulin therapy (Gumprecht and Nabrdalik, 2016) and appears to be one of the main causes of alpine accidents, especially among elderly trekkers (Malabu 2014). The available studies investigating first aid knowledge and emergency procedures among mountaineers do not explore this issue (Kimura et al., 2012). Apart from hypoglycemia, which seems to be the most frequent acute complication of diabetes during physical activity, there are other crucial health issues affecting diabetic patients, which mountain guides should be aware of, such as higher risk of sudden cardiovascular events and sudden death (Burtscher 2007).
The mountains in Poland have an altitude of over 1.000 m and rise to just over 2500 m. Mountain leaders accompany organized groups on climbs to ensure their safety on the trail and provide first aid when needed. Until 2012, Polish law required a guide during any mountain climb. The law has been partially abolished, but it still prevails in selected National Parks and on school trips.
While the range of theoretical courses for mountain guides includes topics such as tourist health, physical conditioning, and contraindications to mountain hiking, practical first aid training addresses the basic rules of tending to injured climbers and offers subjects concerning acclimatization and symptoms, prevention, and treatment of acute mountain sickness (AMS) (Journal of Polish Laws, 2014). The first aid course does not address hypoglycemia or diabetes. Therefore, in light of the rising prevalence of diabetes, it was crucial to assess diabetes-related knowledge among mountain leaders and to implement appropriate courses if needed.
This study was undertaken in Poland; however, its focus appears to be an issue of international importance, and the need for medical education among British mountain guides has already been studied (Hillebrandt, 2000). In this questionnaire-based study, members of the Association of British Mountain Guides were asked to identify five medical issues they had encountered as well as five medical educational needs. The study proved that mountain guides are well trained in trauma management, but require additional knowledge on practical aspects of travel medicine. Diabetes and asthma were identified as chronic conditions where additional education was needed.
While complications of diabetes may present during trail hiking, the level of risk can vary depending on the hiker's type of diabetes. Predominantly, not only in diabetes mellitus type 1 but also in patients with diabetes type 2 treated with insulin or insulin mimetic drugs, attention should be paid to the high number of potential complications of diabetes that can lead to potentially serious consequences. These include hypoglycemia, the possible malfunction of an insulin pump (which can put a patient at risk of hyperglycemia) or a glucometer, and freezing of insulin at low temperatures.
In the case of type 2 diabetes, some medications and their side effects pose significant risks. Patients treated with oral drugs that stimulate the secretion of insulin can suffer from hypoglycemia, while treatment with SGLT-2 inhibitors can lead to dehydration, especially if taken with diuretics and at high temperatures. To prevent hypoglycemia during intense physical activity, a diabetic person should remember to reduce the dose of prandial insulin and basal insulin and be aware of the need to consume high-carbohydrate snacks.
If climbing at higher altitudes, where acclimatization is needed, a diabetic may need to take additional precautions, which would be unnecessary for a healthy person. Vomiting, a symptom of AMS, and usage of acetazolamide, which is helpful in preventing AMS, can lead to ketoacidosis. This is one of the most serious potentially fatal complications of diabetes. Therefore, actions to prevent AMS, most importantly gradual acclimatization, are crucial. Since severe hypoglycemia can be confused with AMS, it is important for guides to be familiar with both diseases (Moore et al., 2001). Considering all the above information, the aim of this study was to evaluate diabetes-related knowledge among Polish mountain leaders.
Materials and Methods
This was a cross-sectional study based on an anonymous survey questionnaire. A total of 500 Polish mountain leaders were invited through e-mail to participate in this study. Data collection was conducted in January 2016. Each respondent received a web link to fill out a questionnaire through https://docs.google.com Along with a questionnaire, mountain leaders received an informed consent to participate in the study. All those who responded to the inquiry sent back the signed informed consent through regular mail. The study was anonymous and voluntary. To be included in the study, participants had to be Polish mountain leaders of at least 18 years of age and needed to have at least a high school diploma. Demographic information and length of work experience were collected from the participants.
The standardized questionnaire was adapted from the study by Wee et al. (2002) (Table 1). To the best of our knowledge, there is no validated questionnaire assessing diabetes-related knowledge among mountain leaders. The questionnaire we chose is the only validated one used in a population of people without diabetes. The questionnaire adapted from the study by Wee et al. originally aimed to determine diabetes-related knowledge of members of the public in Singapore.
Adapted from a study by Wee et al.
It is a 41-item questionnaire divided into 5 main sections, including general knowledge about diabetes (8 questions); risk factors (4 questions); signs and symptoms (12 questions); control and treatment (13 questions); and diabetes monitoring (4 questions). The answer to each question was confined to the options of yes, no, or unsure. One point was given for a correct answer, 0 points for either an incorrect or no answer. The maximum possible score was 41 points.
The survey was translated into Polish by two independent translators, fluent in both languages, and checked by two specialists from the diabetes field. The original question “How many types of diabetes are there?” was changed to “Is there more than one type of diabetes?” since the original question was an open one. Additionally, respondents were asked how often and on which mountains they had guided groups. We also wanted them to state the main source of their diabetes-related knowledge.
Statistical analysis was performed using Statsoft Statistica, v12, software. In the case of quantitative variables, normality of distribution was tested by the Shapiro–Wilk test. Distribution of quantitative variables was evaluated based on the average and standard deviation (SD), while distribution of categorical variables was presented in percentage terms. Depending on the number of cases and normal distribution, the Mann–Whitney U-test or Student's t-test was used for statistical analysis of quantitative variables. The chi-square and Fisher tests were used for statistical analysis of categorical variables. The statistical significance level was set at p < 0.05.
Results
Of 500 mountain leaders, 106 (21.2%) with a mean (SD) age of 38.6 (13.5) years (60.4% male) responded to the invitation to complete the questionnaire. The minimum age of respondents was 21 and the maximum 70 years. The largest group of respondents (29.2%) was in the age range of 31–40 years and a minority of them were over 60 years of age (12.3%). Eighty-four percent of respondents held a university-level diploma. The mean (SD) length of experience as a mountain leader was 11.9 (10.2) years. The guides came from every part of Poland and their guide certifications covered the entire area of mountain ranges in Poland (the Beskidy, Sudety, and Tatra Mountains). Nine of the mountain leaders were members of the Union of International Mountain Leader Associations (UIMLA).
In terms of frequency of group guiding over a span of 12 months, the most frequent response was several times a year (36.8% of mountain leaders). It was reported by 81% of respondents that they always asked group members about chronic medical conditions before departure.
Regarding the main source of diabetes-related knowledge, 33% of respondents declared that it had been acquired from members of their family and friends who suffered from diabetes (Fig. 1).
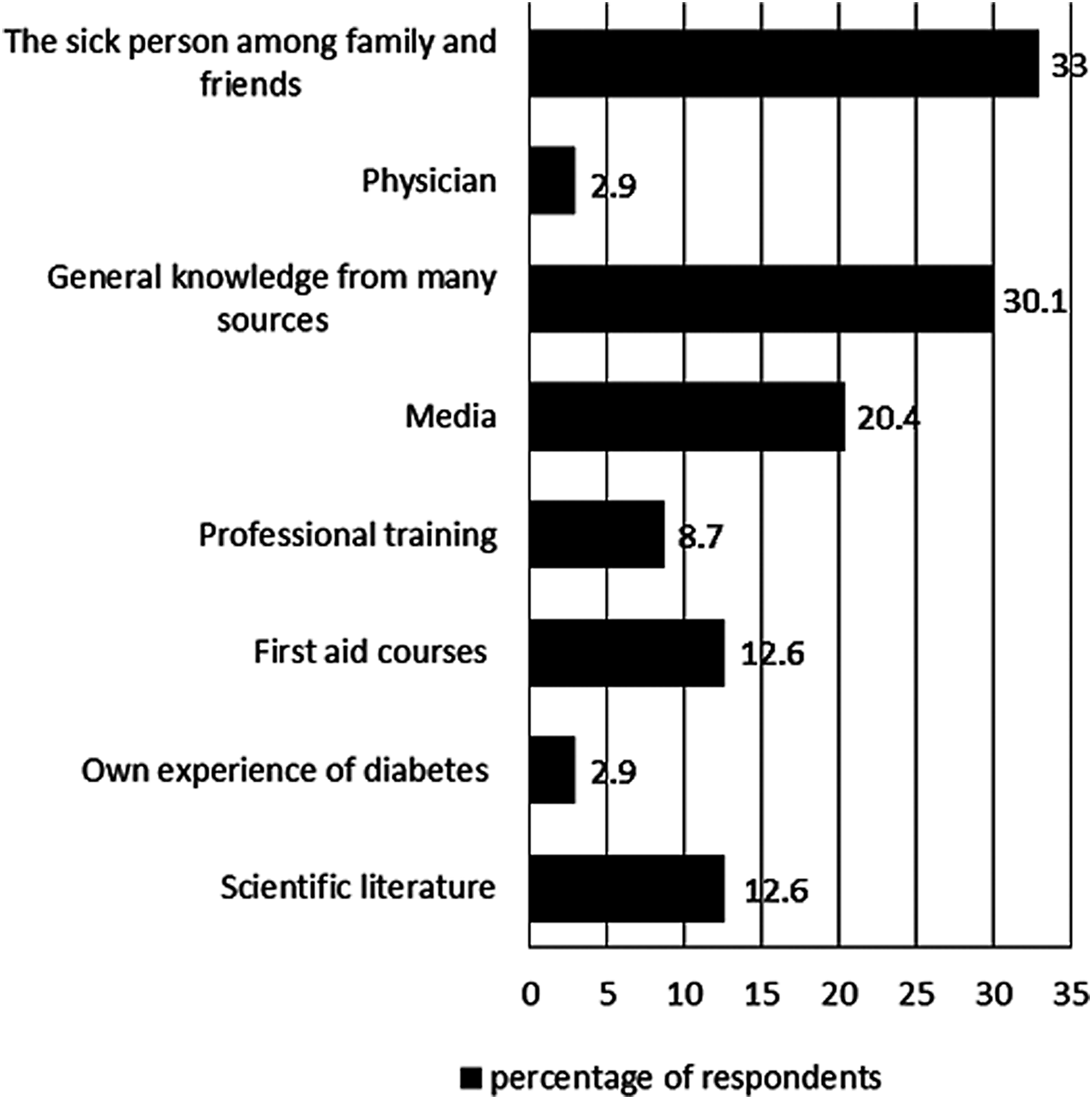
Sources of diabetes-related knowledge indicated by mountain guides.
The average score obtained from the questionnaire was 72.4% of the maximum possible score (29.7 of 41 points). The lowest score was 17% and the highest was 100% (Fig. 2). Scores were grouped into classes: very good: 41–31 points; good: 30–21; poor: 20–11; and very poor: under 11. Almost half of the respondents (46.2%) achieved a very good score (41–31 points) in the questionnaire.
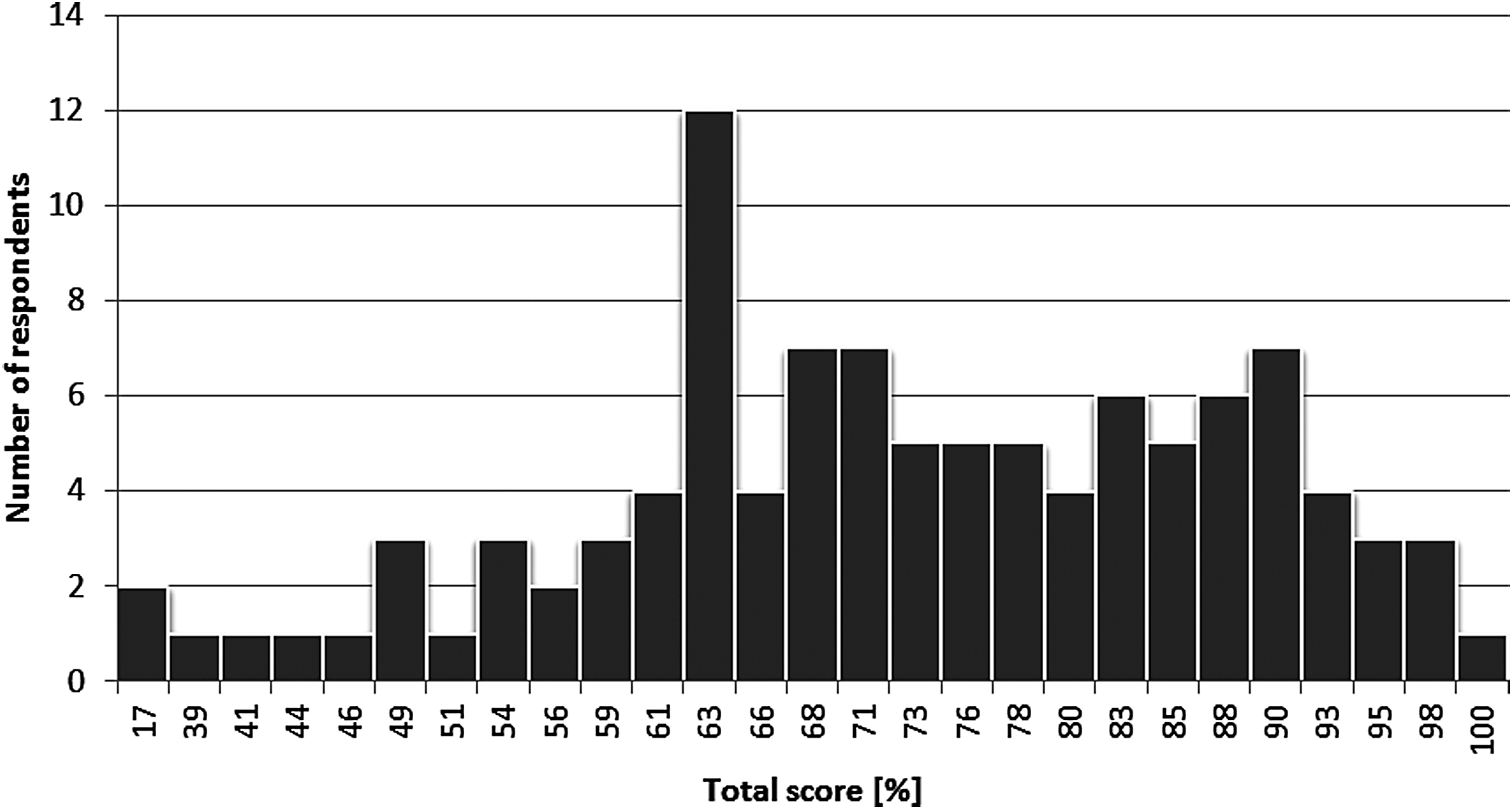
Distribution of questionnaire total score.
The mean percentages of correct answers in particular sections of the questionnaire were as follows: 74%—general knowledge, 71%—risk factors, 62%—symptoms and complications, 69%—treatment, and 85%—monitoring.
Results varied significantly depending on the respondent's gender (p = 0.006). The mean (SD) score for women was 31.9 (6.0) points and the mean (SD) score for men was 28.3 (6.6) points. Among women, 61.9% achieved a very good score and 30.9% achieved a good score. Among men, the figures were 35.9% and 54.6%, respectively. There was no significant difference between the average score of the questionnaire and age, type of education obtained, frequency of group guiding over a year, or mountain leader experience.
Discussion
Due to the high prevalence of diabetes worldwide and the risk of hypoglycemia during physical activity, the general public and especially people accompanying diabetic patients during physical activities should be appropriately educated so that they can administer first aid if needed. Mountain leaders should have basic diabetes-related knowledge and should know how to respond in cases of a diabetic emergency. We have shown that diabetes-related knowledge among the studied mountain leaders was adequate, even though it was not obtained from professional training.
To our knowledge, this was the first study performed to date assessing diabetes-related knowledge of mountain leaders of any nationality, although general diabetes-related knowledge has previously been evaluated in various countries and among different occupations (Wee et al., 2002; Rubin et al., 2007; Khan et al., 2012; Abdoli and Tavana, 2013). It is difficult to compare the results obtained from our study with previous studies as the study populations and questionnaires varied. We have briefly summarized the results and comparison to provide broad insights into the study topic.
Wee et al., who originally designed the questionnaire used in our study, evaluated general diabetes-related knowledge among 1337 people in Singapore, revealing sufficient knowledge about diabetes among respondents. Similar to our study, knowledge about monitoring of blood glucose was the strongest, with slightly better average scores from the Polish group (85% vs. 83.3%) Wee et al., 2002.
Abdoli and Tavana designed a descriptive study in Iran exploring diabetes-related knowledge in a group of 400 adults from the general population, who were older than 20 years, living in Isfahan, and who manifested normal glucose tolerance. The average score obtained from this questionnaire was comparable with that of the Polish mountain leaders. Moreover, it turned out that (similar to our study) the best scores were achieved by female participants. Contrary to our results, there were no significant differences between age and diabetes-related knowledge. The lowest score among the Iranian population was from respondents younger than 27 years (Abdoli and Tavana, 2013).
Khan et al. designed a study in United Arab Emirates to assess diabetes-related knowledge of 168 students on nonhealthcare-related professional courses. In accordance with our findings, the highest scores were achieved by females (Khan et al., 2012).
In the study performed by Wee et al. and Khan et al. and in our study, female participants obtained better scores than their male colleagues; however, the reason for this remains unclear. Comparing the results, one must take into consideration that respondents in the three previously mentioned studies were members of the general public who did not share any particular occupation, while mountain leaders are expected to be more qualified in medical emergencies and therefore their diabetes-related knowledge should be better.
Even among health professionals, this knowledge is not always adequate, which was shown by Rubin et al. using a questionnaire exploring diabetes-related knowledge among 48 nurses, 42 residents in surgery, 52 internal medicine residents, and 21 family practice residents in the United States. The mean score of all the respondents was 61%, indicating that healthcare professionals from medical specialties other than diabetology lack important knowledge of diabetes. Against this background, knowledge about diabetes of the Polish mountain leaders seems to be adequate (Rubin et al., 2007).
In addition to knowledge related to diabetes, its treatment, and potential health complications, a mountain leader should also be aware that a person with diabetes monitors blood glucose levels using a blood glucose meter (BGM). In our study, knowledge in this area was good with respondents answering questions on this topic, with accuracy between 73% and 98%. However, even though the questionnaire did not cover the accuracy of glucometer measurements, mountain leaders should realize that a glucometer may not work accurately at high altitudes. This is important since not all patients are aware of this fact.
Several studies have assessed the accuracy of different BGMs at high altitudes (Gautier et al., 1996; Fink et al., 2002; Bilen et al., 2007; De Mol et al., 2010; Olateju et al., 2012), but results regarding a preference to use BGMs based on glucose oxidase or glucose dehydrogenase were inconclusive. In conclusion, some authors state that the measurements can be under- or overestimated and therefore continuous insulin dose adjustment is crucial (Richards and Hillebrandt, 2013).
Most recently, the functioning of modern technologies has been tested in practice by the previously mentioned, and described by Gawrecki et al. (2016), group of Polish patients with type 1 diabetes during an expedition above 5000 m. After the expedition, authors concluded that the devices used during the trek seemed to work accurately even though the altitude was higher than that recommended (Matejko et al., 2017). Moreover, the participants finished the climb without experiencing severe hypoglycemia or metabolic decompensation (Gawrecki et al., 2016; Matejko et al., 2017). This proves that with proper preparation and sufficient diabetes-related knowledge, hiking can be a safe and beneficial physical activity for diabetic patients and they should not be discouraged from undertaking such ventures.
It must be remembered that the patients climbing Mount Damāvand were accompanied by qualified health professionals who helped them avoid critical health situations, ensuring a safe expedition for all concerned.
The literature suggests that even if a hiking patient is not accompanied by a doctor, the available technology can facilitate communication between patients and doctors, and in emergency situations, the latter may be able to solve diabetes-related problems on the mountain trail through telemedicine (Szawarski and Hillebrandt, 2017).
Our study has some limitations. Although diabetes-related knowledge among the studied group of Polish mountain leaders was satisfactory, we cannot neglect the fact that the respondents represented only a small proportion of the total number of mountain leaders in Poland. Only 21.2% of Polish mountain leaders replied to our invitation to take part in the study.
The elderly age of some of the guides and consequently their poor computer skills may account for a low response rate. This theory is supported by the fact that a majority of our respondents were between 31 and 40 years of age, which constitutes a range of people who are usually more familiar with modern technologies. Similarly, the study population may not be fully representative of the entire population. It still, however, provides insights into the need for more diabetes-related education and encourages similar studies on larger study groups. The second limitation of our study was the questionnaire itself, which did not include specific questions related to insulin, glucometers, or glucagon management. Regardless of these limitations, this first attempt in medical literature to study diabetes-related knowledge among mountain leaders may inspire future research in this field.
With the increasing popularity of mountain expeditions, there is a need to develop adequate educational programs for mountain leaders related to diabetic emergencies. In over a dozen European countries, including Poland, mountain leaders take practical and theoretical courses, conducted by physicians and mountain leaders, on health issues that could be experienced during mountain climbs (Peters and Plötz, 1998; Peters, 2000). The current training does not specify inclusion of diabetes and diabetic emergencies, which may be why the respondents identified first aid courses and professional training as less common knowledge sources for hypoglycemia (fourth and fifth places in terms of frequency declared, respectively) (Fig. 2).
It would be valuable to extend the curriculum of mountain leaders by introducing the subject of diabetic emergencies and most importantly the need for an immediate response to hypoglycemia, including the use of glucagon injection. In addition to diabetes-related training, the study also identified a need for training in other chronic diseases such as epilepsy and asthma, where exacerbations must be treated immediately.
Conclusions
Knowledge about diabetes among Polish mountain leaders appears to be adequate, especially considering the fact that it is not usually gained from first aid courses. However, there were still topics where mountain leaders' knowledge about diabetes was lower than the average score for a given category and there is a need for further education in these areas.
Footnotes
Author Disclosure statement
No competing financial interests exist.