
Abstract
Abstract
The goals of this study were to characterize headache at high altitude in relation to the severity of acute mountain sickness (AMS), to investigate whether a history of migraine or nonmigrainous headache at low altitude is a risk factor for AMS and to estimate its effect size in relation to established major risk factors. We performed a secondary, extended analysis of data obtained from 1320 mountaineers staying overnight at the Capanna Margherita (4559 m). Headache at low and high altitude was classified according to the criteria of the International Headache Society. About 45% of the mountaineers suffered from headache in the evening of the arrival day at 4559 m. In those with headache, tension type headache decreased from 62% to 29% and 13% with no AMS (AMS-C <0.70), moderate AMS, and more severe AMS (AMS-C ≥1.5), while headache fulfilling the criteria of migraine increased correspondingly from 14% to 34% and 69%. A history of migraine or any type of headache at low altitude is a minor predictor of AMS that does not significantly contribute to AMS risk in a multivariate analysis including the major risk factors such as history of AMS, rate of ascent, and degree of preacclimatization in this population of alpine mountaineers. The association between more severe AMS and migrainous headache may be due to common nonspecific symptoms but a common underlying pathophysiology of AMS and migraine cannot be excluded. Despite this association a history of migraine or other headache at low altitude is not a major risk factor for AMS.
Introduction
H
Larger studies involving between 500 and 800 subjects showed an association between a history of headache or migraine at low altitude and headache at high altitude in subjects flown from 500 to 3700 m (Bian et al., 2013), in mountaineers staying overnight between 2200 and 3817 m (Burtscher et al., 2011), and in hikers ascending and descending in <12 hours between 3438 and 4349 m (Davis et al., 2016). The first two studies did, however, not state how history of migraine was assessed, while Davis et al. (2016) applied the criteria of the International Headache Society (IHS) but cannot exclude confounding effects of exercise (Olesen and Steiner, 2004).
The question whether migrainous headache in the study of Davis et al. (2016) is associated with AMS could not be answered conclusively, since these authors used the Lake Louise criteria for the diagnosis of AMS, which requires headache as a compulsory symptom. A history of migraine at low altitude was a minor independent risk factor for severe AMS in about 1300 trekkers and mountaineers on expeditions (Richalet et al., 2012). These authors did, however, not specify how a history of migraine was assessed.
Considering the discussion about the role of migraine in AMS, we think that our data published as abstract only (Schneider et al., 2002a) could make a valuable contribution because we avoided some limitations of the abovementioned studies (i) by defining AMS by the AMS-C score, which does not require headache as a compulsory symptom, (ii) by classifying headache at low and high altitude according to the criteria of the his, and (iii) by obtaining AMS-C scores also after an overnight stay, when symptoms are usually most prominent and not confounded by short-term effects of exercise. Thus, we investigate whether a history of migraine or non-migrainous headache at low altitude is an important risk factor for AMS in our cohort, and we characterize headache at high altitude in relation to the severity of AMS. In addition, we evaluated the effect sizes of migraine and nonmigrainous headache at low altitude in relation to other well-known risk factors that had already been published in this cohort (Schneider et al., 2002b).
Having a large data base that includes the major known risk factors for AMS and a history of headache at low altitude, characterizing headache by the criteria of the IHS, and defining AMS by a score, which does not require headache as a compulsory symptom, allows a thorough examination of the relationship between migraine and AMS and thus justifies a secondary analysis of our in part previously published data (Schneider et al., 2002b).
Methods
Study design and subjects
This study is in part a secondary and extended analysis of a large epidemiological study on risk factors of AMS in mountaineers staying overnight at the Capanna Margherita (4559 m) (Schneider et al., 2002b). In addition to the published data based on AMS scores obtained in the first morning at 4559 m in 829 subjects we included data of another 491 subjects of whom only AMS scores in the evening of the arrival day were available. Thus, in the years 1996–2000 overall 1320 mountaineers were interviewed after their arrival at 4559 m. We focused in this analysis on classifying headache at high altitude according to the criteria of the IHS and on exploring whether a history of headache at low altitude is a risk factor for AMS. About 55% of all mountaineers staying overnight at the Margherita-hut participated in this survey. Each year, data were collected by different investigators obtaining informed consent from the subjects. The protocol of the study was approved by the Ethics Committee of the Medical Faculty of the University of Heidelberg.
Mountaineers who had ascended to the Capanna Margherita for an overnight stay were asked for their participation. Most of them reached the hut by walking over technically easy terrain (glaciers and mountain trails) spending a variable number of days in huts at intermediate altitudes, ranging from 2882 m (Monte Rosa hut) to 4176 m (Balmenhorn biouvac). The preferred ascent from the Italian side passes via the Gnifetti hut (3625 m).
The mountaineers filled out questionnaires about previous exposures, symptoms of AMS during previous exposures, mountaineering activities during the last 2 months, rate of ascent, drug and alcohol intake during the actual ascent, training history, history of headache at low altitude, smoking, habitual alcohol intake, body weight, body height, gender, and age. AMS scores were assessed in 1306 mountaineers 4–6 hours after arrival and additionally in a subgroup of 829 mountaineers in 1996, 1998, and 2000 in the following morning before leaving the hut. All questionnaires were available in Italian, German, and French to avoid incorrect answers due to insufficient foreign language skills.
Assessment of susceptibility to AMS, preacclimatization and rate of ascent
This is described in detail in the previous publication (Schneider et al., 2002b). Briefly, the frequency of the symptoms of AMS with exposures above 3000 m is scored from never (0 points), seldom (1 point), often (2 points), and regularly (3 points) and nonsusceptibility is defined as headache frequency ≤1 and a total score history score <4. Preacclimatization is defined as number of days spent above 3000 m in the last 2 months. Rate of ascent is the average daily gain in altitude of the overnight stay between 2000 and the final altitude (4559 m).
Assessment and classification of headache at high altitude
Mountaineers filled out another questionnaire asking about the severity and characteristics of acute headache and associated symptoms 4–6 hours after arrival in the hut. The intensity was scored as no headache ( = 0), mild ( = 1), moderate ( = 2), and severe ( = 3) headache. The characteristics of acute headache were assessed by binary scale (present/not present) for one-sided, both-sided, dull, pulsating, forcing reduction of activity and aggravation by movement, and for the presence or absence of nausea, vomiting, photophobia, or sonophobia. Based on this information headache was diagnosed as migraine, tension, or other type of headache using the criteria of the Kiel Headache Questionnaire (KHQ) (Gobel, 1994) that is based on the criteria of the IHS. Headache was considered to be migrainous when at least two of the four headache characteristics (one-sided, pulsating, forced to reduce activity, and aggravation by movement) and at least one of the following symptoms: nausea, vomiting, photophobia, and sonophobia were present. Nonmigrainous headache was considered to be of the tension type when at least two of the following four characteristics (both-sided, non-pulsating, not forcing to reduce activity, and no aggravation by movement) and no nausea, vomiting, photophobia, or sonophobia were present. Headache that did not fulfill the criteria for migrainous or tension type, was classified as “other type of headache”.
History of headache at low altitude
Subjects were also asked 4–6 hours after arrival at the hut about the frequency of headache at low altitude (none within the last year, less than once in a month, and less and more than once per week). If they had had at least one episode of headache in the last year, they were asked to fill out a KHQ and headache was classified as described above.
Assessment of AMS
AMS was assessed by the AMS-C score of the abbreviated Environmental Symptom Questionnaire (Beidleman et al., 2007). This comprises the following 11 items that are graded from 0 (not present) to 5 (extremely severe). The factorial weight of each item is given in parenthesis: light-headed (0.489), headache (0.465), dizziness (0.446), feeling faint (0.346), dim vision (0.501), off-coordination (0.519), feeling weak (0.387), sick to stomach (0.347), loss of appetite (0.413), feeling sick (0.692), and feeling hungover (0.584). To obtain the AMS-C score, the sum of all item scores multiplied by the respective factorial weight is multiplied by 5 and divided by 25.95. A criterion score of ≥0.70 indicates AMS. This score was shown to correctly identify 60% of subjects reporting sick and 98% of subjects not reporting sick at high altitude (Sampson). AMS-C score of 0.70 corresponds to a Lake Louise Score (self-report) of 4 (Bärtsch et al., 1993). AMS-C score >1.5 was considered to indicate more severe AMS.
Further parameters
History of AMS
Subjects were asked whether each of the five major symptom complexes of AMS (headache, gastrointestinal symptoms, dizziness, insomnia, and peripheral edema) occurred never ( = 0), seldom ( = 1), often ( = 2), or regularly ( = 3) during exposures at altitudes ≥3000 m. For gastrointestinal symptoms the highest score of any of the three items (loss of appetite, nausea, or vomiting) was scored. The Lake Louise Consensus Conference defined AMS as headache plus one of the additional symptoms mentioned above in the context of a recent gain of altitude (Roach et al., 1993). With respect to this definition, we rather chose to define nonsusceptibility than susceptibility to AMS. Individuals who reported having never or seldom headache (score ≤1) at high altitude and who had a total score <4 were considered to be not susceptible to AMS. History of AMS was only obtained from mountaineers who had a minimal average yearly exposure to altitudes above 3000 m of at least 1 day.
Preacclimatization was evaluated by the number of days spent above 3000 m in the previous 2 months, not including the present exposure. The rate of ascent was expressed as days spent above 2000 m including the arrival day during the present exposure.
Medication
We have data on drug intake only in those mountaineers with AMS scores in the morning. About 2.2% of the study population took dexamethasone (3 mountaineers) or acetazolamide (15 mountaineers). One hundred seventy-three mountaineers (22%) had taken ibuprofen, diclofenac, salicylic acid, or acetaminophen before or during the study. Intake of analgesics was significantly more frequent in those with versus without AMS (44.3% vs. 25.5%).
Missing values
This investigation is based on the analyses of epidemiological data collected between end of July and end of August in the years 1996, 1997, 1998, and 2000 by different researchers. A total of 1320 mountaineers were enrolled in these studies. One thousand three hundred six mountaineers filled out a questionnaire about headache at 4559 m (98.9%). The AMS score in the evening was obtained in each year (n = 1302 of 1320, 98.6%). Data on preacclimatization were available in 99.1% (n = 1302), on rate of ascent in 99.5% (n = 1313), and on history of previous altitude exposures in 95.7% (n = 1263) of the mountaineers. The AMS-C-Score in the morning and the frequency of headache at low altitude (which is not obtained by the KHQ) were not assessed in 1997 and AMS-C scores are missing from 70 consecutive cases in 1996. Therefore, the AMS-C scores and headache frequency at low altitude are reported only in 829 (62.8%) and 899 (68.1%) mountaineers, respectively. These serial missing values do not depend on the study endpoints and thus do not affect the results of our analysis. They are classified as missing completely at random according to Rubin (1987). Furthermore, 97 of 1320 mountaineers (7.3%), mostly with a headache frequency of less than one a month, declared that they did not suffer from migraine and refused filling in the KHQ.
Multivariate analysis was performed with the datasets containing AMS in the morning as dependent variable and susceptibility, preacclimatization, rate of ascent, and migraine or any type of headache at low altitude as independent variables. The datasets were analyzed by complete case analyses (National Research Council, 2010). The completeness of the multivariate datasets were 679 of 829 (81.9%), if migraine was an independent variable and 748 of 829 (90.2%) if any type of headache at low altitude was an independent variable.
Statistics
Statistical analysis was performed by statistical software R (Version 3.4.0). For bivariate comparisons we used chi squared test, Cochran-Armitage test for trend, and t-test for independent samples and heterogenouos variances (Welch test). For proportions we calculated the exact confidence intervals. For multivariate analysis we used logistic regressions (function glm of package R base). The following variables were included in the equation that was performed with forward and backward selection: age, sex, alcohol, smoking, training, AMS susceptibility, ascent rate, preacclimatization, migraine at low altitude, any headache at low altitude, analgesics, and drugs for prevention of AMS. Since the results were identical with the previously published data (Schneider et al., 2002b), we do not present the full data here and report the results of the significant factors plus the newly added parameters on headache at low altitude only. A significant effect of multicollinearity in the multivariate logistic regression can be excluded, since the correlation coefficients in a correlation matrix of all included parameters were between r = −0.128 and 0.319. Because of the explorative character of the study, p-values were not adjusted for multiple comparison.
Results
Table 1 presents an overview of the investigated mountaineers. The average age is 38 years, 18% are female, and the average body weight and height are normal. About 62% of the participants reported having episodes of headache at low altitude with variable frequency, among them there are 131 mountaineers (prevalence 10.7%) with a history of migraine at low altitude. The latter was more frequent in women (15.0%) than men (9.7%). Around 45% of all mountaineers had headache in the first hours after arrival at 4559 m. The prevalence of AMS was lower in the evening of the arrival day (17.8%) than on the following morning (29.2%).
Characteristics of the Examined Population
AMS-C score in the morning were obtained in the years 1998 and 2000 only.
AMS, acute mountain sickness; SD, standard deviation.
Table 2 shows the characteristics of the headache at 4559 m in light, moderate, and severe headache. With increasing severity of headache there is a highly significant trend for pain to become more pulsating and impacting activity and being aggravated by movement and more often accompanied by symptoms like nausea, vomiting, photophobia, and sonophobia. The increase of one-sided headache from 23% up to 29% is not significant and both-sided headache shows no trend at all with increasing severity of headache. Using the criteria of the KHQ it follows that migrainous type headache increases from 18% to 63% and the tension type headache decreases from 57% to 16% with light versus severe headache. This shift of the headache types is highly significant. However, the proportion of low altitude-migraineurs does not significantly change between the three groups with different severity of headache (p = 0.36).
Characteristics of Headache in Dependence on the Severity
Proportions with 95% confidence intervals.
Chochran-Armitage test for trend.
Since headache is the major symptom of AMS and more severe AMS is accompanied by nausea and vomiting, it is not surprising that a rise of migrainous type of headache and a decrease of tension type headache occur with increasing AMS scores as shown in Figure 1. The frequency of any headache at high altitude increases from 37.2% in those without AMS, to 81.4% in those with AMS-C scores between 0.7 and 1.49 and to 93.9% in those with AMS-C scores ≥1.5 (Data not shown).

Migrainous and tension type headache in relation to the AMS-C score. Percentage of all subjects with headache who have tension type or migrainous type headache at three levels of AMS-C scores 4 hours after arrival at 4559 m. The difference to 100% indicates headaches that do not fulfill the criteria for tension type or migrainous headache. The p-value refers to the significant trend for both characteristics of headache. A score of <0.7 indicates absence of AMS (n = 383), between 0.7 and <1.50 mild to moderate AMS (n = 144), and ≥1.5 more severe AMS (n = 46). AMS, acute mountain sickness.
Table 3 compares the distribution of symptoms of AMS between those with and without a history of migraine at low altitude. Symptoms of AMS are not significantly different between these groups with the exception of headache and nausea, which are both more frequent in those with a history of migraine. Table 3 also shows that migraineurs suffer more from migrainous type of headache at high altitude in comparison with nonmigraineurs (28% vs. 16%, p < 0.001) and that a higher percentage of migraineurs (66% vs. 40%, p < 0.0001) are susceptible to AMS as judged by their previous mountaineering history.
Symptoms of Acute Mountain Sickness and Type of Headache in Relation to History of Migraine
Table 4 shows the continuously scaled values of established risk factors for AMS in this setting (Schneider et al. 2002b) and the AMS-C scores in the evening and following morning for those with and without a history of migraine. Migraineurs have a significantly higher history score (4.88 vs. 3.43, p < 0.0001) and they ascended slightly more slowly but had 1 day less presacclimatization. These differences are small but close to statistical significance as is the higher AMS-C score in the evening. The AMS-C scores increase considerably overnight, but the small difference between groups is not significant.
History of AMS, Days of Ascent, Days of Preacclimatization, and AMS-C Scores in Those With and Without a History of Migraine
t-test for independent samples and heterogeneous variances (Welch test).
AMS-C score in the morning was obtained only in the years 1996, 1998, and 2000.
CI, confidence interval.
Table 5 shows the prevalence of AMS in the evening and the following morning in relation to the frequency of headache of any type at low altitude. It demonstrates a significant increase of AMS at both time points with more frequent headache at low altitude. The multivariate analysis shown in Figure 2 (right half) demonstrates, however, that headache of any type at low altitude is not a significant risk factor, when the risk factors for susceptibility to AMS, rate of ascent, and degree of preacclimatization are included in the prediction model. Figure 2 left side shows that this is equally the case when history of migraine is taken into the multivariate equation. Thus, a history of migraine or frequent headaches of any type at low altitude are weak risk factors in comparison with AMS history and susceptibility and preacclimatization. Logistic regression of a worst case scenario coding all individuals, who had taken drugs within the last 48 hours, as having AMS confirmed the risk factors susceptibility, rate of ascent, and preacclimatization, while a history of migraine or any headache at low altitude remained not significantly associated with AMS (data not shown).
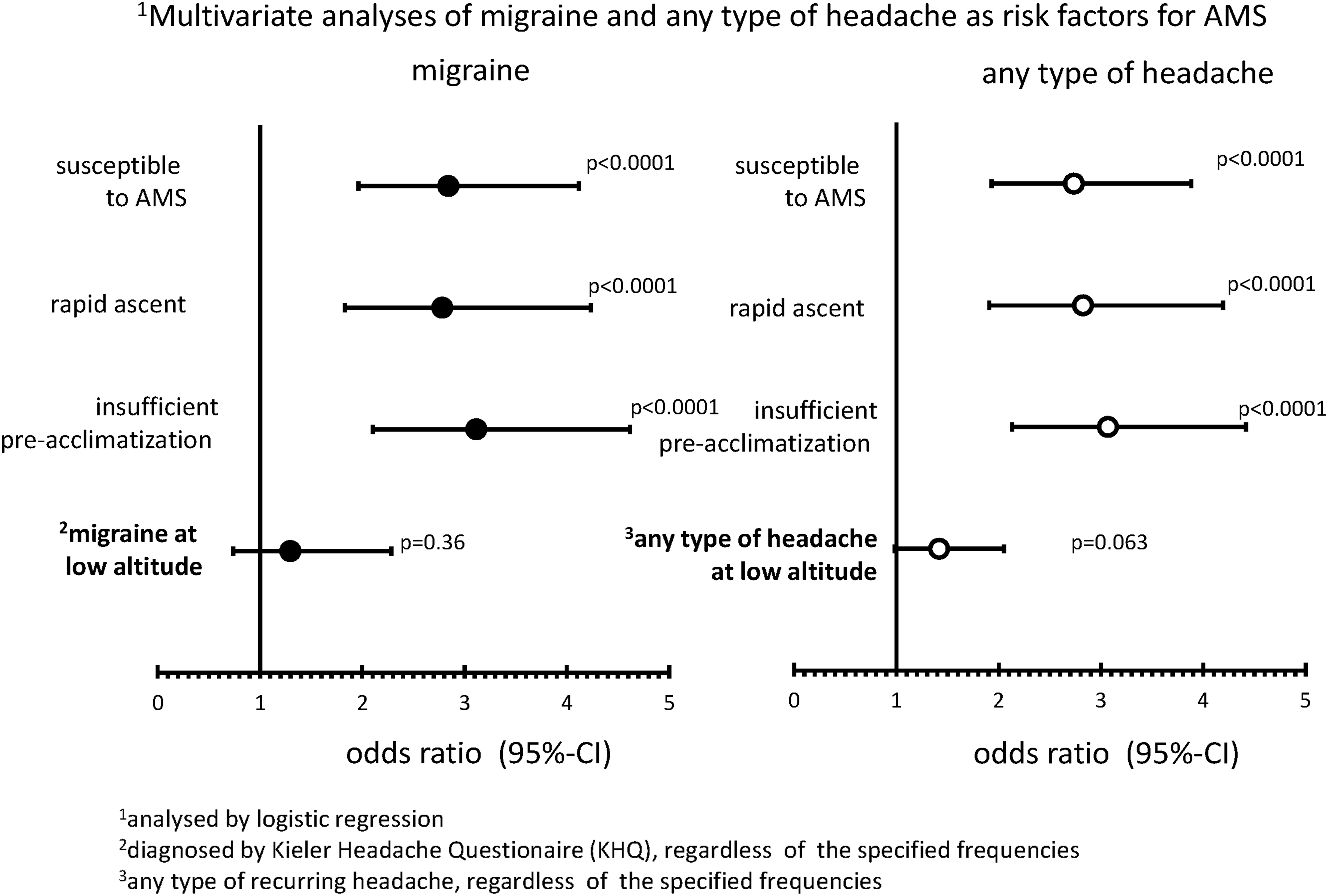
Multivariate analyses of migraine and any type of headache as risk factors for AMS. Multivariate analysis by logistic regression including a history of migraine (left side) and including a history of any type of headache at low altitude (right side). Migraine was diagnosed according to the criteria of the International Headache Society, any type of headache includes all subjects reporting headache at low altitude regardless of specified frequency. For definition of susceptibility, rapid ascent, and insufficient preacclimatization see “Methods” section.
Prevalence of Acute Mountain Sickness in Relation to Frequency of Any Type of Headache at Low Altitude
Values in [ ] are 95% confidence intervals.
Discussion
The major results of this investigation demonstrate that 45% of the mountaineers suffer from headache in the evening of the arrival day at 4559 m and that the characteristics of headache change with the severity of AMS. Tension type of headache is present in 62% of mountaineers with headache but without AMS (AMS-C Score <0.7), while headache fulfills the criteria of migraine in 69% of those with more severe AMS (AMS-C Score ≥1.5). A history of migraine or a history of any headache at low altitude are minor predictors of AMS that do not significantly contribute to the AMS risk in a multivariate analysis including the major risk factors such as history of AMS, rate of ascent, and degree of preacclimatization in our population of mountaineers.
It is unlikely that these findings are due to self-selection eliminating migraineurs in our population of mountaineers, since the prevalence of migraine at low altitude was in the expected overall range (10.7%), lower in male (9.7%) and higher in female mountaineers (15%). This gender-based difference of prevalence of migraine is comparable with values reported in a meta-analysis of 7.5% in male and 16.6% in female subjects (Stovner et al., 2006).
Univariate analysis shows an increased susceptibility to AMS in migraineurs of 66% versus 40% in nonmigraineurs, which is mainly due to headache and nausea (Table 3) resulting in a greater history score. This did not, however, result in significantly higher AMS-C scores in the evening (p = 0.057) and next morning (p = 0.17) in this study (Table 4). Other risk factors like rapid ascent and insufficient preacclimatization, despite not being significantly different at a univariate level (Table 4), had a much higher weight than history of migraine in the multivariate analysis as shown in Figure 2. This finding is confirming the minor role of history of migraine as an AMS risk factor in a multivariate analysis as reported also by Richalet et al. (2012) in a prospective trial. Other studies identifying a history of migraine or headache at low altitude as a risk factor for AMS (Burtscher et al., 2011; Bian et al., 2013; Davis et al., 2016) did not evaluate the effect of headache or migraine in a multivariate model including major, well-established risk factors. We found also a significant trend to higher AMS-C scores with increasing frequency of any type of headache at low altitude by univariate analysis (Table 5) whereas multivariate analysis including the major risk factors mentioned above revealed no significant increase in the odds ratio for AMS by including headache of any type at low altitude Fig. 2). However, because of the low number of mountaineers who had more than one episode of headache per week (Table 5), we cannot exclude that very frequent headache of any type at low altitude might be an independent risk factor for AMS.
Our findings are in agreement with the results of previous studies showing that headache at high altitude may have characteristics of migraine (Silber et al., 2003; Serrano-Duenas, 2005; Broessner et al., 2016; Davis et al., 2016). We extend these findings by demonstrating that migrainous headache is predominantly associated with more severe AMS. This is due to descriptive, nonspecific criteria for the diagnosis of migraine that can also accompany more severe AMS as shown in Table 2: nausea, vomiting, aggravation by physical activity, pulsating quality, sonophobia, or photophobias. Whether this association points to a common underlying pathophysiology for migraine and AMS or is unrelated has not been resolved yet. It had been suggested that activation of the trigemino-vascular system that occurs in migraine might also be triggered by hypoxia (Sanchez del Rio and Moskowitz, 1999). Trials with sumatriptan for prevention and treatment of AMS were, however, not conclusive (Utiger et al., 2002; Jafarian et al., 2007).
As expected, AMS prevalence in the whole study population (Table 1), AMS-C scores in migraineurs (Table 4), and AMS prevalence in relation to headache of all causes at low altitude (Table 5) were lower in the evening versus the following morning. This is in agreement with studies in the field and in normobaric chambers (Hohenhaus et al., 1994; Beidleman et al., 2013) showing that AMS increases overnight at a given altitude. However, the difference in scores and prevalence of AMS between evening and morning had no effect on the analysis of the role of a history of migraine or headache of any type as risk factors for AMS in the univariate and multivariate analysis (data of multivariate analysis with evening scores not shown). This may be due to a delay of several hours between arrival in the hut and examination thus avoiding potentially confounding effects of exercise inducing headache, fatigue, or exhaustion.
Compared with an epidemiologic study performed 10 years earlier in 136 mountaineers at the same location, AMS prevalence was about 10% lower (Maggiorini et al., 1998). This may be due to behavioral changes over time or variability by chance in the smaller sample of the earlier study. Furthermore, intake of nonsteroidal anti-inflammatory drugs (NSAIDs) during ascent in about 20% of the mountaineers without AMS in this study may have lowered prevalence of AMS somewhat.
Study limitations
Data were collected between 1996 and 2000 and the primary analysis on major risk factors of AMS were published in 2002 (Schneider et al., 2002b). More recent publications on headache in AMS made us perform a secondary analysis of the data with a focus on this topic, since we had unpublished data, the collection of which had avoided some of the shortcomings of the more recent studies as mentioned in the introduction. The basic data on AMS and headache were collected in studies with slightly different focus. Therefore, there are some missing values. The vast majority of missing values are, however, completely at random, which is considered not to bias the results of the analysis (National Research Council, 2010).
Intake of drugs can be a confounder in such epidemiologic studies. NSAR intake was associated with significantly higher prevalence of AMS and is likely a consequence of illness rather than a cause or risk factor. NSAR predominantly affect headache and thus have less effect on assessing AMS by the AMS-C score compared with the Lake Louise score. Nevertheless, NSAR may have prevented the diagnosis of AMS at the time of examination in some individuals. The intake of drugs preventing AMS (diamox or dexamethasone) can be neglected, since it occurred in 2.2% of the study population only. In addition, a worst case scenario classifying all mountaineers, who had taken drugs within the last 48 hours, as having AMS did not significantly change the results of the logistic regression.
Furthermore, recall bias may have affected our results. Since most questions addressed previous headache or symptoms of AMS occurring repeatedly and are therefore likely to be remembered we assume that recall bias was minimal.
Finally, this is a cross-sectional study in a representative sample of alpine mountaineers, who train on average 8 hours per week and who are capable of climbing at altitudes up to 4500 m. Therefore, caution must be applied when extrapolating the conclusions to different settings such as lower altitudes, passive ascent, and tourist populations.
Footnotes
Acknowledgments
The authors thank Dirke Bernasch, Jörn Weymann, and Dominik Uttiger for their help with collecting the data at the Margherita hut.
Author Disclosure Statement
No competing financial interests exist.