
Abstract
Abstract
Objectives:
We sought to characterize the mental health morbidity associated with avalanche rescue, and to generate hypotheses as to how such morbidity may be mitigated.
Materials and Methods:
Avalanche first responders were recruited through online advertisements, social media, direct outreach, and e-mail solicitation. Thirteen subjects were selected for inclusion. Each subject participated in a semistructured interview. Transcripts were coded and thematically analyzed.
Results:
Themes identified from interviews fell into three broad categories: long-term effects of rescue participation, assessments of psychological support, and recommendations for change. Symptoms of substance use disorder, depression, anxiety, panic, acute stress disorder, and posttraumatic stress disorder were evident in the interviews, as was evidence of adverse effects on subjects' personal relationships. Many respondents described a deficiency of formal psychological support for avalanche first responders, often limited to after-action debriefs of varying effectiveness. Nevertheless, subjects who received high-quality professional psychological support considered it helpful. Participants' suggestions for improvement focused on formalizing preincident psychological preparation and postincident support.
Conclusions:
Avalanche responders may experience long-lasting, work-related psychological effects. There is a paucity of effective psychological preparation and support for this population of first responders. Formal psychological support is positively received when available. Further study is required to evaluate particular interventions in this specific population.
Introduction
D
Recent years have heralded an emerging awareness of the vulnerability of ski town communities to mental illness. Mental health providers have attributed this phenomenon to a culture of rugged individualism, ready access to firearms, and lack of mental healthcare in mountain communities. Moreover, social factors in these communities—including profound wealth disparity, lack of social cohesion due to transient populations, unreliable seasonal employment, and substance use—serve to exacerbate the issue (McMillan, 2016). Many avalanche rescue personnel are likely to live and work in vulnerable communities like these.
We hoped to learn more about the effects of avalanche rescue work on first responders in the prehospital setting. Adverse psychological effects in other first responders such as paramedics (Roden-Foreman et al., 2017), firefighters (Jahnke et al., 2016), police officers (Marmar et al., 2006), and responders to terrorist events (Wesemann et al., 2018) are well documented. Several studies have demonstrated that rates of PTSD and acute stress disorder are higher in search and rescue and disaster response workers, such as canine handlers, emergency medical technicians, and firefighters (Benedek et al., 2007). Few studies specifically pertain to avalanche rescuers (in particular, ski patrollers and search and rescue workers). Yet, this group interfaces with one of the most dramatic types of trauma with some regularity. One prior investigation of professional and volunteer rescue workers in avalanche conditions found that volunteer responders experience PTSD symptoms more often than professionals (Haraldsdottir et al., 2014).
It is difficult to estimate the prevalence of psychopathology among avalanche rescue workers, in large part, due to the apparent rarity of formal diagnoses. Rural areas, where many backcountry first responders are apt to live, have a greater likelihood of shortages of mental health professionals like psychiatrists and psychologists and, as such, less access to relevant care (National Advisory Committee on Rural Health and Human Services, 2004).
This study aims to describe the psychological burden in prehospital avalanche responders, with a view to elucidating how such individuals might be more effectively psychologically prepared and supported preincident and postincident.
Materials and Methods
Individuals who had directly participated in one or more avalanche rescue events were recruited through online advertisements, outreach to mountain rescue organizations, solicitation through e-mail, social media, and personal communication to backcountry ski communities in Wyoming, Utah, and Colorado. Interviews with individual subjects often led to referrals to subsequent potential participants. Inclusion required personal involvement in avalanche first response human rescue within the past 10 years. No exclusion criteria were used. Numerical identifiers were assigned to study subjects to protect confidentiality, and the confidential nature of the study was explained to subjects. Thirty potential subjects were identified, 18 expressed willingness to participate, and 13 ultimately completed the full interview. All willing and qualified subjects were interviewed, and each was interviewed only once. Of the five who did not ultimately participate, one was unable to due to unanticipated health problems and four were unavailable due to scheduling conflicts.
Semistructured interviews were conducted with each subject; each typically lasted 20–40 minutes. One investigator (N.D.) conducted all interviews to maintain consistency, and interviews were conducted through telephone due to the wide geographic distribution of subjects. Questions were generalized and pluralized for subjects who had experienced multiple avalanche rescues. Digital voice-recordings were created and thereafter assigned a numerical identifier.
After data collection, verbatim transcripts of each interview were created and analyzed. Demographic data were collected and reported in aggregate. Qualitative data were analyzed using NVivo software (QSR International, Burlington, MA). A grounded-theory approach (Choo et al., 2015) was used to analyze and code transcripts, based on themes related to the study questions as well as topics that arose de novo during the interview process. Both authors reached consensus on assigned codes and themes.
The study was approved by the Institutional Review Board of Columbia University Medical Center.
Results
The demographic characteristics of participants are shown in Table 1. The majority of participants were 25–44 years old (54%), were male (92%), and had experience in professional mountain rescue (93%). All subjects had basic medical training, but there was a wide range of avalanche rescue training experience (Fig. 1).
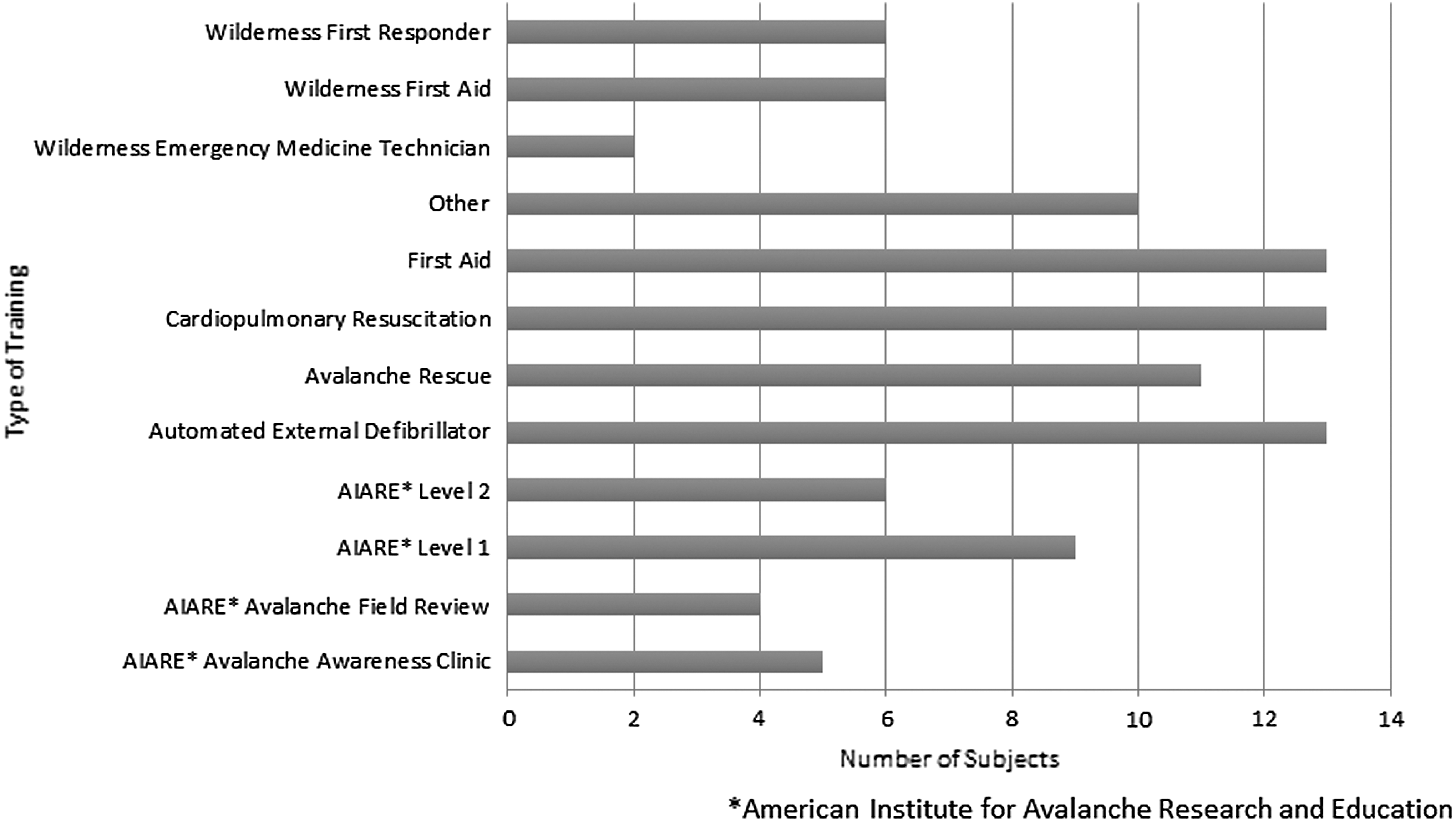
Formal training experience of avalanche first responders.
Experienced multiple avalanche events with different characteristics.
Coding and analysis identified three broad categories pertaining to avalanche rescue: long-term effects, impact of psychological support, and improvement recommendations.
Subjects reported many psychological, personal, and professional effects of avalanche rescue (Table 2), including a wide range of mental health effects. Representative responses included the following:
PTSD, posttraumatic stress disorder.
“I can only explain this in an analogy—I teach pre-hospital medicine and if I talk about a particular incident or situation I can bring gravity to a situation by adding emotion to it. When I do that once it's powerful, when I can't hold it together a second time it's like ‘ah that poor guy,’ but when it happens a third time it's like ‘can somebody get that guy some help because this is really uncomfortable?’”
“I'll go back to the lack of sleep or the difficulty in sleeping. I refer to it as ‘the movie plays on’ where you get the privilege of experiencing that event over and over again, and then the awesome experience of having a different event trigger the same hormonal release and then you get to experience the same event again. I laugh when people talk about the avoidance of trauma-related thoughts—you can't get them out of your head.”
“I had to find that discipline to be able to have fun again, meaning to be able to go out into the mountains with my friends and be able to have a very good time. At one point in my life, I was having difficulty doing the things that I enjoy the most because of what I experienced in that environment; I was going out there and I would be like, ‘OK, so am I going to see dead out here today?’”
The interview was not structured to determine whether participants met formal diagnostic criteria for any particular psychiatric disorder. Nonetheless, subjects often revealed symptoms such as panic, anxiety, and depression, as well as components of PTSD (American Psychiatric Association, 2013). The use of alcohol to self-medicate and facilitate conversation about rescue missions was prevalent among participants. Percentages of total respondents who exhibited specific mental health symptoms are shown in Figure 2.
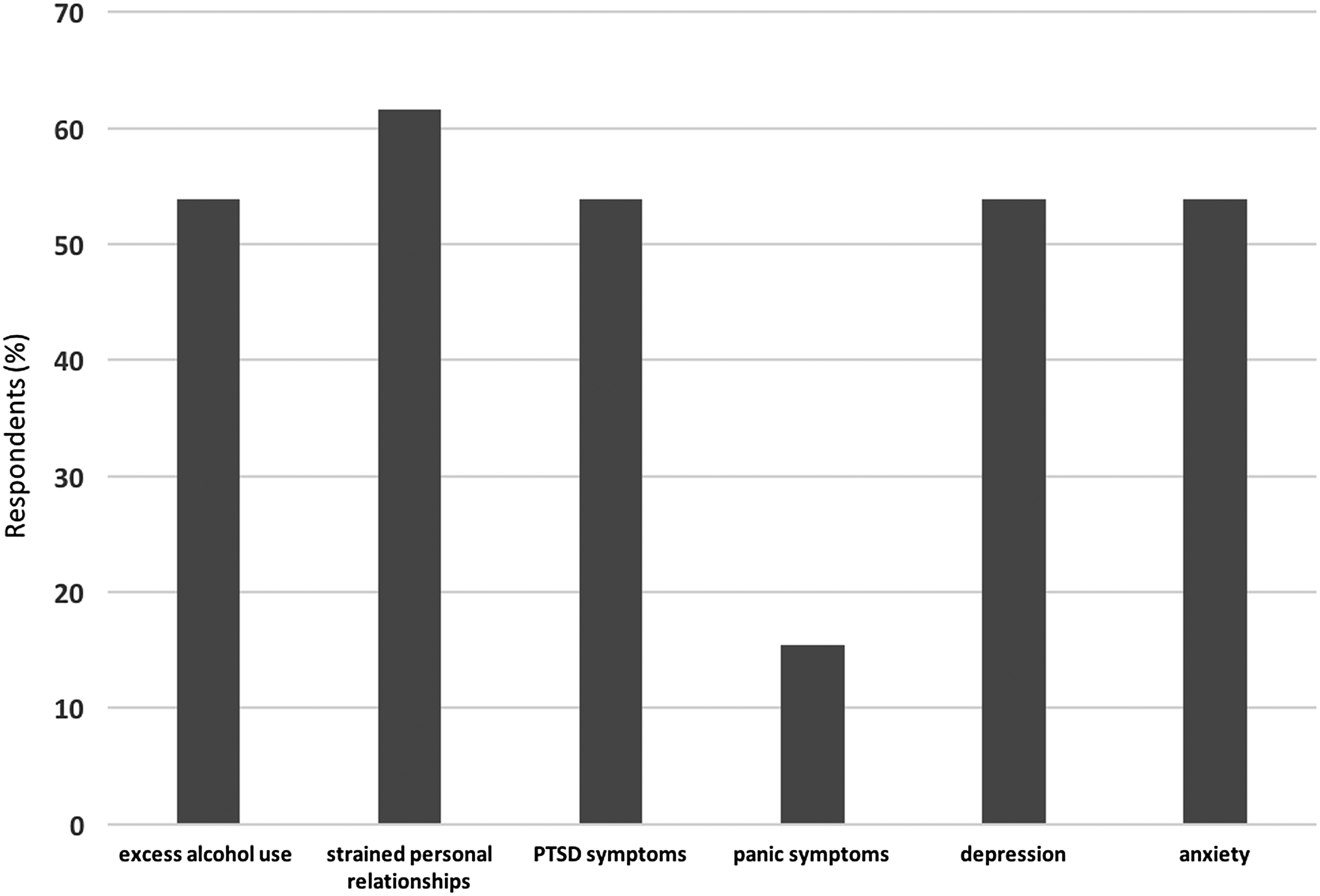
Frequency of mental health-related symptoms among avalanche responders.
Symptoms often persisted on the order of years. Many described long-lasting negative effects of rescue experiences:
“I'm five years out and I'm still talking about stuff.” “A couple of weeks, as far as I know. But since I've given up alcohol, I think they've probably lasted a couple of years, but were just never dealt with….”
In their personal lives, subjects reported experiencing feelings of social isolation and strained relationships—in two instances resulting in relationship breakdown.
However, in the professional setting, subjects generally reported positive effects: a deep sense of career satisfaction, strengthening of bonds with coworkers, and a high level of respect within the workplace:
“Having the opportunity to take care of those patients in those sometimes challenging situations gives you a good experience to continue your professional development.” “Professionally, I think [the rescue experience] has gained me more respect from my peers, from my coworkers. It has caused me…to have a desire to sharpen my skills on a constant basis–to stay on top of my game.”
Despite these positive professional effects, some subjects complained of occasional symptoms of burnout:
“I got to a point where I thought maybe I should get out of this world and not do this anymore.”
Multiple themes arose related to the availability and effectiveness of psychological support (Table 3). Subjects tended to report an ingrained culture of stoicism and a paucity of psychological support within the backcountry community, but acknowledged a growing awareness of and responsiveness toward psychological issues in recent years:
“People in the room venting about what went wrong and then being told to put their boots on and go to work the next day—that's the culture that I worked in for 20 years and that I'm happy is finally starting to change.”
Participants generally considered informal psychological support from social support networks to be the most effective aid:
“I think the best support is just being around those people, without really even needing to talk that much, just being around [them]. The folks that I have the best relationships with are arguably the best informal psychological support.” “A lot of that just comes from our team or our community. We live in a pretty small community, so people will know that there's been an incident in the community and they'll reach out and get in touch; they'll drop cookies off at the building where we rescue from, team members take care of each other, offering to help with babysitting with kids or whatever else they need if somebody is really struggling.”
In some cases, respondents described the informal support network as insufficient:
“Ski patrollers and avalanche workers are great dark humor comedians. Informally we are always standing around having a beer—or six—depending on how bad of a day it was and joking. The famous joke around here is, ‘that was the deadest man I've ever seen.’ It is effective to some extent—that camaraderie is key, and a lot of patrollers report being able to disassociate with it and they have no problems. For some people, such as myself, it was effective for a long time, but it ceased to work and I finally broke.”
The main modality of more formal psychological support described was after-action debriefing—often incorporating elements of psychological first aid—which ranged widely in quality and utility. Respondents favored formal group-based and individualized options in instances where high-quality ones were available, but felt that debriefs were often inadequate when facilitators lacked appropriate training (Table 3).
Many respondents offered suggestions as to how the psychological effects of rescue work could be mitigated (Table 4). Avalanche rescuers generally regarded their formal avalanche training highly, but endorsed a clear need for greater preincident and postincident support:
“My first aid training and experiences made me adequately prepared to deal with the real event, but I had never received any psychological preparation. The actual psychological trauma—no, I wasn't prepared at all. I don't think any ski patrollers get any psychological training to deal with it.”
“I think that just letting people know that these events are very traumatic and have very serious effects should probably be more of a component in the training. When I teach avalanche training myself, I try to impress upon people that it isn't about being a tough guy or anything else, but it's about being honest that it affects people very differently and that there is professional help out there.”
Additional recommendations for improvement included training exercises with greater emphasis on the physical intensity and psychological risks of avalanche work, after-action debriefs utilizing mental health professionals, proactive long-term psychological monitoring and support, and individualized psychological support when necessary.
Discussion
This qualitative study examined the long-term psychological, personal, and professional effects of avalanche rescue work on first responders, as well as the perceived availability and sufficiency of psychological support for such individuals. Participants suggested improvements to avalanche training programs as well as preincident and postincident psychological support.
Long-term effects
Avalanche rescue work is likely associated with a wide range of mental health sequelae that escape formal diagnosis. One of the most striking themes to emerge is a culture of alcohol dependency within the backcountry rescue community. While some subjects reported only a slight increase in their alcohol consumption in the immediate wake of an incident, others openly admitted to substantial self-medication with alcohol as a means of coping with occupational stress. Drinking establishments commonly serve as venues for informal postincident debriefs in the backcountry rescue community.
In addition to varying degrees of alcohol use, subjects also described symptoms of depression, anxiety, panic disorder, acute stress disorder, and PTSD. Indeed, prior studies have demonstrated that disaster responders with more frequent or severe PTSD symptoms are more likely to drink as a coping mechanism (Stewart et al., 2004). The relationship between alcohol use and other psychological morbidity in this population warrants further attention.
Psychological support
There was consensus among subjects that, historically, limited psychological support has been available to avalanche first responders; nonetheless, respondents indicated that the situation has been improving. We observed a culture of stoicism in the rescue community, resulting in lack of awareness, dialogue, and support pertaining to the psychological effects of traumatic rescue work. However, in recent years, there seems to be a growing awareness of and responsiveness to this issue, although to varying degrees depending on location and institution.
After-action debriefing sessions reportedly vary dramatically in effectiveness, ranging from informal discussions to formal sessions overseen by experienced clinicians. Consequently, there is considerable variation regarding the effectiveness of these debriefs, leading to strongly held opinions about their utility. No subjects reported engaging in the newer practice of psychological first aid, although components of it—including contact/engagement, comfort, practical assistance, and linkage with services—were occasionally offered.
Suggested improvements
The technical aspect of avalanche training is generally highly esteemed within the backcountry rescue community, but there is a clear need to better prepare rescue workers for the physical intensity and psychological trauma of avalanche response. While this study suggests that it may not be possible to prepare avalanche first responders for the psychological impact of backcountry rescue, it suggests a number of potentially measurable changes to the current system: first, responders suggested that avalanche training should incorporate more physically intense drills and emphasize the psychological morbidity associated with real-life incidents. Second, respondents felt that after-action debriefs should routinely involve trained mental health professionals. And finally, long-term psychological support may be improved by being more proactive, incorporating periodic professionally mediated workshops, ongoing monitoring from medical professionals, and individualized psychological support where needed.
Exclusions
Certain interview data were disregarded in the analysis. Quantitative data pertaining to the state of the victim(s) and presence of an air pocket(s) were omitted due to widespread difficulties recalling such details among subjects. Qualitative data pertaining to Incident and Prehospital Interactions questions were disregarded due to lack of cohesive themes therein.
Limitations
This study has limitations. Although the study size is sufficient to generate hypotheses it may not be possible to make generalizable conclusions, given the sample size, overrepresentation of male and professional first responders (92% male, 93% professional), underrepresentation of female and layperson responders, and geographic limitation to subjects in Utah, Wyoming, and Colorado. Moreover, it is possible that the small sample size is not large enough to elucidate all underlying themes; however, the recurrence of themes in multiple interviews suggests a degree of saturation that implies that major themes have been identified.
Furthermore, bearing in mind that questions pertaining to mental health are deeply personal, subjects may have felt uncomfortable being completely open in a single interview conducted over the telephone. The primary mode of outreach was to professional avalanche rescue organizations; upon establishing contact with these organizations, individuals with a particular interest in mental health outcomes may have been more likely to participate; and as the study progressed, new participants were frequently referred by previous participants, who may have been motivated to refer like-minded individuals.
In addition, the vast disparity in avalanche rescue experience may have confounded the analysis; it seems inevitable that a first responder in the infancy of their rescue career would demonstrate profoundly different psychopathology to one who has worked on upwards of 50 avalanches over a period of 20 or more years, and as predicted, such differences were evident in the transcripts. In this regard, prior studies have yielded conflicting results when examining if professional responders with more years of service tend to experience greater or lesser degrees of posttraumatic, stress, and depressive symptoms (Brooks et al., 2016).
Finally, the very nature of the interviewer-subject relationship introduced limitations; the interviewer inevitably approached the study assuming that avalanche rescue is inherently psychologically straining and the interview questions were developed from that perspective—these inherent preconceptions introduced bias simply by influencing what questions were asked and the manner in which they were posed.
Future directions
In light of the aforementioned limitations, three directions for future work are suggested. First, larger studies may be helpful: as the pool of relevant and willing participants in Utah, Wyoming, and Colorado was effectively exhausted in the first round of interviews, either geographical scope should be broadened or the approach to subject recruitment should be augmented, possibly utilizing telephone outreach as a supplement to e-mail and social media. Second, future research could focus exclusively on professional first responders, considering that such individuals are both more likely to be recruited (as evidenced by this study) and more likely to experience additive psychopathology. Third, future subjects could be stratified according to the number of years they have worked in a first response role and number of avalanches they have participated in—both important themes in this initial study.
Of note, a revision of the interview format to include in-person interviews was considered, but ultimately deemed unhelpful—subjects were too geographically dispersed and often favored the relative anonymity of a telephone call.
Conclusions
As noted, our data suggest grounds for the following hypotheses: first, avalanche first response work is likely associated with significant psychiatric morbidity. Second, there is a paucity of psychological training and support among different backcountry rescue organizations, oftentimes consisting of ineffective after-action debriefs performed by individuals perceived to be underqualified. Finally, formal professional psychological support is generally positively received when available.
Future studies should seek to test the effectiveness of the aforementioned improvement recommendations pertaining to psychological preparation, postincident psychological support, and long-term psychological monitoring and maintenance for avalanche first responders.
Footnotes
Acknowledgments
We thank the scholarly projects program at Columbia University Vagelos College of Physicians and Surgeons for research time and financial support. We are indebted to the subjects of the study who shared their personal and often traumatic experiences with us.
Author Disclosure Statement
N.D. and C.T. conceptualized and designed the study; ND conducted, transcribed, and coded interviews; N.D. drafted the initial article; and C.T. edited and revised a final version. Neither of the authors has any relevant conflicts to disclose.