
Abstract
Abstract
Introduction:
Hypothermia and frostbite occur when there is a significant decrease in central and peripheral body temperature in individuals exposed to cold windy conditions, often at high altitude or in a mountain environment. Portable hyperbaric chambers increase the barometric pressure and thereby the partial pressure of oxygen inside the chamber, and their use is a well-known treatment for altitude illness. This study aims to show that a portable hyperbaric chamber could also be used to treat hypothermia and frostbite in the field, when rescue or descent is impossible or delayed.
Methods:
During a European research program (SOS-MAM, Flow Pulse study) measurements were taken from 27 healthy nonacclimatized voluntary subjects (21 men, 6 women, mean age 41 ± 17) at an altitude of 3800 m (Chamonix Mountain Lab, Aiguille du Midi, France) right before and immediately after spending 1 hour in a portable hyperbaric chamber at 300 mbar. We measured digital cutaneous temperature (Tcut), digital cutaneous blood flow (Fcut), digital tissue oxygenation (TcPO2), blood oxygen saturation (SpO2), heart rate, and core temperature. Air temperature inside the chamber (Tchamb) was measured throughout the whole session.
Results:
We observed significant increases in Tchamb: 9.3°C compared with the outside temperature, Tcut: +7.5°C (±6.2°C 71%), Fcut: +58PU (±89) (+379%), TcPO2: +18 mmHg (±11.9) (304%), and SpO2: 13%.
Conclusion:
This study shows that a portable hyperbaric chamber can be used to treat frostbite and/or hypothermia in the field at altitude when descent or rescue is impossible or even simply delayed.
Introduction
Frostbite is a freezing cold injury that occurs when tissues are exposed to temperatures below their freezing point for a sustained period of time (Gross and Moore, 2012). The main groups of people at risk of frostbite are winter sport recreationists (alpinists, skiers, and polar travelers), military personnel, and outdoor workers in cold environments. Nowadays, the availability and accessibility of high altitude sports has significantly increased the number of people participating in these activities irrespective of their level of expertise. The specific austerity of high altitude environments is a major complicating factor in expediting treatment for time-sensitive injures such as frostbite. Considering that to date, no treatment has been shown to positively affect the outcome of frostbite if administered three or more days after injury, the risk of amputation is dramatically increased in those injured on expeditions in remote locations.
The initial response to skin cooling is a peripheral vasoconstriction, a measure that protects core temperature (CT) and lessens heat loss through peripheral skin. To preserve the extremities during prolonged exposure to cold, a cold-induced vasodilation occurs (Lewis, 1941). However, as the skin cools further, there is constriction of the microvascular vessels and an increase in blood viscosity. Except for cases of very rapid freezing, initial crystal formation occurs in the extracellular space (Meryman, 1974). This creates an increase in osmotic pressure and draws free water across the cell membrane resulting in an intracellular water loss and hyperosmolarity. This process causes damage to the cell membranes and endothelium and ultimately results in cell death. If there is a long delay to treatment, the damage will be significant and in the worst cases, the frozen body part will require amputation.
Treatment of frostbite remains challenging for several reasons. First, assessing the severity of the injury in the field is necessary to define the appropriate treatment. Second, an accurate time of onset of injury must be established to guide subsequent steps and finally, the inevitable delay in providing treatment undoubtedly has a negative impact on outcome. As mentioned previously, if the initial treatment of frostbite is delayed beyond 24 hours, and definitive treatment for longer than 72 hours the risk of amputation remains high.
Standard recommendations for the initial emergency treatment of frostbite are as follows:
Rewarm the frozen part in a warm water bath at 37°C–39°C for 1 hour (Cauchy et al., 2016). Rehydrate the patient with warm drinks. Remove cold wet clothes and replace with warm dry clothes. If there are no contraindications, administer aspirin or ibuprofen for their antiprostaglandin and analgesic effects (Handford et al., 2014).
Once rewarming has been initiated, it is very important not to stop the process and to prevent refreezing. If frostbitten tissue refreezes, new ice crystals will form causing further mechanical damage to the affected tissues.
Following these first steps, there are medical treatments that can be offered if there is access to trained medical personnel. The early use of thrombolytic therapy and prostacyclin in hospital has shown a significant reduction in predicted amputation rates, but these medications are often unavailable, impractical to administer, or inappropriate for use in the field, and they require the presence of expert health care professionals and patient monitoring infrastructure.
Specifically, in the case of expeditions to high altitude, these treatment options would only be available if appropriately trained medical experts were present on the expedition. In most cases, there are no treatments beyond the basic first aid described above that would allow lay rescuers to limit tissue loss from frostbite when evacuation to an appropriate medical facility is delayed.
The presence of hypoxia at altitude further impairs oxygenation and reperfusion of frozen digits when patients are stuck in high altitude camps waiting for safe conditions to allow descent. Portable hyperbaric chambers have become a common device for expeditions to high altitude and are often part of a comprehensive medical kit. They have been shown to be effective in the treatment of altitude illness such as high altitude pulmonary edema and high altitude cerebral edema. The increased atmospheric pressure inside the chamber simulates descent to lower altitude when real descent is not possible (Bartsch et al., 1993) and the subsequent increase in partial pressure of arterial oxygen is what improves the symptoms of high altitude illness. Some of the amelioration in symptoms could be attributed to the improvement in vascular function at a higher atmospheric pressure within the chamber.
In frostbite cases, increasing the arterial partial pressure of oxygen and the partial pressure of oxygen within the tissue could improve thermogenesis and combat hypothermia (Frappell et al., 1998; Mortola, 2004; Madden and Morrison, 2005). Acute hypoxia tends to diminish the cold-induced vasodilation with marked impairment of hand rewarming; therefore, the portable recompression chamber could improve blood flow by reducing hypoxemia. The resulting increase in tissue oxygenation could increase basal metabolic rate while also producing peripheral vasodilation and increased temperature in the periphery (Daanen and van Ruiten, 2000; Keramidas et al., 2014). Moreover, the hyperbaric chamber offers protection from windchill and isolates patients from the ground. All of these factors could improve microvascular function and potentially limit the impact and severity of frostbite.
Our working hypothesis was that the use of a portable hyperbaric chamber can improve peripheral vascular flow, peripheral skin temperature, and peripheral skin oxygenation, thereby indirectly limiting the impact of frostbite.
Materials and Methods
Subjects
Twenty-seven healthy nonacclimatized volunteers recruited through an IFREMMONT newsletter participated in our European study (SOS-MAM, Flow Pulse study). Exclusion criteria included pregnancy, cigarette smoking, contraindications to high altitude, vasoactive treatment, hypertension, peripheral vascular disease, and coagulopathy. Characteristics of participants are summarized in Table 1.
Participant Characteristics
This protocol was approved by the Grenoble Ethics Committee (CPP Sud-Est V, Grenoble, France). All participants were informed of the potential risks and discomforts of taking part in the study.
Study design
The protocol took 4 hours per subject. Each participant joined the study at an altitude of 1000 m (Chamonix Mont Blanc) and went directly up to an altitude of 3800 m (Chamonix Mountain Lab, Aiguille du Midi, France) in a cable car. All subjects were similarly dressed in appropriate clothing.
After 20 minutes acclimatizing to the ambient temperature at that altitude, they were monitored for 15 minutes in a supine position, at rest in the open hyperbaric chamber, then for 60 minutes in the closed hyperbaric chamber, followed by a further 15 minutes with the chamber open again (Fig. 1).
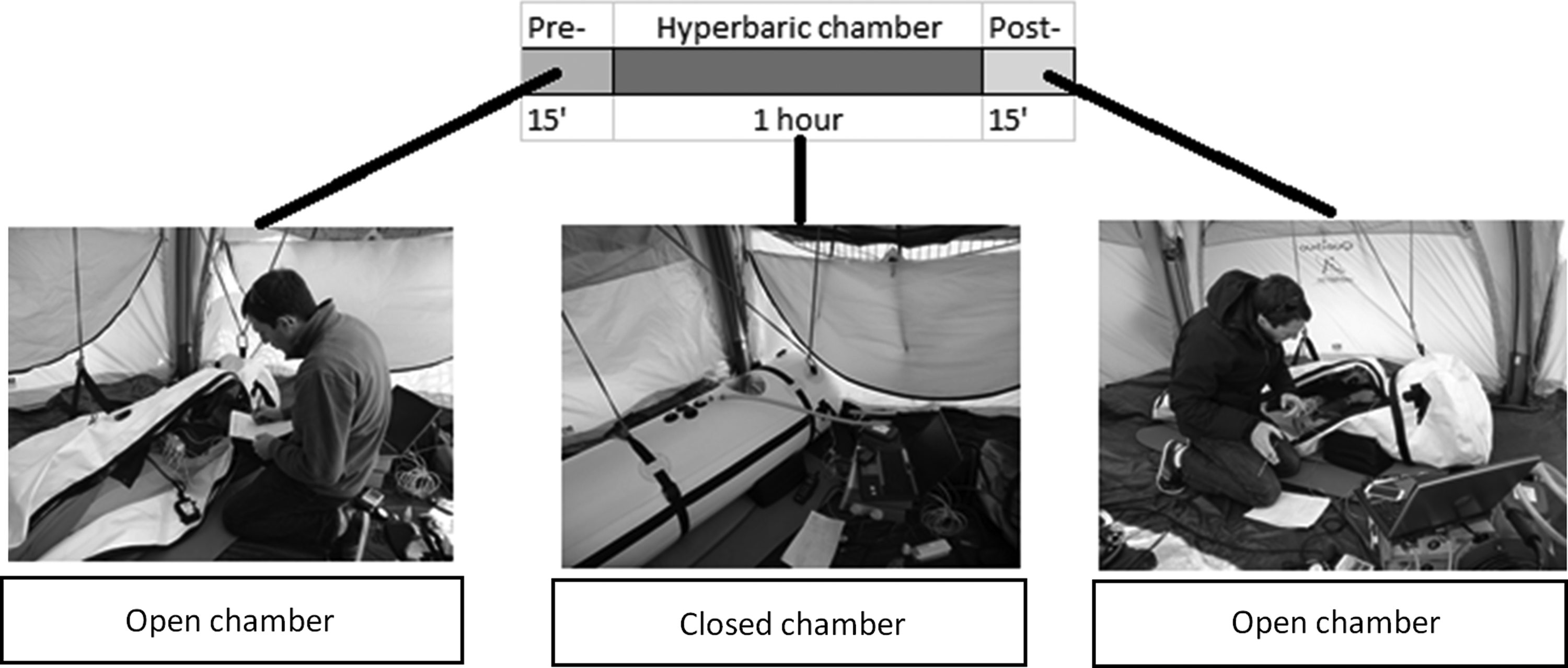
Study design.
Digital cutaneous temperature, digital microvascular flow (Laser Doppler Flow [LDF]), digital tissue oxygenation (TcPO2), heart rate (HR), CT, and blood oxygen saturation (SpO2) were recorded continuously throughout with the chamber in both the open and closed positions (Fig. 2).

Recording equipment.
Skin perfusion and cutaneous temperature were recorded on the palmar surface of the middle finger with an LDF (Periflux 5010) and temperature sensor (Periflux 5020), respectively. Tissue oxygenation was measured with a transient cutaneous pressure oxygen system (TcPO2; Periflux 5040) on the dorsal surface of the hand. CT and HR were recorded with a HR monitor on the chest wall (Zephyr) and the SpO2 was measured with a digital pulse oximeter (Nonin).
The hyperbaric chamber
We used a CERTEC portable hyperbaric chamber specially adapted for the purpose of this study. It was an emergency mountain rescue equipment previously used to treat patients with acute mountain sickness. The chamber is essentially an airtight container made of plastic material that is big enough for a person to be treated inside in a recumbent position. The pressure inside the chamber is increased using an electric pump, mimic the manual pump effect but easier for the experimental design, and the air inside is continuously replaced. This simple piece of equipment is able to simulate descent to a lower altitude by increasing the barometric pressure inside the chamber.
Data analysis
Data were digitalized, stored on a computer, and analyzed offline with signal processing software (Perisoft, Perimed, Järfälla, Sweden).
Statistical analysis
Data were reported as mean and standard deviation. We considered p values <0.05 to be significant. Statistical analysis was performed using package R-commander software (R-project software version 3.2.1).
Results
Air temperature (Fig. 3) was similar on different days (6.5°C ± 4.3°C, p > 0.05). All volunteers wore similar clothes (light high mountain pants and shirts). Ambient temperature inside the hyperbaric chamber increased by 9.3% during the time of increased pressure (inside 15.7°C ± 4.0°C vs. outside 6.5°C ± 4.3°C, p > 0.0001).
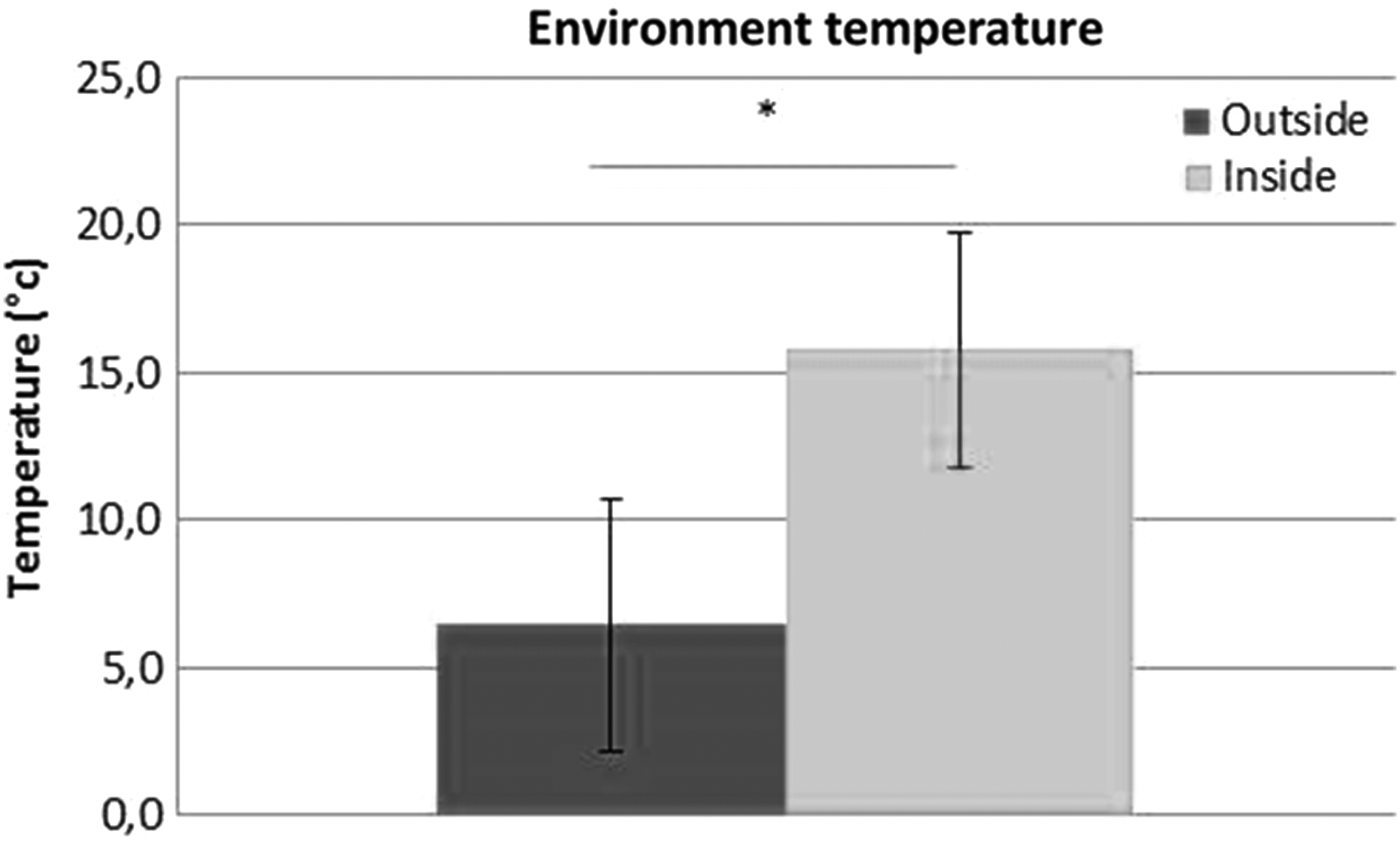
Temperature inside and outside of the hyperbaric chamber. *Indicates a significant difference between the two groups.
Digital skin temperature (Fig. 4A) was significantly higher during the pressurized phase (before 15°C ± 8°C vs. during 22°C ± 8°C, p < 0.0001). There was no difference in skin temperature with the chamber open before and after the period of increased pressure.
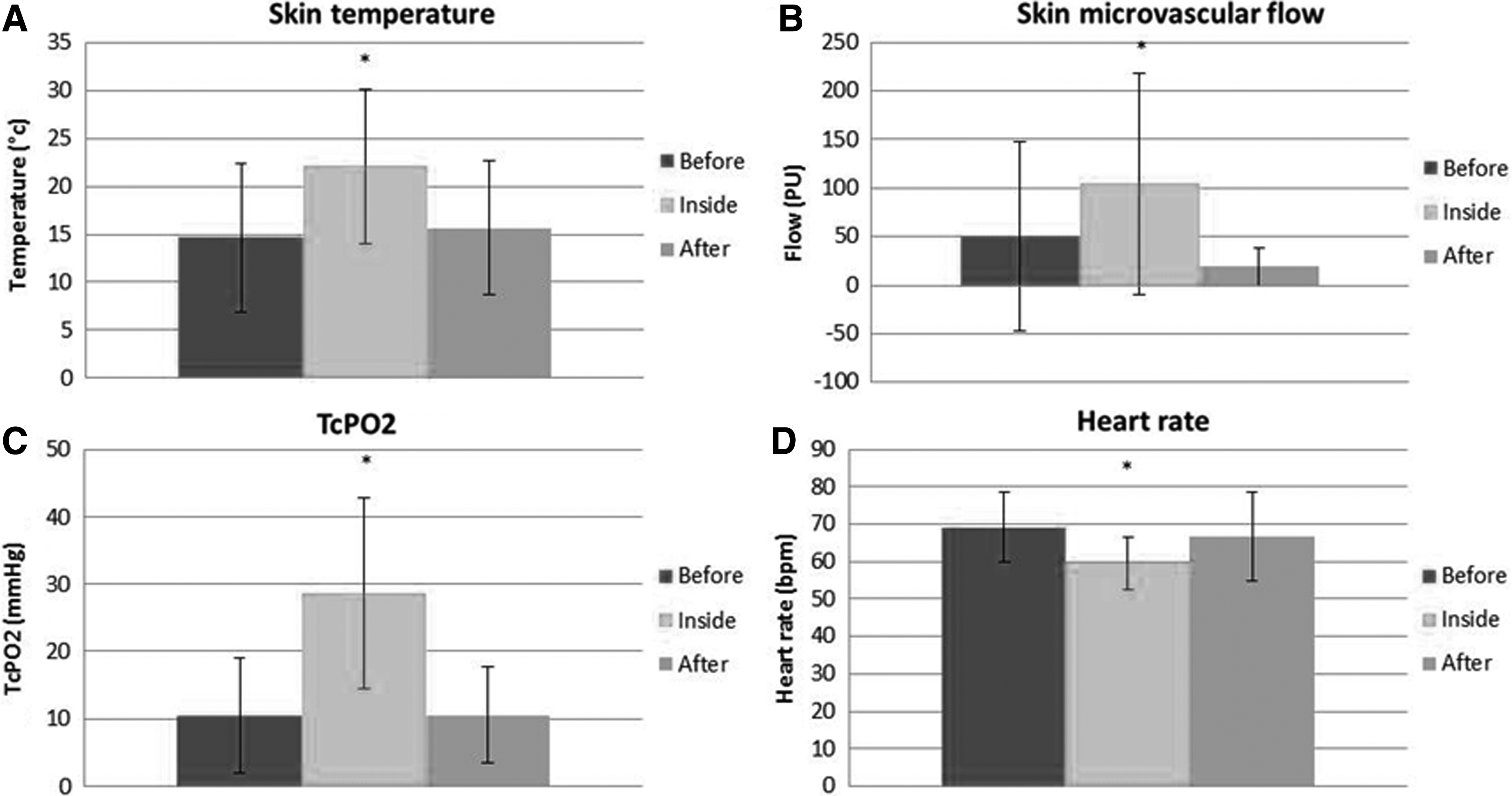
Skin microvascular flow (Fig. 4B) was significantly higher during the pressurized phase (before 50 ± 97 PU vs. during 104 ± 114 PU, p < 0.0001). There was no difference in flow with the chamber open before and after the period of increased pressure.
TcPO2 (Fig. 4C) was significantly higher during the pressurized phase (before 11 ± 8 mmHg vs. during 29 ± 14 mmHg, p < 0.0001). There was no difference in TcPO2 with the chamber open before and after the period of increased pressure.
SpO2 was significantly higher during the pressurized phase (before 85% ± 5% vs. during 98% ± 1%, p < 0.0001). The SpO2 was similar inside the chamber during the pressurized phase to the SpO2 at 1000 m altitude in Chamonix. There was no difference in SpO2 with the chamber open before and after the period of increased pressure.
HR (Fig. 4D) was significantly lower during the pressurized phase (before 69 ± 10 bpm vs. during 60 ± 7 bpm, p < 0.0001). There was no difference in HR with the chamber open before and after the period of increased pressure.
All of these adaptations disappeared when the hyperbaric chamber was opened after the period of increased pressure.
Discussion
Portable hyperbaric chambers are familiar pieces of equipment for high altitude mountaineering expeditions and the practice of mountain sports at altitude in general. However, their use in the treatment of frostbite has not yet been demonstrated to be beneficial although it had already been discussed as a possibility by our team (Cauchy et al., 2014).
Our results show a global improvement of skin microvascular function when subjects are inside the hyperbaric chamber at pressure compared with when they are at the ambient pressure at 3800 m, which could represent a first step in using a hyperbaric chamber in the treatment of frostbite in the field.
During the hyperbaric phase, the increase in the partial pressure of atmospheric oxygen facilitates oxygen uptake and improves oxygen saturation to 98%, the same as values in Chamonix town at an altitude of just 1000 m above sea level.
Higher SpO2 facilitates oxygen delivery to tissues and may improve endogenous thermogenesis by increasing mitochondrial activity. Moreover, a decrease in the hypoxic stress and associated sympathetic nervous system activation has a vasodilatory effect on the peripheral vascular system (Dana et al., 1969; Mathew et al., 1977; Daanen and van Ruiten, 2000). Our analyzed parameters showed an improvement in microvascular flow, TcPO2, and digital skin temperature. A general improvement in blood flow enabling more efficient heat and oxygen uptake and transfer in the whole body could explain what we observed. The decrease in HR during the pressurized phase can be interpreted as an appropriate response to improved oxygen transport and utilization with the demonstrated increase in SpO2. Furthermore, inside the closed hyperbaric chamber, individuals are protected from the wind and isolated from the ground canceling windchill and limiting heat loss by conduction. The combination of all of these features results in a higher ambient temperature inside the chamber, which in turn further improves microvascular function, limits hypoxic and cold stress, and enhances peripheral rewarming.
This pilot study into the effects of using a portable hyperbaric chamber on peripheral vascular function shows a global improvement in the parameters measured and suggests that there may be benefits in using a portable hyperbaric chamber to limit the extent and severity of injury due to frostbite in an austere and remote environment.
Footnotes
Acknowledgments
Special thanks to Mr. Buttin and Mr. Katz from Perimed France for the technical support. We also thank Mr. Stéphane Jaricot from CERTEC Enterprise.
Author Disclosure Statement
No competing financial interests exist.