
Abstract
Abstract
Background:
Because of the limited evidence available, recommendations for defibrillation of hypothermic patients vary among published guidelines.
Aim:
To report successful defibrillation of four severely hypothermic patients with witnessed cardiac arrest.
Results:
During a four-year period from 2014 to 2017, four of five hypothermic patients admitted to our institution with a history of sudden, unexpected ventricular fibrillation (core temperature: 24°C–27°C) were successfully defibrillated. Restoration of spontaneous circulation (ROSC) was possible after a single defibrillator shock (two patients) or during prolonged advanced life support cardiopulmonary resuscitation (two patients). Our patients and additional cases identified in the literature indicate that successful defibrillation is predominantly found in hypothermic patients with a core temperature above 24°C.
Conclusions:
Our data demonstrate that successful defibrillation and ROSC are possible in selected patients with severe accidental hypothermia and are perhaps more common than widely believed. These findings are of particular importance for mountain and wilderness rescue missions when transfer of an arrested patient to the nearest hospital providing extracorporeal rewarming is not possible. An automatic external defibrillator should be part of the medical equipment on any search or mountain rescue mission, in which the victim may have sustained accidental hypothermia.
Introduction
It is widely accepted that initial attempts at defibrillation may fail in hypothermic patients, although successful defibrillation will be possible later after rewarming (Vanden Hoeck et al., 2010; Brown et al., 2012; Truhlar et al., 2015; Paal et al., 2016). However, successful defibrillation has been described at a core temperature below 30°C (Walpoth et al., 1997; Clift and Munro-Davies, 2007; Paal et al., 2016). Few clinical or experimental data are available concerning the actual incidence of successful defibrillation during hypothermia or the number of defibrillation attempts that may be necessary and useful (Clift and Munro-Davies, 2007; Vanden Hoeck et al., 2010; Zafren et al., 2014; Truhlar et al., 2015). Consequently, recommendations for defibrillation of severely hypothermic patients differ among guidelines (Vanden Hoeck et al., Zafren et al., 2014; Truhlar et al., 2015).
We here report on four severely hypothermic patients with persistent restoration of spontaneous circulation (ROSC) following successful defibrillation.
Materials and Methods
The Medical University of Innsbruck is one of the regional study centers participating in the International Hypothermia Registry (IHR: www.hypothermia-registry.org), a prospective multicenter registry study collecting data on the treatment and outcome of patients with accidental hypothermia. The study has ethics committee approval.
For patient recruitment, all trauma emergency room admissions are screened for patients with accidental hypothermia and a core temperature below 30°C. Hypothermic patients after accidents and those after emergencies in mountainous terrain are all admitted to the trauma emergency room. Patients after urban hypothermia are admitted to the trauma emergency room only when extracorporeal life support (ECLS) is considered necessary (e.g., cardiac arrest or severe hemodynamic instability).
Results
A review of trauma emergency room admissions between January 1, 2014, and December 31, 2017, revealed 27 severely hypothermic patients with a core temperature below 30°C. Seventeen of these 27 patients had a history of prehospital cardiac arrest and in five of them cardiac arrest was witnessed (Fig. 1).
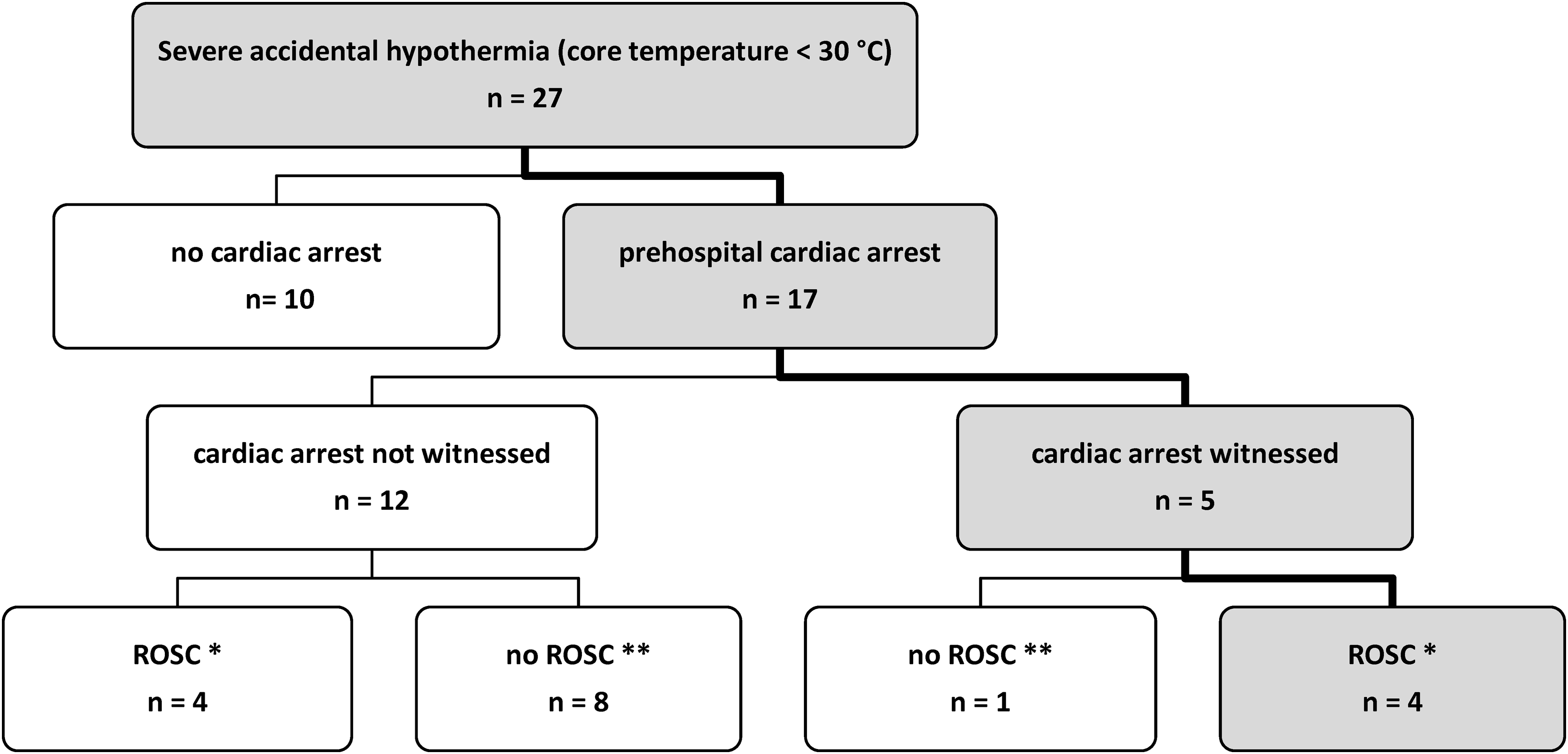
Characteristics of hypothermic patients admitted to the trauma emergency room (n = 27). *Restoration of spontaneous circulation on admission to the trauma emergency room. **Ongoing CPR on admission to the trauma emergency room. All nine patients were rewarmed and resuscitated with an extracorporeal life support system; the patient with witnessed cardiac arrest survived with full neurological recovery. CPR, cardiopulmonary resuscitation.
Four of these five patients had persistent ROSC after successful defibrillation (Table 1).
Characteristics of Hypothermic Patients with Witnessed Cardiac Arrest and Successful Defibrillation (n = 4)
Active external or internal rewarming without extracorporeal circulation applied before successful defibrillation.
Core temperature when defibrillator shock was successful.
Thermistor-based epitympanic temperature.
ROSC, restoration of spontaneous circulation; ER, emergency room; PH, prehospital.
Cases of successful defibrillation
Patient 1 was a 25-year-old male skier extricated after 20 minutes of complete burial by an avalanche. Basic life support cardiopulmonary resuscitation (BLS CPR) was immediately started. ROSC was achieved on site after advanced life support cardiopulmonary resuscitation (ALS CPR) and administration of 3 mg of intravenous epinephrine by the crew of an emergency medical services helicopter crew. Forty minutes later, the patient arrived at Innsbruck Medical University Hospital. On admission, the patient was in a deep coma with a heart rate in the range of 90 beats/min and a systolic blood pressure of 110 mmHg. Thermistor-based epitympanic temperature on arrival in the emergency department was 25.6°C.
When the patient was removed from the helicopter rescue bag, sudden ventricular fibrillation occurred. Manual chest compression was started immediately while defibrillator patches were being applied. A single shock (200 J) within 1 minute restored a perfusing rhythm with a systolic blood pressure of 120 mmHg. Active external rewarming using forced air was started immediately. The patient was successfully rewarmed to 36°C within 5 hours without any further episodes of ventricular fibrillation. The patient eventually died from hypoxic multi-organ system failure due to snow burial.
Patient 2 was a 25-year-old alcohol-intoxicated male who spent a cold winter night outside. When a physician-staffed emergency medical helicopter arrived at the scene the next morning, he was unconscious (Glasgow Coma Scale [GCS] 7), breathing spontaneously (respiratory rate 10) with palpable central pulses. Electrocardiography (ECG) demonstrated narrow complex tachycardia and a heart rate of 100–120 beats/min. Core temperature by epitympanic thermometer (thermistor probe) was 25°C. During transfer to a nearby hospital, the patient developed sudden bradycardia with loss of pulses and external chest compression was started. On admission to hospital a few minutes later, the patient was in ventricular fibrillation. After 20 minutes of ALS CPR including epinephrine 5 mg and amiodarone 300 mg, the third defibrillator shock restored spontaneous circulation.
The patient was transferred to Innsbruck Medical University Hospital for further treatment. During helicopter transfer, two further episodes of ventricular fibrillation occurred, both immediately responding to a single defibrillator shock. On arrival at Innsbruck Medical University Hospital, the patient had a heart rate of about 40 beats/min and a mean arterial pressure of 50 mmHg. Bladder temperature was 24.6°C. The patient was rewarmed using a forced air device with an ECLS system on standby. The patient was successfully rewarmed noninvasively in 8 hours. He made a full recovery and left the hospital a few days later.
Patient 3 was a 57-year-old female, who was missing for several hours on a cold November evening. She was eventually found lying partially immersed in a small creek. This unconscious woman, who was breathing normally, was evacuated by the Mountain Rescue Service and handed over to a physician-staffed ambulance unit about 1 hour later. The patient was in a deep coma (GCS 5 points) with a normal respiratory rate. ECG demonstrated bradycardia with a heart rate about 40 beats/min; blood pressure could not be obtained. Thermistor-based epitympanic temperature was 26°C. Peripheral venous access was established and endotracheal intubation was performed. After endotracheal intubation, ventricular fibrillation suddenly occurred. This was converted to a stable bradycardic rhythm with a single, immediate defibrillator shock; no blood pressure could be obtained. External chest compressions were started, and the patient was transferred to Innsbruck Medical University Hospital.
On arrival in the emergency department, she was mechanically ventilated and in a deep coma (GCS 3) with fixed dilated pupils. She had wide complex bradycardia at 45 beats/min on cardiac monitor. Femoral pulses were palpable on admission, and therefore, external chest compression was discontinued. A femoral arterial line was placed and showed a systolic blood pressure of 60 mmHg. Bladder temperature was 26.8°C. The patient was transferred to the operating room for ECLS placement despite persistent ROSC. Successful extracorporeal rewarming was followed by a prolonged stay in the intensive care unit. The patient survived with full neurological recovery.
Patient 4 was a 40-year-old male, who sustained a severe brain trauma in an avalanche accident. When the emergency physician arrived at the scene, he found a spontaneously breathing, unconscious patient (GCS 6) with palpable central pulses, and a huge open skull fracture. After volume resuscitation and drug-assisted endotracheal intubation, the patient was evacuated to a nearby hospital by helicopter. Shortly before landing at the hospital, ECG monitoring demonstrated sudden onset of ventricular fibrillation. A single defibrillator shock restored a supraventricular tachycardia with a palpable pulse. After admission to the emergency department a few minutes later, thermistor-based epitympanic temperature was 27°C. External rewarming started.
The patient was immediately transferred to Innsbruck Medical University Hospital. A cerebral computed tomography scan obtained after admission demonstrated irreversible traumatic cerebral injury; 24 hours later, brain death was confirmed.
Discussion
Our data suggest that successful defibrillation and ROSC are possible in selected patients with severe accidental hypothermia and are perhaps more common than widely believed. We must, however, point out that this small case series includes only patients with witnessed cardiac arrest, immediate professional CPR, and early attempts at defibrillation. None of the patients had a core temperature below 24°C.
In addition to publications mentioning successful defibrillation without providing further details (Kornberger et al., 1999; Vassal et al., 2001; Darocha et al., 2014; Ruttmann et al., 2017), a nonsystematic review of the literature yielded 11 reports (Dominguez et al., 1973; Nordrehaug, 1982; Baumgartner et al., 1992; Kuester-Kaufmann et al., 1996; Koller et al., 1997; Irone et al., 1998; Thomas and Cahill, 2000; Alfonzo et al., 2009; Lee et al., 2009; Masaki et al., 2009; Marimuthu et al., 2013) describing in more detail the circumstances associated with successful defibrillation in severely hypothermic patients not supported by extracorporeal circulation (Table 2). This nonsystematic review included a PubMed search using the terms “accidental hypothermia and defibrillation” and “accidental hypothermia and restoration of spontaneous circulation” as well as a hand search of guidelines, review articles, and case series published in peer-reviewed journals. Publications for hand search were selected based on the scientific and clinical experience of the authors in the field of accidental hypothermia.
Characteristics of Hypothermic Patients with Successful Defibrillation Reported in the Literature (n = 11)
Active external or internal rewarming without extracorporeal circulation applied before successful defibrillation.
Core temperature when successful defibrillator shock was applied.
Nasopharyngeal temperature.
Rectal temperature.
Esophageal temperature.
ALS CPR, advanced life support cardiopulmonary resuscitation; ECC, extracorporeal circulation; M, male; F, female; OR, operating room; ICU, intensive care unit; VT, ventricular tachycardia.
Successful defibrillation was reported after prolonged exposure to cold as well as after drowning. Defibrillation was successful not only after a single shock but also after repeated defibrillation attempts during prolonged ALS CPR. Our literature review also yielded two reports of “chemical defibrillation” after bretylium administration (Danzl et al., 1982; Kochar et al., 1986) and reports of spontaneous termination of ventricular fibrillation in hypothermic patients during prolonged ALS CPR (DaVee Reineberg, 1980; De Caen, 2002; Claret et al., 2013). Remarkably, two of the three patients with spontaneous termination of ventricular fibrillation had a core temperature <20°C. Successful defibrillation was possible with a core temperature as low as 22°C, but as in our experience, more than 90% of patients reported in the literature had a core temperature above 24°C (Table 2). Furthermore, in a report of 23 profoundly hypothermic patients (all with a core temperature ≤24°C), none of the 7 patients with witnessed ventricular fibrillation were able to be defibrillated successfully before extracorporeal rewarming (Pasquier et al., 2014). Available data suggest that a core temperature above 24°C could be a parameter associated with successful defibrillation in severely hypothermic patients.
During the four-year period we reviewed, four of the five hypothermic patients with a history of witnessed cardiac arrest were successfully defibrillated. Our experience with this small number of patients suggests that a large portion of hypothermic patients may be successfully defibrillated. Our experience most likely overestimates the success rate, considering the large number of published hypothermia cases needing extracorporeal support because of persistent ventricular fibrillation. However, a publication bias toward cases surviving very prolonged periods of resuscitation and cases needing extracorporeal support is likely.
Only limited clinical or experimental data are available to estimate more precisely the actual incidence of successful defibrillation in patients with hypothermic cardiac arrest. As in our experience, Darocha et al. (2014) reported ROSC in two hypothermic patients who sustained sudden ventricular fibrillation during transfer to the Krakow Accidental Hypothermia Center. Experimental animal studies repeatedly report successful defibrillation in about 50% of animals despite a core temperature ≤26°C (Elenbaas et al., 1984; Gillen et al., 1986; Murphy et al., 1986). However, these animal data also indicate that defibrillation in prolonged untreated cardiac arrest often results in pulseless electrical activity (Elenbaas et al., 1984) or only transient ROSC (Krismer et al., 2000).
Furthermore, successful defibrillation at a core temperature below 28°C is often seen in patients with extracorporeal circulatory support and optimized myocardial perfusion (Walpoth et al., 1997; Clift and Munro-Davies, 2007; Paal et al., 2016). Recently published experimental animal data (Piktel et al., 2017) further support the theory that myocardial ischemia may aggravate hypothermia-associated irritability of the heart. To improve myocardial perfusion pressure by administering vasopressor drugs during external chest compression may be one option for increasing defibrillation success during hypothermic CPR (Schwarz et al., 2002).
There is some evidence that defibrillation can be successful in some cases of hypothermia-associated cardiac arrest. Consequently, an automatic external defibrillator (AED) should be part of the medical equipment on any search or mountain rescue mission when victims may have sustained accidental hypothermia. ROSC at the scene is of utmost importance in these missions, as transfer of an arrested hypothermic patient to ECLS with continuous CPR or within a reasonable period of time is often impossible. A recent survey among mountain rescue services showed that AEDs were available in about two-thirds of the services (Podsiadlo et al., 2017). The use of AEDs to diagnose and treat hypothermic cardiac arrest in the prehospital environment has been reported (Claret et al., 2013; Boue et al., 2014).
If three attempts at defibrillation fail, current European Resuscitation Council guidelines (Truhlar et al., 2015) recommend avoiding further shocks at the scene and immediate transfer of the patient to the nearest hospital providing ECLS. As patient transfer with continuous external chest compression may be impossible during many mountain and wilderness rescue missions, the use of intermittent CPR has been recommended for this scenario (Gordon et al., 2015). This recommendation is based on experience obtained during cardiothoracic surgery and a few isolated case reports (Oberhammer et al., 2008; Boue et al., 2014). Our data suggest that a period of advanced life support CPR at the scene may be a reasonable alternative. However, resuscitation efforts at the scene should never delay patient transfer to ECLS when transfer time is reasonably short and continuous external chest compressions are guaranteed (Vanden Hoeck et al., 2010; Brown et al., 2012; Truhlar et al., 2015; Paal et al., 2016).
Mechanical chest compression devices are an option to provide continuous high-quality external chest compression during technical rescue (Putzer et al., 2013) or helicopter evacuation (Rauch et al., 2018). Mechanical chest compression devices can therefore enable patient transfer to the next ECLS center even in difficult rescue scenarios.
There is evidence that a moderate increase in core temperature during active rewarming may improve defibrillation success (DaVee and Reineberg, 1980; DeCaen, 2002; Clift and Munro-Davies, 2007; Zafren et al., 2014). About one-third of all cases of successful defibrillation reported in the literature underwent active rewarming before defibrillator shocks were able to restore spontaneous circulation (Table 2). Therefore, active rewarming should be started as early as possible when transfer to extracorporeal circulation is not an option.
Conclusions
Our experience and data from the literature suggest that the success rate of defibrillation attempts may be higher than widely assumed in hypothermic patients with ventricular fibrillation and a core temperature above 24°C. This finding is of particular importance for mountain and wilderness rescue when immediate transfer of a hypothermic patient to a hospital providing ECLS is not possible.
Footnotes
Author Disclosure Statement
None of the authors has any financial or personal relationship that could have inappropriately influenced the work.