
Abstract
Abstract
We compared the decrease in maximal heart rate (HRmax) from normoxia to normobaric (NH) and hypobaric (HH) hypoxia, respectively, in trained and untrained subjects (n = 187). HRmax data in normoxia and NH (n = 55) or HH (n = 26) were collected from 81 publications. No study directly compared HRmax in NH and HH. Concomitant arterial oxygen saturation (SaO2) and HRmax data were found in 60 studies. Overall, the results showed that the higher the desaturation, the greater the decrease in HRmax. Since desaturation appeared to be slightly higher during HH versus NH and was higher in trained than in untrained subjects, the decrease in HRmax tended (p = 0.07) to be higher in trained subjects in HH than in NH (e.g., −12.7 bpm vs. −8.6 bpm at 4000 m), whereas in untrained subjects the difference was negligible (−9.9 bpm vs. −8.3 bpm). To conclude, when compared with normoxia, the decrease in HRmax was slightly higher in HH than in NH in trained subjects. However, this result has to be confirmed and from a practical point of view, one may question the significance of this difference as well as the relevance of using different HR values for prescribing training intensity during exercise performed in NH or in HH.
Introduction
Normobaric hypoxia (NH), corresponding to reduction of the inspired fraction of oxygen (FiO2) <20.93%, can be used instead of the natural and terrestrial altitude, so-called hypobaric hypoxia [HH, e.g., a lower barometric pressure (PB) inducing a lower oxygen partial pressure, PO2]. For long, it was thought that only PO2 was determining the (patho)-physiological responses of individuals, whatever PO2 <150 mmHg was caused by decreased FiO2 (NH) or decreased PB (HH). This paradigm called the “Equivalent Air Altitude” model was questioned first by space physiologists such as Conkin (Conkin and Wessel, 2008) and then by respiratory physiologists (Savourey et al., 2003).
It is now well established that “NH is not a surrogate to HH” (Conkin, 2016). Several physiological differences such as minute ventilation (Savourey et al., 2003), fluid balance (Loeppky et al., 2005), or oxidative stress markers (Faiss et al., 2013; Debevec et al., 2015; Ribon et al., 2015) have been reported between NH and HH exposure (Millet et al., 2012; Richard and Koehle, 2012). Sleep disturbances have also been reported higher in HH than in NH (Heinzer et al., 2016; Saugy et al., 2016b). Moreover, the contribution of PH2O is different between NH and HH (Conkin, 2011) and at least PIO2 should be matched for relevant comparison. However, even if this is done, the hypoxic stimulus appears more severe in HH than in NH for the same ambient PO2 (Conkin, 2016). So, not surprisingly, acute mountain sickness symptoms have been shown to be more severe in HH than in NH (Roach et al., 1996; Loeppky et al., 2005). Taken together, these differences suggest different physiological responses to hypoxic exposure in “simulated” (NH) versus “real” altitude (HH).
It is well known that altitude-induced decrement in performance or related parameters such as VO2max is larger in trained athletes than in their less trained counterparts (Lawler et al., 1988; Koistinen et al., 1995; Mollard et al., 2007a; Faiss et al., 2014). The influence of arterial oxygen saturation (SaO2) is also well established, that is, the lower the SaO2 level the larger the performance decrement (Gavin et al., 1998; Chapman et al., 1999; Mollard et al., 2007a). For example, Mollard et al. (2007a) reported a larger decrement of VO2max in trained triathletes than in untrained subjects at a simulated altitude of 3500 m. In that study, the drop in SaO2 was a strong predictor of the VO2max decrement in hypoxia.
A relative hypoventilation (i.e., lower increase of ventilation) in response to hypoxia might explain partly the higher sensitivity observed in trained athletes (Mollard et al., 2007a, b). However, the influence of exercise-induced hypoxemia (i.e., a higher limitation of O2 diffusion in pulmonary capillaries when cardiac output is near maximal) is likely the main determinant of the higher decrease in SaO2 during maximal exercise at altitude in trained than untrained athletes (Robergs et al., 1998; Chapman et al., 1999, 2011).
When comparing the SaO2, there are several reports that HH leads to a lower level than NH at rest (Savourey et al., 2003, 2007; Saugy et al., 2016c) or during maximal exercise (Saugy et al., 2016a). However, based on a review of 13 studies, (Coppel et al., 2015), the differences in SaO2 remain unclear.
There are many clinical applications of hypoxic exposure/training aiming for performance enhancement in endurance (Millet et al., 2010) or team sports athletes (Brocherie et al., 2017) as well as for therapeutic purposes (Millet et al., 2016). The prescription of exercise intensity is often based on percentage of maximal heart rate (HRmax) or HR reserve. Recently, a literature review (Mourot, 2018) based on 86 studies confirmed that HRmax declined with altitude and suggested that the main mechanism was the reduction in SaO2. This author showed also that the HRmax decrease was larger in trained than in sedentary subjects. Despite the development of NH devices for performance and medical purposes and despite that exercise intensity is often based on %HRmax, it is of interest to compare if HRmax is similar between NH and HH. However, to our knowledge, there is no review comparing HRmax in HH versus NH.
Therefore, the aim of the present review was to test the two following hypotheses: (1) HRmax is lower in HH than in NH and (2) the difference is more important in trained athletes than in sedentary subjects. These assumptions were based on the facts that the decrement in HRmax seems to be influenced by the desaturation level; that this desaturation is generally larger in trained than untrained subjects; and that HH represents a more severe hypoxic stimulus than NH.
Methods
A literature search was made up until July 2018 using PubMed, ScienceDirect, Scopus, SPORTDiscus, and Web of Science databases. Search terms were used to restrict studies to those involving healthy humans under hypoxic conditions, including a combination of either “altitude” or “hypoxia” or “oxygen fraction” or “oxygen delivery” and each of the following: “exercise,” “exercise training,” “Live Low-Train High,” “intermittent hypoxia,” “incremental,” “GXT,” “graded,” “heart rate,” “exhaustion.”
The published studies were assessed for relevance to the topic and selected if they met the following inclusion criteria: involving humans; normoxia and hypobaric or NH conditions; hypoxic level expressed as altitude (m); and/or inspired oxygen fraction (%). The articles reporting HRmax in normobaric and HH and normoxia were selected.
To do so, the common criteria to assess that maximal intensity was reached at the end of the incremental test to exhaustion were considered (Howley et al., 1995) except for older ones within which the author's statement of “maximal intensity” was deemed adequate. Also, only acute exposure to hypoxia, that is, the maximal test should have been performed within 8 hours of exposure to the hypoxic environment, was taken into consideration. References of articles that fulfilled the criteria were also scanned for further relevant studies that were included if they met the inclusion criteria. To divide the participants into trained or untrained groups, we followed the author's statement of training status. In five of the reviewed articles, the data were not reported in the text/tables but in figures. In these cases, the data were extracted using the Digitizelt software (v2.2; BormiSoft2, Braunschweig, Germany).
Due to the important lack of standardization of study designs (the most important of which being the hypoxic stimulus, and also how the training status was determined), it was not possible to systematically analyze the effects of the different hypoxic interventions. However, analyses of covariance were used to compare the slopes of the linear relationships found between altitude gain and the decrement in HRmax and between altitude gain and the decrement in SaO2 (Microsoft Excel 2010; Microsoft Corporation, Redmond, Washington).
Results and Discussion
HRmax data in normoxia and normobaric and/or HH were collected from 172 different groups of participants reported in 81 publications (26 in HH and 55 in NH). Concomitant SaO2 and HRmax data were found in 60 studies (15 in HH and 45 in NH). As depicted in Figure 1, the results obtained confirmed the decrement in HRmax with altitude gain, the higher the altitude gain the greater the decrease in HRmax (y = −0.0025x + 1.2977; r2 = 0.37) (Mourot, 2018). The slope of the decrement in HRmax with altitude gain was not different (p = 0.86) in trained (n = 69; y = −0.0026x + 1.2486; r2 = 0.45) versus untrained (n = 103; y = −0.0025x + 1.4263; r2 = 0.33) participants. Also, the decrement was nonsignificantly different (p = 0.25) in HH (n = 50; y = −0.0036x + 3.4964, r2 = 0.56) versus NH (n = 122; y = −0.002x – 0.2103; r2 = 0.26).

Decrement in maximal heart rate (bpm) during normobaric (NH) or hypobaric (HH) hypoxia expressed as altitude gain (m). Effect of training status. Each single point represents group average results in a published study.
As depicted in Figure 1, subgroup analyses showed that in both HH and NH, trained subjects have nonsignificantly (p = 0.09 and p = 0.37) higher decrement in HRmax with altitude compared with untrained subjects. The decrement tended to be higher in HH versus NH in trained (p = 0.07) but not in untrained (p = 0.82) subjects. The results obtained from 132 different groups of participants confirmed the decrement in saturation at maximal intensity with altitude gain (y = −0.0054x + 1.3372; r2 = 0.67). As for HRmax, the slope of desaturation with altitude was not different (p = 0.11) during HH (n = 31; y = −0.0049x–1.1464; r2 = 0.78) than in NH (n = 100; y = −0.0058x + 3.0242; r2 = 0.65). It was significantly higher (p < 0.001) in trained (n = 118; y = −0.0057x + 0.5595; r2 = 0.78) than in untrained (n = 142; y = −0.0053x + 2.2172; r2 = 0.76) participants.
Finally, our results showed that the higher the desaturation the greater the decrease in HRmax (Fig. 2), as already reported (Mourot, 2018). These results are in line with the existing literature (Chapman et al., 1999, 2011; Mollard et al., 2007a) and a consequence of the exercise-induced hypoxemia reported in endurance- trained athletes. The present results confirm also that slight differences exist between NH and HH and that they cannot be used interchangeably (Fulco et al., 2011; Saugy et al., 2014; Coppel et al., 2015; DiPasquale et al., 2015b).
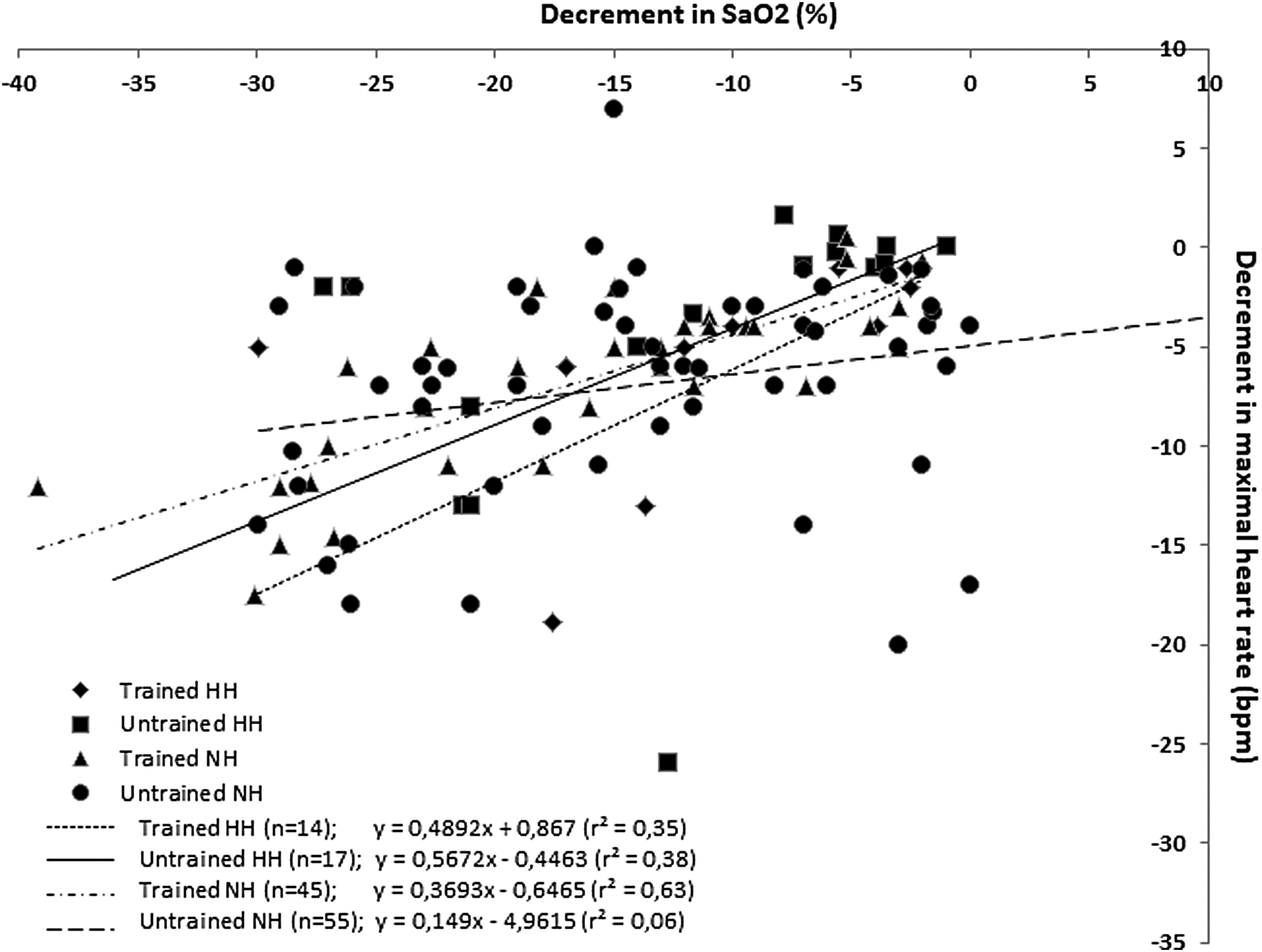
Decrement in maximal heart rate (bpm) as a function of arterial oxygen saturation (SaO2, %) during normobaric (NH) or hypobaric (HH) hypoxia. Effect of training status. Each single point represents group average results in a published study.
However, a better evaluation of the effect of NH and HH on HRmax using adequate research design is mandatory. Indeed, a direct comparison of the effects of NH versus HH on the decrement of HRmax has not been performed yet. The ability of a subject to reach HRmax is affected by numerous factors, including (but not limited to) age, testing modalities, training status, or duration of exposure to the hypoxic stimulus before testing. These factors were controlled in the studies comparing HRmax decrement in normoxia versus NH or versus HH. However, no study directly compared the decrement of HRmax in the two environments and it was not possible to systematically analyze the effect of NH versus HH due to important lack of standardization of study design. Further studies are thus mandatory with appropriate design, including proper control of the placebo effect that is known for having a major effect in such a context (Lundby et al., 2012).
Nevertheless, we observed that as a consequence of the slightly larger decrease in SaO2 in trained subjects when exposed to HH, the decrease in HRmax tended to be higher in this group in HH than in NH. As an example, at an altitude of 4000 m, the decrease in HRmax from normoxia to NH or HH, respectively, would be −8.6 and −12.7 bpm in trained subjects and −8.3 and −9.9 bpm in untrained subjects. The difference between NH and HH is 4.1 and 1.6 bpm for trained and untrained subjects, respectively. This difference (<2 bpm) seems negligible in untrained subjects and only a moderate source of error (<4 bpm) for training intensity prescription in trained subjects. Let us take an example of a cyclist performing intermittent hypoxic training at 80% HRmax ( = 200 bpm in normoxia) (Roels et al., 2005). This corresponds to 82.5% and 83.8% of his HRmax in NH and HH, respectively.
Altogether, from a practical point of view, one may question if there is a need for adapting intensity prescription based on HR for exercise performed either in NH or in HH. In contrast, if based on wattage, there is a need for lowering the intensity in HH when compared with NH, since the difference in power output between NH and HH has been shown to be significant (Saugy et al., 2016a).
Conclusion
The present study adds elements to the expending body of evidences stating that NH and HH cannot be used interchangeably (Fulco et al., 2011; Millet et al., 2012; Saugy et al., 2014; Coppel et al., 2015; DiPasquale et al., 2015a, b). When compared with normoxia, the HRmax decrease was slightly lower in NH than in HH (up to 4 bpm difference) in trained subjects—and likely even more in elite endurance athletes. However, although a given %HRmax would correspond to a slightly lower relative intensity in NH than in HH, one may question the practical significance to use different HR values for prescribing training intensity during exercise performed in NH or in HH.
Footnotes
Author Disclosure Statement
No competing financial interests exist.