
Abstract
Abstract
Background:
Sickle cell trait (SCT) is a common genetic abnormality in the so-called “sickle belts” in India. Splenic infarction often brings to medical attention an underlying SCT, when appropriately looked for. The hypoxic environment of an extreme high-altitude area (HAA) is conducive for developing a splenic infarct in an SCT individual not a native of these areas.
Aims:
We studied retrospectively 27 cases who presented with a splenic infarction during the last 4 years.
Results:
Twenty-five patients (92.5%) were diagnosed to have SCT, and 85% patients had developed splenic infarct on exposure to very HAAs. Clinically, splenomegaly was seen in 33% of patients with splenic infarct at presentation. The mean hemoglobin S was 36.92% in SCT individuals. A thrombus in the splenoportal axis was demonstrated in 22.2% of cases. Splenic rupture was a rare event, seen in only 3.5% of patients. Splenectomy was not required in any of the cases. Splenic abscess was not seen, and antibiotics were not required in any of the cases. We discuss the profile and management of these patients and review the literature on splenic infarction in HAA.
Conclusion:
SCT is commonly overlooked cause of splenic infarction and conservative management is effective in most of the cases. Splenectomy is required only in the rarest of rare cases. The profile and management of these patients and a review of the literature on splenic infarction in HAA has been discussed.
Introduction
Sickle cell trait (SCT) occurs due to the heterozygous glutamic acid-to-valine substitution in the beta-globin gene on chromosome 11 (HbAS). Worldwide, an estimated 300 million individuals carry this gene (Key and Derebail, 2010). The sickle gene evolved in the areas with high Plasmodium falciparum transmission as a defense against mortality by reducing parasitemia (Allison, 1954; Williams et al., 2005). In India, an estimated 13.1% of the population carry this gene, mostly in the so-called “sickle belts” (Kar, 1991). Patients are usually unaware of their condition unless they have a family history. SCT, although not a true disease entity, is a risk factor for certain adverse outcomes resulting from a complex interplay of genetic and environmental influences.
Splenic infarct, also known as the splenic syndrome, has diverse etiologies with thromboembolism and infections being the most common (Vijayaraghavan and Thomas, 2016). Splenic infarction has been commonly reported in SCT individuals in various hypoxic situations, such as ascent to high-altitude areas (HAAs) and flying in unpressurised aircrafts (Conn, 1954; Sheikha, 2005). Although SCT is common in many populations, the occurrence of splenic infarct on exposure to a high altitude has been restricted to case reports or small case series (Nussbaum and Rice, 1984; Goldberg et al., 1985; Lane and Githens, 1985; Steinberg, 1985; Shalev et al., 1988; Kopp et al., 1989; Tiernan, 1999; Goodman et al. 2014; Hota and Singh, 2015). Military soldiers are one group that gets exposed to very high altitudes for prolonged periods of time. Velu Nair et al. have earlier reported 5 cases of splenic infarct from our institution, in their study on 24 cases with various thrombotic complications in military soldiers at very high altitudes (Nair et al., 2006). In the absence of any national policy on the universal screening of newborns for hemoglobinopathies, SCT, an otherwise benign entity, often comes to light due to increased sickling in the setting of hypoxia, leading to splenic infarct.
Splenectomy, although unnecessary, is sometimes resorted to when it presents as acute abdomen, and SCT is not thought of as the underlying cause (Sheikha, 2005). We studied the case records in our hospital of all patients referred with splenic infarcts during the last 4 years. We identified 27 patients who were referred with a diagnosis of splenic infarct to our hematology center. We present an extensive clinical evaluation of these cases and review the existing literature.
Patients and Methods
In this retrospective observational study, young healthy soldiers, with no significant past history, referred to a tertiary care hematology center with splenic infarction were studied from January 2012 to June 2016. Diagnosis was confirmed with abdominal ultrasonography (USG) when patients presented to the peripheral hospital with acute abdomen. Patients were included in the study if they had undergone evaluation with USG abdomen and abdominal doppler and/or computed tomography (CT) angiographic studies for the confirmation of a splenic infarct and evaluation of splenoportal axis, hemoglobin high-performance liquid chromatography (Hb HPLC), and appropriate thrombophilia workup if Hb HPLC was negative for SCT. Risk factors and clinical symptoms were assessed. The follow-up of the patients for a period of at least 6 months was required to be included in the study.
Results
During the period from January 2012 to June 2016, 27 adult males were referred to our tertiary care hematology center with a possible diagnosis of splenic infarction. The clinical and investigation profile of the patients is presented in Table 1. The median age was 30 years, and all were males. Out of 27 patients, 23 (85%) reported splenic infarction from an HAA with a mean altitude of 12,700 ft above the sea level; 14.8% (n = 4) had developed splenic infarcts in plain areas, of which 3 patients (11.1%) after strenuous physical exertion and 1 (3.7%) during a short febrile episode. On evaluation, 92.5% patients (n = 25) were found to have SCT. Most of the patients belonged to the known sickle belts of India, including Maharashtra (32%), MP/Chattisgarh (25%), AP (10%), and Odisha (7%). Clinically palpable spleen was seen in 33% of cases. The mean hemoglobin S (HbS) percentage was 36.92% on HPLC. The mean hemoglobin, total leucocyte count, and platelet count were 14.39 g/dL, 8800/μL, and 308.8 × 103/μL at presentation, respectively. One patient (3.5%), who developed splenic infarct at an HAA, was found to have JAK2 V617F-positive polycythemia vera.
Patient Profile
JAK2 V617F-positive and hyperhomocysteinemia.
CDFI, color doppler flow imaging; CT, computed tomography; HAA, high-altitude area; Hb HPLC, hemoglobin high performance liquid chromatography; HbS, hemoglobin S; USG, ultrasonography.
Thrombus in the splenoportal venous axis was demonstrated on abdominal doppler and/or CT angiographic studies in 22.2% patients only. The pattern of infarcts seen on USG was diverse and included inferior pole, superomedial pole, wedge-shaped, peripheral, and diffuse infarct. The inferior pole of the spleen was the most common area infarcted as seen on USG studies (55.5%). One patient (3.5%) had partial splenic rupture, which resolved with conservative management. All patients required >2 months of hospital admission and recovered completely with conservative management with analgesia, hydration, rest, and aspirin 75–150 mg once daily. Hydroxyurea was not given to any patient. Patients with demonstrable thrombosis in the splenoportal axis were given short-term anticoagulation with vitamin K antagonists for up to 3 months. No patient required splenectomy. Splenic abscess due to superinfection, described in literature, was not seen in any of our cases. Prophylactic antibiotics were not administered. A complete radiological resolution on follow-up USG of the abdomen done at 6 months was seen in 30% of cases. All cases were placed under prolonged follow-up with a restriction on duties involving possible hypoxic conditions.
Discussion
Sullivan's initial description in 1950 of a young “sicklemic” patient with episodes of splenic infarction after each of the two airplane flights over the Rocky mountains was regarded a chance occurrence, only to be followed by Cooley et al.'s description of the triad of SCT, flying, and splenic infarction in six cases, which sort of established the relationship of SCT with flying. Splenectomy was considered the treatment of choice at that time (Conn, 1954).
In a review, Tsaras G et al. classified the complications of SCT as definite, probable, possible, and unlikely (Tsaras et al., 2009). Splenic infarction was considered a definite complication in this listing. However, Nigel S Key did not discuss splenic infarction as an important complication in their description of SCT complications (Key and Derebail, 2010). This was likely due to splenic infarct being an uncommon presentation of SCT in plain areas. Although exercise is a risk factor for sudden death and/or rhabdomyolysis in plain areas, splenic infarct still remains an uncommon complication in SCT. However, exposure to a high altitude and related hypoxia is a common precipitant of splenic infarction, as >90% patients who developed splenic infarction in our retrospective study had a SCT, which was hitherto not known/undiagnosed in an apparently healthy soldier. Similarly, in their case series, Velu Nair et al. reported SCT in two of five cases of splenic infarction on exposure to very high altitudes.
The extent of sickling seen in individuals with SCT is 2% at an altitude of 4050 ft, and dramatically rises to 8.5% at 13,213 ft. However, there is no significant increase in hemolysis, even in a hypobaric chamber simulating an altitude of 10,000–25,000 ft (Kark and Ward, 1994; Arora et al., 2008). All the soldiers who developed splenic infarct in this study were serving at an altitude of 12,000–16,000 ft. Vascular infarction occurs due to the vaso-occlusion by sickle cells in the relatively stagnant anoxic and acidotic milieu of the red pulp of the spleen compounded by severe hypoxic conditions at an HAA and physical stress and strain (Sheikha, 2005).
The problem of splenic infarction in SCT-natives of plain areas on exposure to a high altitude and related hypoxia is not seen in SCT-residents of HAAs. In one study where 143 individuals with SCT who were natives of an HAA were closely followed up, none of them developed the splenic syndrome (Addae et al., 1990). This observation suggests that acclimatization in the residents of HAAs has a protective effect on sickling and its related complications. Rachelle Nuss et al., in their study on 17 healthy young black men, observed that long-term residency at a moderately high altitude does not place persons with SCT at a risk of splenic dysfunction (Nuss et al., 1991).
The risk of splenic infarct on exposure to a high altitude is also affected by the percentage of HbS. In a patient with “pure” SCT, the HbS percentage is around 40%. A trimodal distribution of HbS percentage is seen in many populations, with a mean being around 41%, 35%, and 28% (Huisman, 1977; Sears, 1994). Co-inheritance of one or two α-thalassemia gene reduces the proportion of HbS to 35% and 28%, respectively. This gives protection against sickling at a high altitude as is seen in black SCT individuals in whom the splenic syndrome is much less common (Castro and Finch, 1974; Sears, 1994). The α-thalassemia gene is extremely rare in white people, making them more susceptible to the splenic syndrome at a high altitude and occurrence at a lower altitude (5280–7000 ft) (Sears, 1994). In our study, the mean HbS percentage was 36%, which places the SCT individuals at a risk somewhere in-between. Although the α-thalassemia gene mutation was not studied in this work, the α-thalassemia carrier rate in India varies from 1% to 80% (Higgs et al., 2001). Hence, it is likely that some of the patients had at least one α-thalassemia gene, giving them a partial protection. However, exposure to an altitude >12,000 ft and physical exertion likely overcome this protection, leading to the precipitation of a splenic syndrome.
Splenic infarction is rarely seen in patients with sickle cell disease (HbSS), compared to those with SCD, due to the fact that the spleen is atrophic due to repeated episodes of vaso-occlusive crises occurring early in life even in normoxic conditions in the majority of patients with HbSS (Sheikha, 2005). Other sickle cell variants, such as HbSC disease, Sβ+ thalassemia, and HbSE disease, have also been reported with massive splenic infarcts. Sleep apnea has also been implicated in splenic infarcts in SCT individuals without any apparent precipitating factor (Yeung and Lessin, 1976; Bodo et al., 1997).
In 1950 when the initial cases of splenic infarct in SCT individuals were presented, the acute nature of presentation with pain in the abdomen prompted splenectomy to be the treatment of choice (Conn, 1954). However, soon, the benign nature of the condition was realized and conservative management was proposed to be effective. Despite this consideration, splenectomy continues to remain a therapy in day-to-day practice, principally due to a lack of appreciation of an underlying SCT in hitherto undiagnosed patients presenting with acute abdomen and radiological evidence of splenic infarction (Sheikha, 2005). Thromboembolism and infection being the major causes of splenic infarction in the plains often leads to ignoring the possibility of SCT as an underlying etiology, until the patient is evaluated by an hematologist. In a recent retrospective study on 25 patients with splenic infarction in South India, no cases with SCT were documented (Vijayaraghavan and Thomas, 2016). However, it is not known if any of these patients were evaluated for an underlying SCT. Also, the complex interplay of SCT with different environmental/precipitating factors is evident in the case report of cocaine-induced sickle cell crisis in an SCT individual, which resulted in splenic, intestinal, and cerebral infarctions and multisystem organ failure necessitating a splenectomy, subtotal colectomy, and small bowel resection (Asfaw et al., 2013).
Conservative management of this syndrome consists of rest, adequate hydration with intravenous fluids, oxygen support, pain relief, descent to lower altitude, low-dose aspirin (75–150 mg), and a close observation for hemodynamic compromise, especially in patients showing evidence of splenic rupture radiologically. Splenic infarct is generally benign and associated with a complete recovery with conservative management (Sheikha, 2005; Arora et al., 2008). Pothula et al. (2008) described six cases of splenic infarcts at HAAs in SCT individuals, out of which two underwent splenectomy for near-total splenic necrosis (African American descent) and intractable pain (Mediterranean descent), respectively. We had one patient with near-total splenic necrosis/infarct seen radiologically. However, peripheral blood smear did not show any evidence of splenic dysfunction/hyposplenism, except thrombocytosis, and splenectomy was not resorted to. He recovered well with a close observation and conservative management and was asymptomatic at 6 months. Hence, the role of splenectomy even in the setting of near-total infarction/necrosis seen radiologically, in an otherwise stable patient with no evidence of infection, is debatable. Pain was manageable in all the cases, although 22.2% patients had some left hypochondrial discomfort at 3 months post-splenic infarct. As the Pothula et al. study made no mention of the percentage of HbS, it is not possible to correlate the outcomes with HbS percentage. However, it is possible that α-thalassemia gene co-inheritance may play a role in the extent of splenic infarction.
Complications such as splenic abscess and splenic rupture have been reported (Pothula et al., 2008). However, in our study, no patient developed splenic abscess, and antibiotics were not considered for prophylactic use. One patient had a partial rupture of the spleen, as seen radiologically on USG abdomen, with no clinical evidence of hemodynamic compromise. He showed complete recovery with conservative management, and splenectomy was avoided. Although we did not see any patient developing splenic abscess in our cohort, the same may need to be considered as advocated by the literature, although not in the setting of HAA-related infarct. Prophylactic antibiotics are unlikely to have any benefit. The role of hydroxyurea has not been studied in this setting. However, given the pathophysiology of the disorder and its rapid response to descent to a lower altitude and conservative management, hydroxyurea is unlikely to play any role. Also, the rarity of the syndrome precludes any large-scale study to define its role in this setting. It is also interesting to note that around 30% patients in our study showed complete radiological resolution of splenic infarct at 6 months post-presentation.
Although the splenic syndrome is a benign condition and responds well to conservative management, there could be a need for screening of military soldiers being deployed at very high altitudes. The screening policy for hemoglobinopathy in army recruits varies the world over. The U.S. army had a universal SCT screening policy during recruitment to the army till 1996, after which it was stopped. However, the U.S. Navy, Air Force, and Marines continue with SCT screening at enrolment (Fig. 1) (Naik and Haywood, 2015). Similarly, there is no such policy in the Brazilian army (Thompson, 2013). The identification of 24 cases of SCT-related splenic infarct due to HAA exposure over 4 years, during which period thousands of soldiers have been deployed in these areas, clearly indicates that the prevalence and risk is not very high, and universal screening at recruitment or deployment is unlikely to be cost-effective. The likely co-inheritance of α-thalassemia gene also provides significant protection against this complication. Also, as infarction is less common among seasoned soldiers vis-à-vis recruits, this could provide an additional explanation for the very low rate of splenic infarction observed. The restriction of SCT to the so-called sickle belts could provide an opportunity for the consideration of screening in this specific population, as >75% individuals seen in our study were from the three states of Maharashtra, AP, and Chattisgarh/MP. However, the general benefits of a screening program for identifying SCT in the newborns cannot be over-emphasized as there are other numerous complications with SCT that occur at plain areas in normoxic conditions.
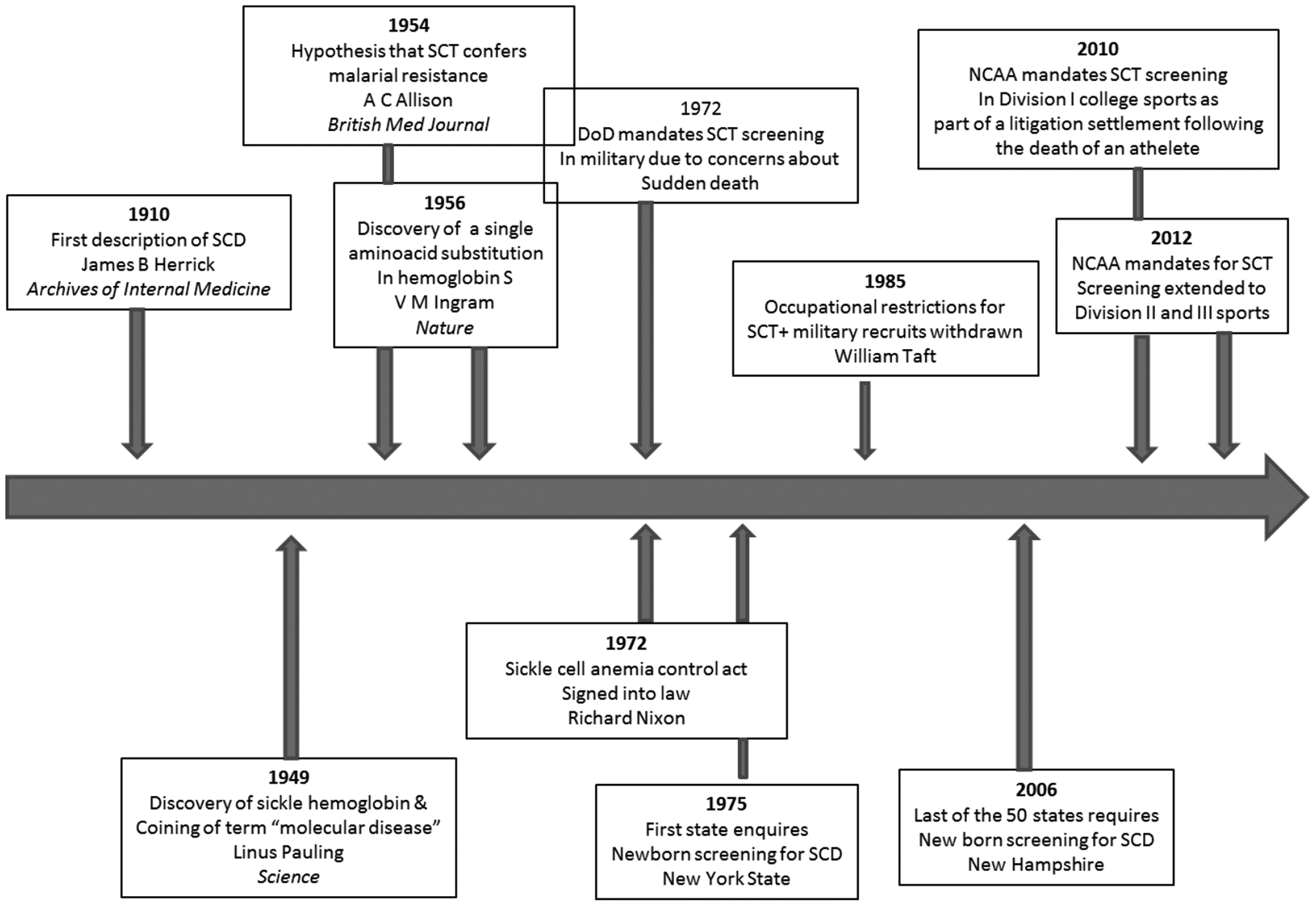
Timeline of major discoveries in sickle hemoglobin and sickle cell trait screening mandates. DoD, U.S. Department of Defense; NCAA, National Collegiate Athletic Association. Reproduced with permission. (Naik and Haywood, 2015)
An extensive review of literature suggests that this study presents the largest sample on splenic syndrome in SCT individuals exposed to high-altitude conditions.
Conclusion
SCT lies somewhere between being a benign carrier state and an intermediate disease phenotype (Key and Derebail, 2010). Under the effect of certain precipitating factors, individuals with SCT can develop varied complications. Splenic infarct is an uncommon complication in the plain areas in individuals with SCT, which might get greatly exaggerated under hypoxic conditions such as while ascending to HAAs. Despite its acute form of presentation, the outcome is good with conservative management, with the need for splenectomy arising in the rarest of rare cases. The knowledge of possible underlying SCT is of paramount importance in avoiding an unnecessary splenectomy when attending to a patient presenting with splenic infarction, especially after exposure to an HAA. The screening of targeted populations for SCT may help in reducing this complication in high-risk military soldiers, which may not be cost-effective given the vast numbers of soldiers being deployed to HAAs on a routine basis and the benign nature of this condition. With an increase in the number of people visiting HAAs for mountaineering and/or recreation purposes, the risk of an unnecessary splenectomy also increases. This study should inform medical practitioners, especially surgeons, on the need for evaluation of SCT in all cases presenting with splenic infarcts and the positive outcomes of conservative management in splenic infarction in SCT patients.
Ethical Approval
Informed consent was obtained from all participants included in the study, and ethical approval was obtained from the institutional ethics committee.
Footnotes
Author Disclosure Statement
No competing financial interests exist.