
Abstract
Abstract
Ultrasonography is a noninvasive, reliable, repeatable, and inexpensive technology that has dramatically changed the practice of medicine. The clinical use of portable ultrasound devices has grown tremendously over the last 10 years in the fields of intensive care, emergency medicine, and anesthesiology. In this review we present the various ways that handheld portable ultrasound devices can be used in austere environments. The purpose of this review is to consider the wide-ranging applications for providers going into the austere environment, which include pulmonary, ocular, vascular, and trauma evaluations, the postdisaster setting, and the role of ultrasonography in tropical diseases. This review is not meant to be a comprehensive how-to guide for each study type, but an overview of some of the more common wilderness applications. This review also focuses on the limitation of each study type. The goal is to help wilderness medicine providers feel more comfortable incorporating ultrasonography as part of their tool kit when heading into austere environments.
Introduction
Portable bedside ultrasonography has changed the way medicine and surgery are practiced in hospitals and clinics around the world. While based on a technology first recognized over a century ago, rapid technological advances in ultrasound hardware over the last two decades have markedly increased the effectiveness and utility of point-of-care ultrasound. From emergency departments to intensive care units, clinicians now routinely use ultrasound to diagnose life-threatening emergencies, guide procedures, assess volume status, inform resuscitation, and assist in everyday diagnoses. Relative to other imaging modalities, ultrasonography is a simple, inexpensive, noninvasive, and portable means to diagnose pathology and guide medical management. Ultrasound imaging uses nonionizing radiation and so may safely be used for serial examinations and on “at risk” (e.g., pregnant) patients. The true benefit of bedside ultrasonography is that it can drive interventions in real-time and be repeated as needed, right at the patient's bedside. Over the last few years, ultrasonography has been incorporated in medical school curricula around the country, accompanying courses like anatomy and pathophysiology. It has even been labeled as an integral part of the physical exam and the “stethoscope of the 21st century” (Gillman and Kirkpatrick, 2012). In addition, training in bedside ultrasound is now required to complete many residencies, as well as fellowships like Pulmonary and Critical Care Medicine.
Ultrasound's strengths in developed settings (e.g., portability, ease of use, battery power, etc.) make this technology uniquely valuable in austere settings. The utility of X-ray, computed tomography (CT), and magnetic resonance imaging (MRI) devices under austere conditions is limited by significant initial expense and complex maintenance requirements. Each of these devices are burdened with substantial weight, size, power, and environmental requirements that preclude their use for portable field imaging. These constraints have created an opening for a high-quality imaging device not so burdened. While wilderness environments can be notoriously inhospitable toward delicate electronic equipment—such as the early portable ultrasound devices—early adopters successfully proved this portable means of imaging can function effectively in austere environments and in so doing, revolutionized medical care there. Early ultrasound adopters in austere conditions included clinicians working at high altitude, postdisaster, in combat care, and space (Blaivas et al., 2005; Sargsyan et al., 2005; Allemann et al., 2006; Fagenholz et al., 2007b; Otto et al., 2009; Fagenholz et al., 2012; Law and Macbeth, 2011).
Harris and Fagenholz wrote the first chapter devoted to wilderness medicine imaging techniques in the Sixth Edition of Auerbach's Wilderness Medicine (2011). They recognized the barriers to ultrasound use in austere environments were real: electricity can be unreliable or nonexistent and ultrasound devices profoundly fragile. Since a medical provider will often have to carry the device on their person, the liabilities of device weight, reliability, tolerance of a wide range of ambient temperature and humidity conditions, and user proficiency were obvious hurdles to be overcome. By 2011, there existed enough practical clinical and research experience that inclusion of this novel imaging technique in this comprehensive text was indicated.
Over the past two decades, ultrasound devices have continued to get smaller, lighter, more portable, more durable, and resistant to hostile environments. Table 1 lists and describes a few of the portable ultrasound devices currently available. Image quality continues to improve and the cost of the devices continues to fall. The latest generation of ultrasound probes attach directly to a handheld tablet device or smart phone (Figs. 1 and 2). Many new devices use solid-state technology (rather than fragile, fixed array crystals in the probe), which allow a single more durable probe to be used for a variety of different indications. Batteries have become less expensive and more reliable. Solar arrays to power these devices (when off-the-grid) have similarly become much more robust, reliable, and inexpensive. Images obtained in the field can also be virtually relayed to experts who are not in the field for guidance regarding image acquisition and diagnostic confirmation. For all of these reasons, ultrasonography has quickly become the imaging modality of choice in the field of wilderness medicine (the provision of resource-limited medicine under austere conditions). Nonetheless, ultrasonography, especially in the austere environment, does have its limitations. Most notably the available studies are proof-of-concept articles that have yet to look at changes in clinical outcomes. In this article we review the variety of ways that handheld ultrasound devices are being used in austere environments and how a clinician could use this technology in the field.

The Butterfly iQ probe attaches to Apple devices. Photograph courtesy of Bryan Jarrett, MD.
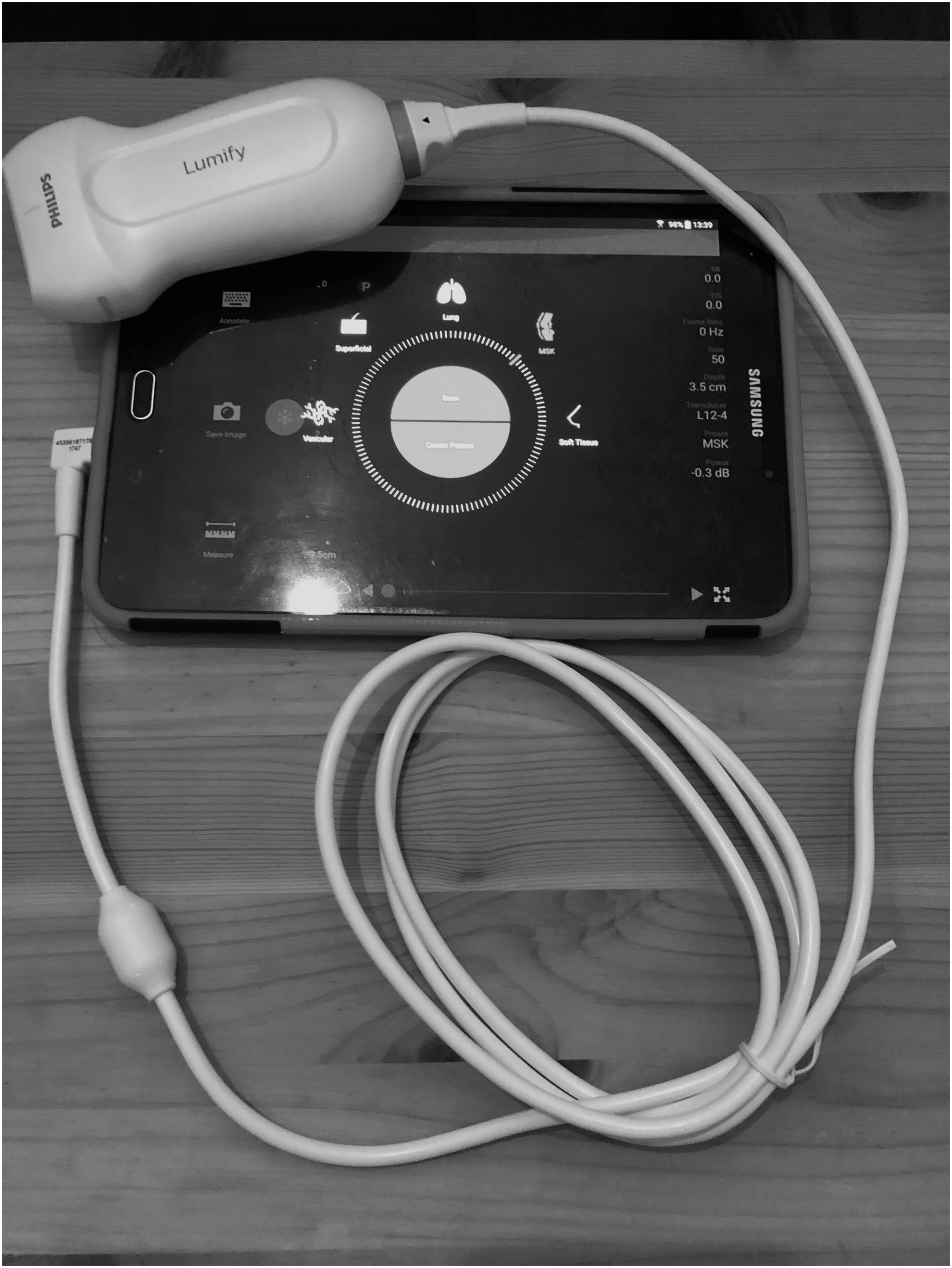
The Philips Lumify transducer attaches to an Android tablet. Photograph courtesy of Carlo Canepa, MD.
These Are a Few of the Currently Available Handheld Portable Ultrasound Devices and Their Features
Pulmonary
Lung ultrasonography is an excellent tool to evaluate pulmonary disease in general and specifically at high altitude (Picano and Pellikka, 2016). In a very early use of ultrasound in austere environments both for research and clinical care, in Fagenholz et al. (2007b) demonstrated that ultrasound was an effective diagnostic and monitoring tool for high-altitude pulmonary edema (HAPE) using a 28-zone anterior and lateral chest technique. Comet tails or B-lines (as seen in Fig. 3) indicate the presence of interstitial fluid and have had various names throughout the early literature. The sum of comet tail findings in each of the mid axillary, anterior axillary, mid clavicular, and parasternal locations bilaterally resulted in a total comet tail score (CTS). CTS scores of 11 patients suspected of having clinical HAPE were compared with 7 patients with no evidence of HAPE. They found an inverse correlation between a CTS (mean 31 and 11) and oxygen saturation (61% and 87%). They demonstrated that the CTS could successfully be used to diagnose and monitor the extent of HAPE in a high-altitude, remote, off-the-grid setting.
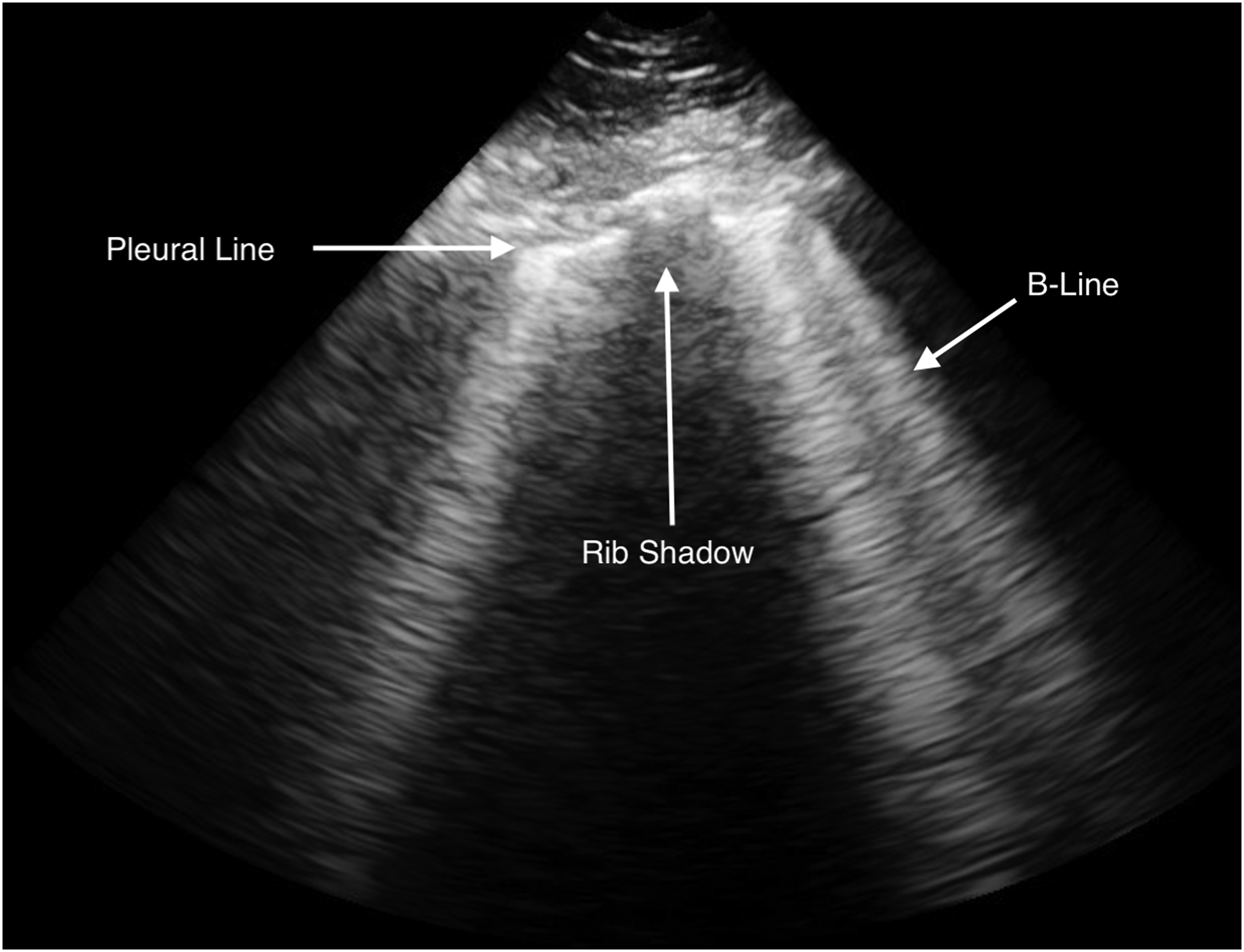
An anterior chest ultrasound demonstrates multiple B-lines extending from the pleural line, which indicates the presence of interstitial edema. Image courtesy of Carlo Canepa, MD.
Initial reservations about the utility of using ultrasound to diagnose and manage HAPE (a clinical diagnosis), and if ultrasound would change HAPE management were noted (Luks and Swenson, 2007). These early reservations have been answered by a robust, positive clinical experience. Ultrasound is now the diagnostic imaging modality of choice for most high-altitude pulmonary indications. Additional studies have gone on to demonstrate a high prevalence of clinically silent interstitial pulmonary edema using lung ultrasonography (Pagé et al., 2013). Pratali et al. (2010) demonstrated in 18 subjects that ultrasound lung B-lines appeared in 83% at 3440 m and 100% above 4790 m. They also found that two out of three climbers in their group who went on to develop clinical HAPE had increases in ultrasound lung B-lines at intermediate steps of ascent. Another expedition in Bolivia demonstrated that ultrasonography could detect the evidence of pulmonary edema in the absence of clinical signs of HAPE (69% of participants at 5270 m) (Dunton and Hanlon, 2012). While as Wimalasena et al. (2013) point out in their review article, it remains to be proven if ultrasound lung B-lines can aid in detecting the conversion of subclinical ultrasound findings into clinical HAPE, additional studies may help decide if screening hikers and mountaineers for subclinical HAPE using ultrasound may eventually prove helpful in determining who is at risk for developing clinical HAPE at a higher altitude.
Lung ultrasound can also be used to diagnose pneumonia when chest X-ray is not available. Shah et al. (2013) demonstrated in their prospective observational cohort study of 200 pediatric patients that lung ultrasonography had an overall sensitivity of 86% and specificity of 89% for diagnosing pneumonia. They used a 6-zone imaging protocol looking for lung consolidation with sonographic air bronchograms with a reference standard of an attending pediatric radiologist's reading of a chest posteroanterior (PA) and lateral radiographs. This study demonstrated that lung ultrasonography can be used to detect pneumonia when other imaging modalities are not available.
Noble et al. (2009) demonstrated that in the prehospital setting, nonultrasound trained providers can be taught through a brief training module how to correctly identify pneumothorax and pulmonary edema using the identification of B-lines and lung sliding. Ultrasonography is particularly useful for the detection of a pneumothorax, with a sensitivity approaching 100% and a specificity greater than 90% (Noble, 2012). Ultrasound often outperforms X-ray and matches CT for the evaluation of pneumothorax. The presence of lung sliding and B-lines will rule out the presence of a pneumothorax, while the absence of lung sliding indicates air in the pleural space that is causing the sound waves to scatter. This is an easy study to learn that can reliably distinguish an acute cause of dyspnea in the austere environment and help guide a timely intervention.
Several additional protocols have described how ultrasound may be used to assess other pulmonary pathology. In 2008, Lichtenstein described the Bedside Lung Ultrasound in Emergency (BLUE) protocol, which was able to provide the cause of acute respiratory failure in 90.5% of 260 participants using lung ultrasound alone. They describe the various lung ultrasound findings, including A-lines, B-lines, and lung point, which allow clinicians to distinguish between pulmonary edema, pneumonia, pulmonary embolism, pneumothorax, and COPD/asthma. Gargani and Volpicelli (2014) describe an 8-zone evaluation of the chest, consisting of 4 chest areas per side with excellent descriptions of various lung pathology. That these techniques can be readily taught in a rapid and reliable manner is a key strength of ultrasound use.
Ocular
Ocular ultrasound is an excellent tool to evaluate the eye and the causes of vision changes and loss of vision. The patient is examined while supine with the eye closed. A protective clear dressing may be applied over the eyelid. A generous amount of ultrasound gel provides a cushion for a linear probe to be placed over the closed eyelid. A sample ocular ultrasound image can be seen in Figure 4. Suspicion of a globe rupture is one of the few contraindications to ocular ultrasound. Blaivas et al. describe a prospective bedside ultrasound evaluation of 61 patients with 26 found to have findings on ultrasound. They describe finding globe injuries, central retinal artery occlusion, retinal detachment, vitreous hemorrhage, lens dislocation, and the presence of a foreign body (Blaivas et al., 2002). A bedside ocular ultrasound study by Yoonessi et al. (2010) found that the sensitivity for the diagnosis of retinal detachment was 100% and the specificity was 83% in a prospective, observational study in 48 emergency department patients. The sensitivity and specificity for using portable handheld ultrasound to detect intraocular foreign body in a porcine model by Shiver et al. (2005) was 88% and 95%, respectively.
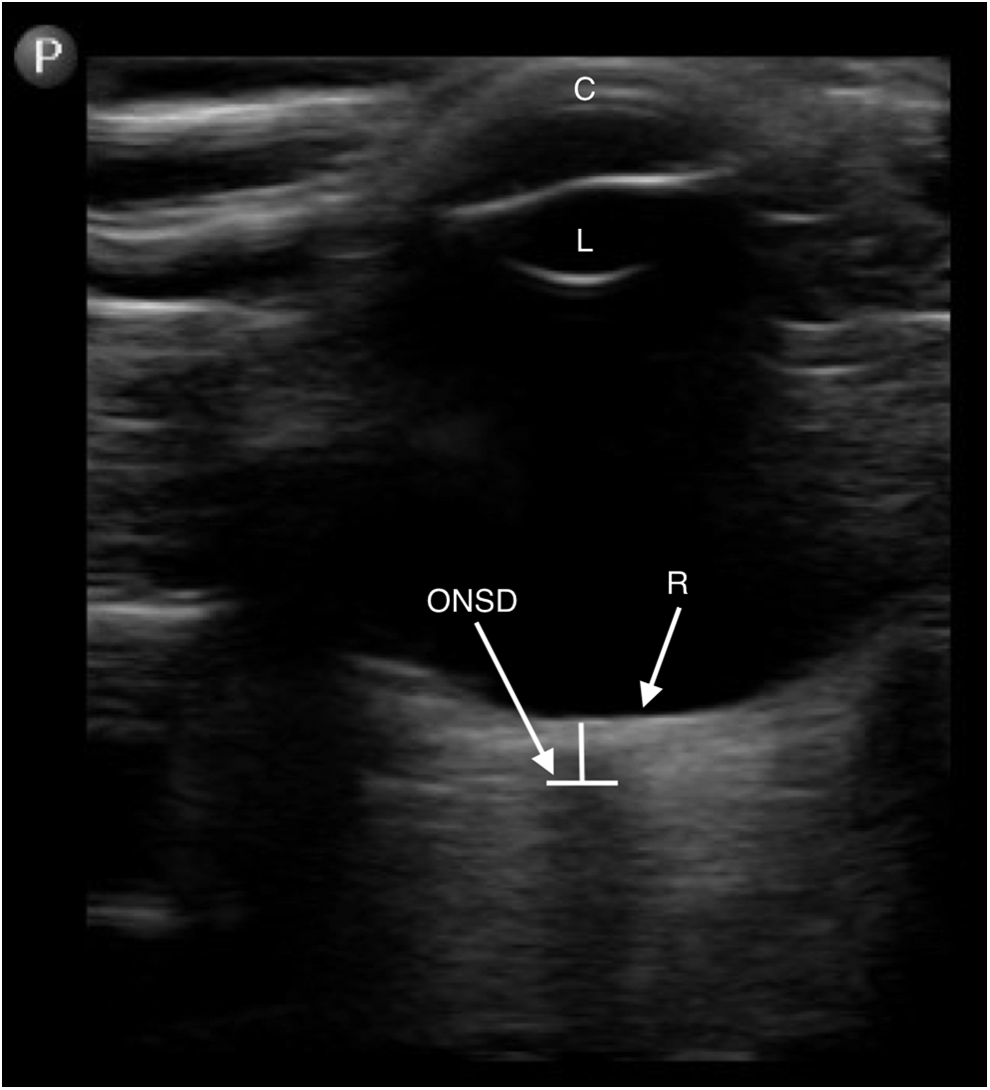
This is an ocular ultrasound obtained using a linear probe. An ONSD is measured 3 mm posterior to the retina (R). The cornea (C) and the lens (L) can also be seen. Image courtesy of Carlo Canepa, MD. ONSD, optic nerve sheath diameter.
Ultrasound has advanced research about early brain responses to acute hypoxia, most notably in examining the fundamental pathophysiology of acute mountain sickness (AMS). Many high-altitude studies have focused on optic nerve sheath diameter (ONSD) as a proxy for intracranial pressure (ICP) (Kanaan et al., 2015). As it exits the posterior globe, the optic nerve is surrounded by a distensible optic nerve sheath, which reliably varies with changes in ICP. By convention, the diameter of optic nerve sheath is measured at a point 3 mm behind the retina. In most studies, an ONSD of greater than 5 mm is considered abnormal. In Fagenholz et al. (2007a), described findings of increased ONSD in patients with symptomatic HAPE when compared with healthy altitude matched controls. Then, in a 2009 article, this same team then demonstrated that ONSD strongly correlates with the presence and severity of AMS as measured by the Lake Louise Score (Fagenholz et al., 2009). They found that the mean ONSD for those with AMS was 5.34 mm as compared with 4.46 mm for those without AMS (p < 0.0001). They also found a positive correlation for ONSD and the total AMS score. ONSD can also be used to evaluate those patients with signs of head trauma and suspected elevated ICP using a similar technique (Blaivas et al., 2003). ONSD should also theoretically be useful to evaluate ICP in high-altitude cerebral edema, although it has not been specifically studied for this purpose and should not supersede a clinical evaluation.
Vascular
Portable ultrasound devices have also been used to evaluate for venous and arterial thrombosis in the austere setting, particularly at mountaineering, where prothrombic risks (e.g., forced immobility in tents due to weather, prolonged travel to reach base camp, cold, dehydration, etc.) may exist. The standard clinical practice of using ultrasound to rule out deep vein thrombosis (DVT) can easily be employed under austere conditions. By using a linear array probe to perform serial compressions of the femoral and popliteal veins, lower extremity DVTs can be effectively evaluated. Veins that are noncompressible or that lack flow indicate the presence of a venous clot.
Fagenholz et al. (2007c) reported a case of arterial thrombosis at high altitude. They describe a previously healthy 41-year-old male hiking the Everest Base Camp trek with acute right lower extremity pain and loss of distal pulses. A bedside doppler ultrasound revealed decreased flow in the right superficial femoral artery and no flow in the right popliteal artery. The patient was treated with the available anticoagulation medications and evacuated to more advanced care. In a Kathmandu hospital, a CT angiogram confirmed the ultrasound diagnosis of arterial insufficiency due to clot.
Ultrasonography can also be used to determine total body fluid status in the field, most easily by measuring the inferior vena cava (IVC) collapsibility index (CI). Pitman et al. used this technique in their study which compared volume status in high-altitude trekkers with symptoms of AMS to altitude-matched controls without AMS (Pitman et al., 2015). The IVC CI evaluates a patient's IVC diameter throughout the respiratory cycle, comparing the smallest diameter to its largest by employing the use of M-mode on the ultrasound device. The CI is defined as the difference between the end expiration IVC and the end inspiration IVC diameters divided by the end expiratory diameter multiplied by 100. Hypovolemic individuals will have a greater variation in the IVC diameter and therefore a larger IVC CI. Although a qualitative evaluation of the CI can help guide resuscitation quickly, especially at the extremes, a calculated CI is more accurate at determining fluid responsiveness (Weekes et al., 2011; Duwat et al., 2014). While other techniques can be used to assess volume status, this is by far the simplest. Figure 5 demonstrates a sample measurement using ultrasound.
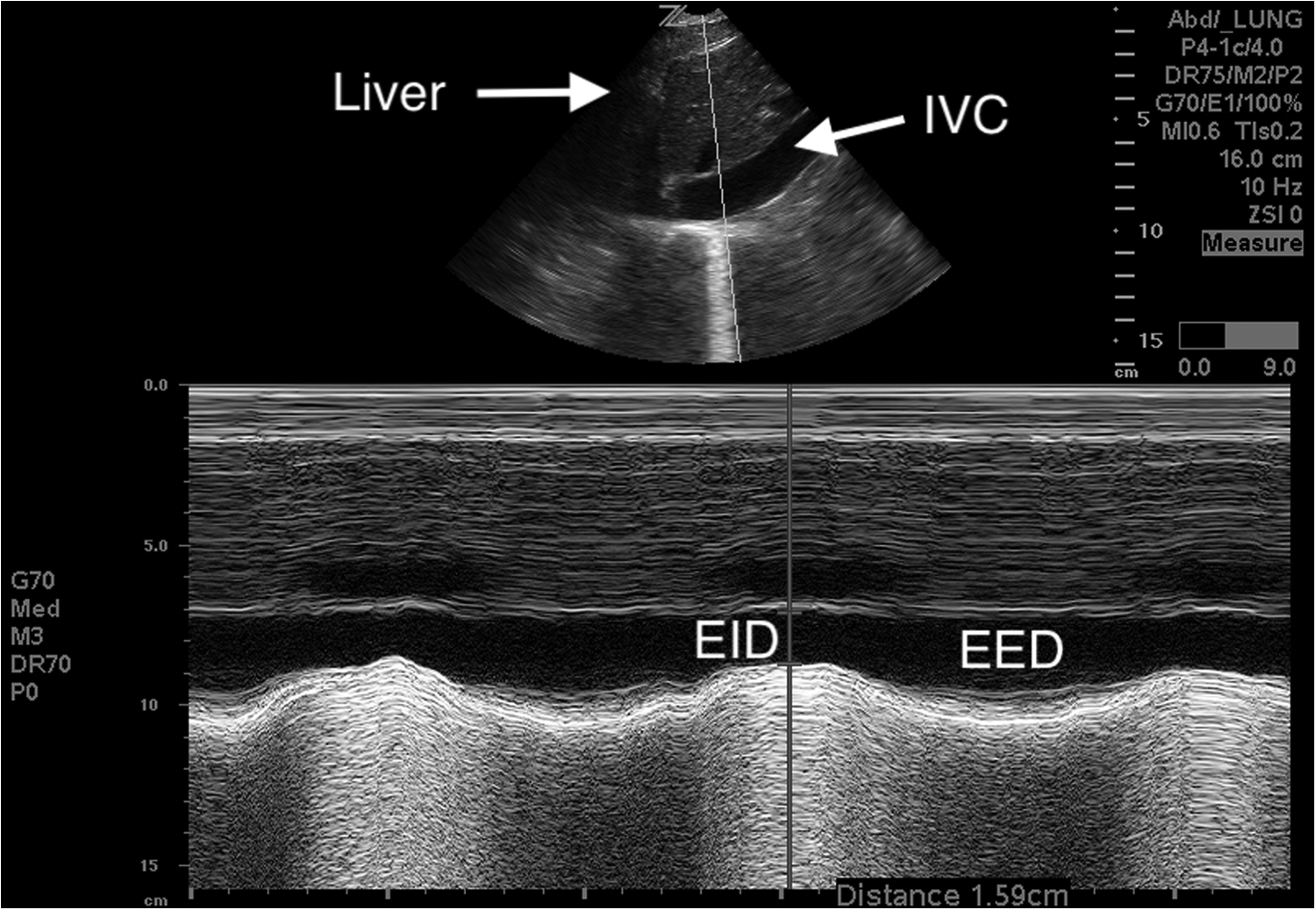
An IVC caval index can be calculated by measuring an EID and an EED using M-mode. Image courtesy of Carlo Canepa, MD. EED, end-expiratory diameter; EID, end-inspiratory diameter; IVC, inferior vena cava.
Where CI = collapsibility index, D = inferior vena cava diameter.
Trauma
The FAST (focused assessment with sonography for trauma) examination has become a standard assessment tool in emergency departments to detect intra-abdominal, intrathoracic, and pericardial injury. This four-view examination of the suprapubic, perihepatic, perisplenic, and pericardial areas can be completed in under 5 minutes and has a very high sensitivity for free fluid (indicating potential acute hemorrhage). Figure 6 demonstrates an example of a pericardial effusion found during a FAST exam. The extended FAST exam (or EFAST) adds the evaluation of the lungs for pneumothorax. Using this technique, pneumothorax is identified by lack of lung sliding and has been demonstrated to be more sensitive than chest X-ray (Kirkpatrick et al., 2004). The feasibility of performing EFAST exams in the prehospital setting have been extensively demonstrated (Jørgensen et al., 2010; Chin et al., 2013; Evans and Harris, 2012). The EFAST exam allows the field provider to make an early diagnosis and potentially intervene in the field with needle decompression for pneumothorax, pericardiocentesis for pericardial effusion, or to prioritize a more aggressive evacuation plan by making a rapid diagnosis. While of obvious potential benefit, prehospital ultrasound assessment has not yet been proven to improve outcomes when patients are transported to hospitals.

A subxiphoid cardiac view during a FAST exam demonstrates a pericardial effusion (E) anterior and posterior to the heart. The image is obtained by using the liver (L) as window to view the different chambers of the heart. Image courtesy of Carlo Canepa, MD. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
McNeil et al. (2009) demonstrate that a digital, handheld, portable ultrasound device can be reliably used to diagnose fractures in the austere environment. The technique involves scanning the cortex of the bone in multiple planes looking for disruptions and irregularities. They found a sensitivity of 100% and specificity of 94% when compared with plain radiography. Another study by Marshburn et al. (2004) found similar sensitivity (93%) and specificity (83%) in 58 patients with suspected long-bone fractures, as compared with plain films or CT.
Ultrasonography can also be used to evaluate patients for shoulder dislocations by using anterior and lateral approaches. In a study of 73 patients by Abbasi et al. (2013), no dislocation was missed by ultrasonography as compared with plain film radiology. The sensitivity for reduction in their study was 100% as well. They describe multiple findings for shoulder dislocation, including widening between the acromion and the humeral head, the disappearance of humeral head sign, the humeral head visualized below the coracoid process, and an empty glenoid fossa.
Postdisaster Setting
Shorter and Macias (2012) documented the various uses of portable handheld ultrasound after a 7.0 earthquake struck Haiti on January 2010. Their study was a retrospective, observational analysis of 51 ultrasound scans on 50 patients who presented to a clinic in Port-au-Prince. In this study they performed scans to evaluate for pregnancy after pregnancy tests were no longer available, for posttraumatic fracture evaluation, for foreign bodies and abscesses, and to assess the underlying cause of hypotension. Pregnancy evaluation and nontraumatic abdominal pain (in particular focusing on the gallbladder) made up half of the total studies performed. They report that ultrasound influenced management decisions (e.g., changes in medication, management, referral to a surgeon, and changes in level of care) in 70% of the scans performed, with nearly half being positive studies. They emphasize the importance of using ultrasonography to assist triage decisions when resources are in short supply. Similarly, one of these authors used a portable ultrasound to diagnose and guide treatment of patients immediately following the 2011 Japanese Great Northeast Earthquake and Tsunami disaster. This 9.0 earthquake disrupted Japan's highly developed medical infrastructure and rendered wide stretches of coastal Japan inaccessibility to any other imaging modalities—local nonportable ultrasound, CT, and MRI devices were destroyed in the tsunami and the electric grid disrupted—leaving only portable battery-powered ultrasound for imaging. A portable ultrasound from the United States was employed for abdominal and pulmonary assessments. The resilience and robustness of ultrasound in a disaster setting—even in a highly developed setting suddenly made acutely austere due to man-made or natural disaster—is a key strength of the technology which should not be underestimated.
Tropical Diseases
Ultrasonography can also be helpful in diagnosing infectious and tropical diseases. It is important to note that although the techniques utilized are similar to those used in the urban setting, many of the findings and the interpretations will vary dramatically based on location. One example is the focused assessment with sonography for HIV-associated tuberculosis (or FASH) exam, which has been demonstrated to be a rapid way to diagnose extrapulmonary tuberculosis in a high-prevalence setting like Sub-Saharan Africa (Heller et al., 2012). This protocol is similar to the FAST exam, which focuses on the presence of pericardial effusion, pleural effusion, and ascites, and adds the evaluation of the para-aortic lymph nodes, and focal liver and splenic lesions. The protocol involves evaluation of six different abdominal and subxiphoid positions. The Manual of Diagnostic Ultrasound in Infectious Tropical Diseases is another excellent and extensive resource that clearly presents the typical ultrasonographic findings of infectious diseases, of specific disease processes like liver cysts and abscesses, and of parasitic infections like filariasis, echinococcus, and many others (Lutz and Gharbi, 2006). While the acquisition of these image will be straightforward, the interpretation of these infectious processes on ultrasound require significant training, local experience, and expert consultation due to the unique appearance of each disease.
Limitations
Despite its relative strengths, the use of any electronic equipment under rigorous field conditions can be fraught with difficulties. The use of a new technology in an unproven austere environment, requires anticipation of potential difficulties for successful deployment. Preparation is key. The conditions of a high-latitude, high-altitude expedition pose very different challenges than the provision of routine ambulatory clinical care in a tropical rainforest. In subzero conditions as experienced by one of these authors (when performing the first ultrasound on the summit of Denali, 20,310 ft), simply assuring nonfrozen gel, a functioning battery, and device, successful articulation of the probe despite thick high-altitude gloves, and the difficulty of maintaining a sufficiently warm subject were anticipated. The remarkable degree of ambient brightness of high altitude that ultimately required multiple sleeping bags layered on top of the ultrasonographer to enable basic visualization of screen images was not. Where preparation fails, ingenuity may provide, but is a poor substitute. Similarly, efforts to keep the ultrasound device dry in a marine environment may be markedly advanced by sealed containers—but must be anticipated before departure. Traveling with multiple ultrasound gel bottles also requires careful consideration. The bottles are too large for carry-on luggage, but trapped air bubbles may expand while in checked luggage. The bottles are heavy, create significant waste once utilized, and the gel may require warming before use. Ensuring that the device, its batteries, power source (e.g., solar arrays), and gel supplies are adequate and well maintained requires prior planning.
Ultrasonography, like all clinical skills, is highly individually variable and user dependent. For all of the studies, intra and interrater reliability can vary widely. Therefore, a minimum number of supervised scans is required for each type of study before any provider can be considered proficient. A further number of scans can qualify a provider as an expert in that specific study. A provider's competence will increase dramatically with increased exposure to varied pathology and variety of cases. Studies have demonstrated that ultrasound image acquisition and interpretation can be easily and effectively taught to even medical novices (Noble et al., 2009). However, the importance of an appropriate clinical background cannot be underestimated. A provider who is unaware of the pathological process occurring may not be able to appropriately interpret the images obtained. Poor image acquisition can also lead to inaccurate conclusions and misguide management. This is where telemedicine and teleradiology can play an important role, especially when a rare or atypical diagnosis is being considered.
Each study type also comes with its unique obstacles for acquiring images. For example, when performing a lung or cardiac ultrasound, the user should recognize that an obese body habitus, a history of underlying lung disease, or any subcutaneous emphysema will make image acquisition more difficult and perhaps not possible. For abdominal studies such as a FAST, an aorta, or an appendix evaluation, an obese body habitus and gas-filled loops of bowel will make visualizing deeper structures more difficult as the sound waves are scattered. A child's appendix will be much easier to visualize than an adult's appendix as it is more superficial. Vascular studies are also often limited by the depth required to visualize each vessel. An ocular study should not be performed if there is any concern for a ruptured globe as the pressure applied during an ocular study can further the leakage of vitreous fluid. In addition, when measuring ONSD, the angle of the probe can affect the measurements taken. If not appropriately angled, a falsely low diameter measurement can be made. Each of these studies poses their distinct limitations, which each performing sonographer should consider before undertaking the study.
Critically, it must be recognized that ultrasonography is meant to be an adjunct to and not replace a thorough history and physical exam. There should always be a specific question that the provider is attempting to answer that ultrasonography can assist in answering. Additionally, in most indications, ultrasonography has much better sensitivity than specificity. In the austere environment it can help make decisions about immediate interventions and evacuation, but should rarely be used as the definitive test to rule out pathology. Lastly, most of the studies discussed in this article have small sample sizes and demonstrate proof of concept, but need to be followed up with larger sample sizes and nonexpert sonographer studies. While many studies demonstrated significant changes in management based on field ultrasonography, there is a lack of studies that have shown improvement in clinical outcomes. Studies focusing on changes in outcomes provide a ripe area for further study.
Conclusion
In austere environments, portable point-of-care ultrasound devices have proven invaluable, from the postdisaster setting in the developed world to high-altitude expeditions working in resource-poor clinics. This article has presented a few of the ways that ultrasound can be used as an adjunct in the austere setting, but there are many more applications that we have not discussed. Ultrasound can be used for a plethora of other nonwilderness-specific diagnoses that commonly present in austere environments, including skin and soft tissue infections, biliary disease, appendicitis, pregnancy, bowel disease, kidney stones, and others. As ultrasound devices continue to shrink in size, become more durable and reliable, and costs continue to drop, it seems highly probable that portable handheld ultrasound devices will become a standard component of every comprehensive wilderness medical kit and that adequate training in ultrasound will become a prerequisite for competent advanced wilderness medical providers. The field of ultrasonography in the austere environment is still in its infancy and would benefit greatly from studies that focus on nonexpert sonographers, larger sample sizes, and changes in clinical outcomes.
Footnotes
Authors' Contributions
C.A.C: Data collection, drafting the article, final approval; N.S.H: Conception and design of the work, critical revision of the article, and final approval.
Authorship Confirmation Statement
All coauthors have reviewed and approved of the article before submission.
Author Disclosure Statement
No competing financial interests exist.