
Abstract
Abstract
Background:
Acute mountain sickness (AMS) is a common disease that may have a pulmonary component, as suggested by interstitial pulmonary edema quantified by the B-line score (BLS) on ultrasound (US). This subclinical pulmonary edema has been shown to increase with ascent to high altitude and AMS severity, but has not been prospectively associated with AMS incidence in a large prospective study.
Materials and Methods:
This prospective observational study was part of a randomized controlled trial enrolling healthy adults over four weekends ascending White Mountain, California. Subjects were assessed by lung US and the Lake Louise Questionnaire at 4110 ft (1240 m), upon ascent to 12,500 ft (3810 m), and the next morning at 12,500 ft (3810 m).
Results:
Three hundred five USs in total were completed on 103 participants, with 73% total incidence of AMS. The mean (±standard deviation) BLS increased from baseline (1.15 ± 1.80) to high altitude (2.56 ± 2.86), a difference of 1.37 (±2.48) (p = 0.04). Overall BLS was found, on average, to be higher among those diagnosed with AMS than without (2.97 vs. 2.0, p = 0.04, 95% confidence interval [CI] −∞ to −0.04). The change in BLS (ΔBLS) from low altitude baseline was significantly associated with AMS (0.88 vs. 1.72, r2 = 0.023, 95% CI −∞ to −0.01, p = 0.048).
Conclusions:
Interstitial subclinical pulmonary edema by lung US was found to have a small but significant association with AMS.
Introduction
Acute mountain sickness (AMS) is a constellation of symptoms that commonly affects travelers ascending to altitudes above 8250 ft (2500 m). While the condition is usually self-limited, severe AMS can be debilitating and may progress to potentially fatal high altitude cerebral edema (Hackett and Roach, 2001). Altitude illness is a common occurrence in the tens of millions of tourists and trekkers who travel to high mountains, with a 25%–69% incidence in the mountains of Western United States (Honigman et al., 1993; Lipman et al., 2012, 2018) and upwards of 50% in Swiss Alps, which was altitude dependent (Maggiorini et al., 1990). Although the exact pathophysiology of AMS is unknown, the disease is considered primarily a cerebral disorder (Hackett and Roach, 2001; Wilson et al., 2009), one marked by increased cerebral inflammation from a combination of both hydrostatic factors and biochemical mediators leading to increased blood–brain barrier permeability (Jensen et al., 1990; Baumgartner et al., 1994), resulting in systemic compensation to optimize cerebral oxygen delivery. While hyperventilation is a physiologic hallmark of high altitude travel, lungs are often considered victims of the hypobaric hypoxic environment of high altitude (Swenson, 2014), with ventilatory responsiveness mediated by peripheral chemoreceptors in the carotid body and centrally induced hyperventilation (Swenson et al., 1995).
An alternative concept has lungs as perpetrators of disease (Swenson, 2014), with initial hypoxia and development of a subclinical pulmonary edema an inciting cause, furthering a hypoxic state that worsens cerebral oxygen delivery and a subsequent cascade of physiologic changes. Impaired pulmonary diffusion has been found in those with AMS compared with healthy cohorts (Ge et al., 1997), in addition to increased alveolar-arterial oxygen pressure differences consistent with interstitial pulmonary edema (Coates et al., 1979; Grissom et al., 1992; Welsh et al., 1993), although these have also been found to be nonsignificant trends (Dehnert et al., 2010). The pulmonary edematous findings are similar to fluid retention and increased total body water in those most symptomatic with AMS (Hackett et al., 1982; Koller et al., 1991; Loeppky et al., 2005). It is unclear what role subclinical interstitial pulmonary edema has in the pathophysiologic paradigm as imaging of pulmonary edema has not been associated with AMS incidence in a large prospective study to date.
Lung ultrasound (US) has been shown to effectively detect pulmonary edema (Jambrik et al., 2004; Baldi et al., 2013; Miglioranza et al., 2013). B-lines are the US hallmark of interstitial pulmonary edema (defined as discrete, vertical, hyperechoic reverberation artifacts that arise from the pleural line, extending to the bottom of the screen without fading), which move synchronously with lung sliding (Volpicelli et al., 2012). B-line scores (BLSs) are strong predictors of pulmonary edema in congestive heart failure (Martindale et al., 2016), and international guidelines are moving toward chest US as the bedside standard for assessing pulmonary edema (Picano and Pellikka, 2016). Due to technology and availability of US, this technique has been replicated in prehospital and wilderness settings (Fagenholz et al., 2007; Prosen et al., 2011). In a small cohort, BLS was found to increase with ascent to high altitude, improve with descent, and be associated with decreased oxygen saturation and increased AMS severity (Pratali et al., 2010). While evidence of pulmonary extravascular edema by BLS has been found in the majority of asymptomatic high altitude climbers (Strapazzon, et al., 2015), the association of BLS with AMS incidence has not been prospectively studied on ascent to high altitude in a large cohort. The objective of this study was to correlate the relationship of BLS and AMS upon rapid ascent to high altitude.
Materials and Methods
Study design
This prospective observational study was part of a double-blind, randomized placebo-controlled trial comparing the inhaled steroid budesonide and diuretic acetazolamide with placebo for prevention of AMS (Lipman et al., 2018). After informed consent was obtained, participants completed the baseline demographic sheet and underwent lung US at a baseline altitude of 4100 ft (1240 m). They then drove to 11,700 ft (3545 m) and then hiked to and slept at 12,500 ft (3810 m). The US measurements along with the Lake Louise Questionnaire (LLQ) of AMS symptoms were repeated the evening of ascent and again the following morning.
Selection of participants
A convenience sample of volunteers was recruited through a variety of e-mail lists with both local and national distribution, in addition to posted advertisements in Northern and Southern California. Inclusion and exclusion criteria were presented for participants to self-screen for eligibility before enrollment. Eligible participants for this free study had to be healthy, reside at an altitude <4100 ft (1240 m), and able to complete a moderately strenuous hike at high altitude. The study was conducted over four weekends in August 2016 in the White Mountains of California.
Exclusion criteria included participants younger than 18 or older than 65 years; pregnant or thought to be pregnant; lived or slept at altitudes >4100 ft (1240 m) in the past week; having taken diuretics, steroids, acetazolamide, or non-steroidal anti-inflammatory drug (NSAID) the week before the study; allergic to acetazolamide, sulfa medication, or corticosteroids; with symptoms consistent with AMS at baseline; or having a hazardous condition, which precluded the ability to hike to high altitude, including sickle cell anemia, asthma, or chronic obstructive pulmonary disease (COPD), severe anemia, or severe coronary artery disease. Stanford University School of Medicine Institutional Review Board approved the study.
Lung sonography protocol
US was performed with participants in the supine or near-supine position. The anterior chest wall was delineated from the sternum to the anterior axillary line and subdivided into upper and lower halves (approximately from the clavicle to the nipple line and from the nipple line to the diaphragm). The lateral zone was delineated from the anterior to the posterior axillary line and subdivided into upper and lower halves (Volpicelli et al., 2008). One scan was recorded from each of the eight areas. B-lines were counted in a single rib space on a still image selected as most representative of the maximum B-lines seen in that area. The sum of the B-lines was used to calculate the overall BLS, indicating the extent of interstitial fluid in the lung. Examinations were performed using a portable US system (iViz by SonoSite, Inc., Bothell, WA) equipped with a phased array probe (P21v probe, bandwidth 5-1 MHz) set to a scan depth of 16.4 cm. Ultrasonographers were blinded to LLQ, oxygen saturation, and study drug information. All images were reviewed at a later date by a US faculty physician blinded to patient information.
Data collection
The LLQ is a widely used, standardized, self-reported clinical survey used for quantification of AMS. A diagnosis of AMS on the LLQ requires a score of three or greater with the mandatory presence of headache and at least one of the following symptoms: dizziness or lightheadedness, fatigue, gastrointestinal symptoms (nausea/vomiting), or difficulty sleeping (Maggiorini et al., 1990; Roach et al., 1993). The LLQ was measured the evening of ascent to high altitude and again the next morning, with values of the morning after ascent (or at time of rescue medication) used for AMS analysis to ensure that maximum amount of time was allotted for symptoms of AMS to declare themselves. Furthermore, an LLQ administered the evening of ascent would include the quality of sleep from low altitude, which would lose accuracy. Values between the baseline level and night after ascent to high altitude were computed. Peripheral oxygen saturation (SpO2) was assessed by fingertip pulse oximetry (Nonin Medical Products, Minneapolis, MN).
Statistical methods
The primary outcomes were BLS and incidence of AMS the morning after ascent. A Wilcoxon rank-sum test and Welch two-sample t-test were used to compare BLSs among AMS and non-AMS groups. Secondary outcomes included change in BLS between each encounter (ΔBLS) compared with the peak subjective LLQ score and incidence of AMS; ΔBLS during ascent; and BLS compared with the medication study arm to isolate potential bias from medications. Pairwise t- and Wilcox tests were used to assess whether BLSs were significantly different among treatment groups and ascent locations. Multiple comparison p-value correction was performed using the Holm method. Analysis of variance was used to assess whether BLS variability could be explained by medication. Linear regression was utilized using the r2 correlation test; p-values <0.05 were considered significant and 95% confidence intervals (CIs) were used. All analyses were conducted using R 3.2.3 software (R Development Core Team 2007).
Results
Three hundred five USs in total were completed on 103 enrolled participants. All participants completed the study and were included in the analysis. Participant demographics are shown in Table 1. As there was no significant BLS variability between drug treatment arms (Table 2), all groups were combined into a single cohort for analysis (Kanaan et al., 2015). The cumulative incidence of AMS was 73% with a mean LLQ severity of 4.15 ± 3.14.
Participant Demographics
SD, standard deviation.
B-Line Score by Treatment Group and Combined
Data are presented as mean ± SD.
The mean BLS increased from baseline to the morning after ascent, a difference of 1.37 ± 2.48 (p = 0.04). The morning after sleeping at high altitude, overall BLS was found to be higher among those diagnosed with AMS (2.97) than without (2) (p = 0.04, 95% CI −∞ to −0.04), although there was no significant correlation between LLQ total score and BLS (r = −0.014, p = 0.89). The change in BLS from low altitude (ΔBLS) was significantly associated with the diagnosis of AMS (r2 = 0.023, 95% CI −∞ to −0.01, p = 0.048). Although statistically significant, the 95% CI effect size was very small with a mean BLS difference of 0.01 for those with a positive AMS diagnosis. The ΔBLS between evening of ascent and the next morning did not show a significant correlation with ΔSpO2 (r2 = 0.048, p = 0.52) (Fig. 1).
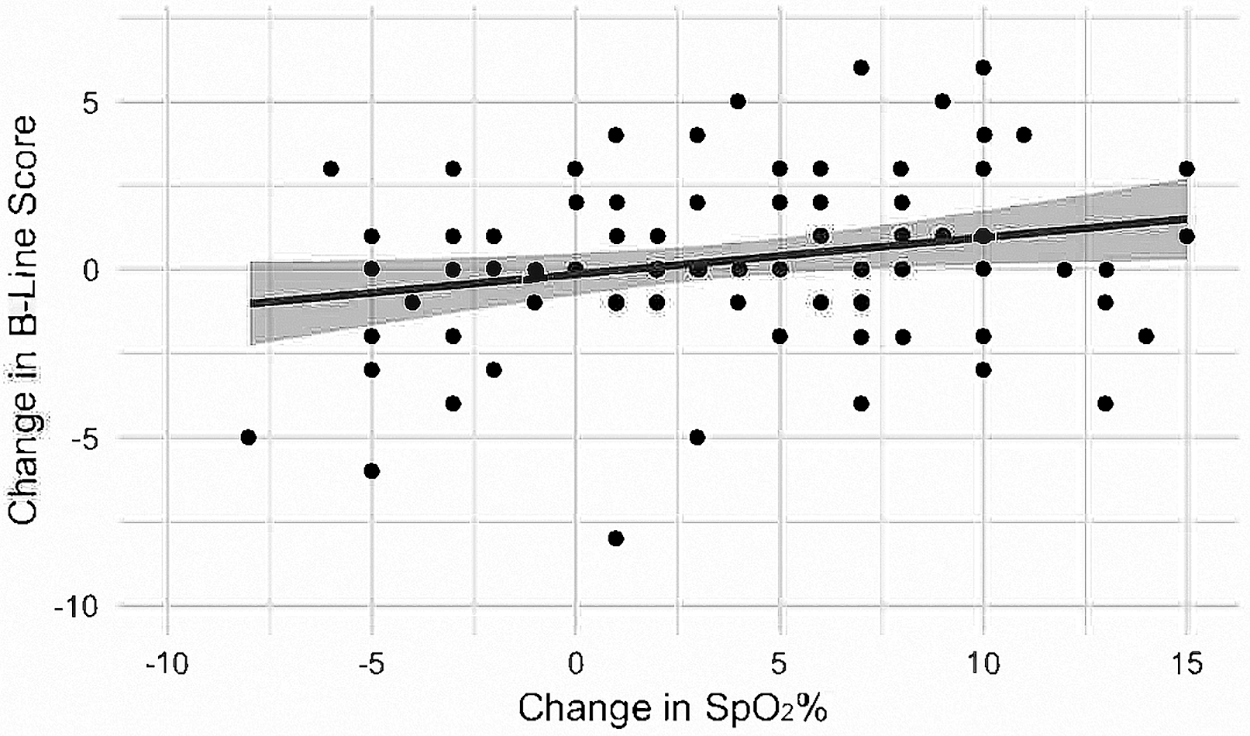
Correlation of change in B-line score and change in peripheral oxygen saturation.
Discussion
Our results demonstrated a significant association between increased BLSs and those diagnosed with AMS on ascent to high altitude. This is the largest study to date to examine this relationship, and results support consideration of subclinical interstitial pulmonary edema in the pathology of AMS. While prior studies have shown mixed results on the observed significance of the AMS and BLS association (Pratali et al., 2010; Bouzat et al., 2013; Page et al., 2013; Strapazzon et al., 2015), these conclusions are limited by their small sample sizes.
We are cautious in the interpretation of our findings, however, as there was a narrow margin of statistical significance, small effect size, and an observed increase in BLS at high altitude regardless of AMS symptoms. While ΔBLS was significantly correlated with an eventual diagnosis of AMS, the observed large CIs minimize the certitude of this relationship. The association of AMS with increased pulmonary interstitial fluid is intriguing, and as it is similar to findings of increased systemic fluid retention with AMS (Loeppky et al., 2005), it encourages further investigations into the role of aquaporins and fluid retention in high altitude illness.
Most investigations of pulmonary fluid accumulations in the high altitude milieu have been in the context of high altitude pulmonary edema, which is a separate clinical entity from AMS. The observed increase in BLS on ascent to high altitude is consistent with prior studies, but the number of B-lines observed at high altitude has been shown to be highly variable (Bouzat et al., 2013; Strapazzon et al., 2015; Taylor et al., 2017). Hypobaric hypoxia leads to pulmonary vasoconstriction, increased pulmonary arterial pressures, and subsequent pulmonary hypertension (Hackett and Roach, 1990). The increased hydrostatic pressures likely lead to extravasation of fluid to the interstitial space as small increases in vascular pressures lead to pulmonary edema (Fishman, 1972). These pulmonary changes have been observed in experimental hypobaric hypoxic models (Miserocchi et al., 2001a, 2001b) and increased with exertion at high altitudes (Cremona et al., 2002; Eldridge et al., 2006). This asymptomatic interstitial fluid has been suggested as the etiology of impaired pulmonary diffusion at altitude (Grocott et al., 2009). Increased BLS in those with, compared with those without, AMS may provide pathophysiologic insight into the mechanism of high altitude illness, if the lungs are to be considered in the upstream signaling mechanism from a pulmonary hypoxic injury. However, as recent trials have shown the lack of efficacy of a pulmonary acting glucocorticoid (Berger et al., 2017; Lipman et al., 2018), we cannot exclude the possibility that the pulmonary findings may represent downstream fluid accumulation.
Acetazolamide is an old drug thought to combat AMS by inhibition of carbonic anhydrase that induces bicarbonate diuresis, leading to compensatory hyperventilation and raising arterial oxygen concentrations (Swenson, 1998). This has been theorized as the mechanism to diurese extravascular pulmonary edema and reduce the arterial-alveolar pressure differential seen in AMS (Grissom et al., 1992). This theory is supported in those with AMS as acetazolamide showed improved arterial oxygenation, more than could be accounted for by increased ventilation (Grissom et al., 1992), which speaks of an improvement in diffusion from diuresis. Hypoxic pulmonary vasoconstriction reduction by acetazolamide is mediated by noncarbonic anhydrase inhibition of pulmonary vascular smooth muscle (Hohne et al., 2004; Swenson, 2006), and as there is inhibition of renal, vascular, and chemoreceptor carbonic anhydrase, the benefit of acetazolamide for AMS prevention is likely a mixed picture. Furthermore, acetazolamide acts as an aquaporin inhibitor, which may contribute to its role in osmoregulation (Swenson, 2016). To isolate the potential confounding effect of acetazolamide's impact on pulmonary interstitial edema and diffusion, we analyzed our results excluding the 35 participants assigned to acetazolamide and found an unchanged statistically significant difference in BLS and presence of AMS (p = 0.04). This reinforces the association of increased interstitial pulmonary edema and AMS.
Although hypobaric hypoxia is accepted as the primary environmental insult leading to AMS (Roach et al., 1998; Kayser, 2009), demonstrating this relationship has proved complex. Multiple studies have found deterioration in lung function in those with AMS compared with healthy controls with lower pulmonary diffusing capacity (Ge et al., 1997; Agostoni et al., 2013), and lower SpO2 is a common, if not sensitive, observation (Roach et al., 1998; Brierley et al., 2012; Subudhi et al., 2014). Our lack of observed significant correlation between SpO2 and BLS supports this ambiguity as greater changes in peripheral oxygenation have been significantly associated with increased pulmonary interstitial edema (Pratali et al., 2010). While the physiologic prediction that low arterial oxygenation correlates with AMS has been substantiated (Roach et al., 1998; Collier et al., 2016), symptoms have resolved on acclimation without proportionately increased oxygenation (Subudhi et al., 2014). Overall, hypoxemia and AMS have very poor accuracy, rendering SpO2 an inaccurate test for diagnosis of altitude illness or AMS prediction (Ge et al., 1997; Tannheimer et al., 2002; Kayser, 2009; Brierley et al., 2012; Faulhaber et al., 2014; Subudhi et al., 2014).
Handheld point-of-care US has been examined in diverse wilderness environments (Sutherland et al., 2008; Ladd et al., 2016), but it has been challenged for its applicability as a diagnostic adjunct for AMS (Kanaan et al., 2015). Our data do not support US as a reliable diagnostic or prognostic tool for AMS. As baseline measurements are necessary to determine ΔBLS, US-trained practitioners would need to be available at all points of ascent, limiting its applicability to the wilderness environment. In addition, due to the universal prevalence of B-lines on lung US at high altitude, point diagnostic imaging would provide limited insight into the disease state. Future direction for high altitude studies that utilize handheld US would benefit from arterial blood gas analysis to examine alveolar-arterial gradients or incorporation of lung diffusion capacity measurements and provide further physiologic insight into the pathology of high altitude illness.
Limitations
This study was conducted during an ongoing, randomized controlled trial investigating acetazolamide and inhaled budesonide for prevention of AMS. Although the relationship between drug ingestion and BLS was investigated and not found to be a significant confounding variable, it is possible that changes in AMS rates between the intervention groups may have introduced heterogeneity. Our study staff had a range of training, from medical students during an elective month to fellows, and this may have affected the accuracy of BLS. All studies were reviewed for uniformity by US fellowship-trained physicians at a later date, and all staff were given hands-on training on the lung US technique by US-trained faculty to optimize accuracy. Furthermore, whereas these physicians were blinded to the participants' LLQ scores, they were understandably aware of the examining elevation and participants' appearance of health. Most participants originated from San Francisco and Los Angeles, which limits extrapolation to other groups and elevations. Last, a year after the study and analysis had concluded, the Lake Louise AMS score was revised to exclude its sleep component (Roach et al., 2018). As our AMS diagnosis and severity were based on sleep scores that included high altitude sleep (excluding low altitude sleep), our analysis likely maximized diagnostic accuracy.
Conclusions
We found a significant increase in both overall BLS and ΔBLS with AMS on rapid ascent to high altitude. While the associations were only slight, these findings build on prior evidence to support increased fluid and the potential pathophysiologic connection of interstitial pulmonary edema and AMS.
Footnotes
Acknowledgments
Material support of the ultrasound machines was provided by SonoSite, with all materials returned at the end of the study. The study would not have been possible without the infrastructure support and generous attitude of the White Mountain Research Station and staff, as well as the enthusiasm of the high altitude trekkers who made this project successful.
Author Contributions
C.A., G.S.L., and V.L. had full access to all of the data in the study and take responsibility for the integrity of data and accuracy of data analysis. C.A., G.S.L., D.P., R.-W.H., P.B., N.J., C.J., M.C., K.E., A.S., P.B., L.L., and J.R. were responsible for data collection. C.A., G.S.L., D.P., and V.L. were responsible for design and conduct of the study. C.A., G.S.L., V.L., and C.P. were responsible for data management and analysis and interpretation of data. C.A., G.S.L., D.P., R.-W.H., P.B., N.J., C.P., C.J., M.C., K.E., A.S., P.B., L.L., J.R., and V.L. were responsible for preparation, review, and approval of the article. G.S.L. takes responsibility for the article as a whole. All authors have reviewed and approved the manuscript before submission.
Author Disclosure Statement
No competing financial interests exist.