
Abstract
Abstract
Therapeutic benefits of hypoxic training have been suggested for clinical populations, such as elderly who could suffer loss of lower limb muscle strength and higher risk of falling. This study investigated the effects of 18 weeks of whole-body vibration (WBV) training in normobaric hypoxia on the strength parameters of an elderly population. Thirty-one healthy elderly participants were randomly assigned to a hypoxic whole-body vibration group (HWBV; n = 10), normoxic whole-body vibration group (NWBV; n = 11), or control group (n = 10). The experimental groups received the same vibration treatment in a hypoxia chamber (HWBV: 16.1% fraction of inspired oxygen [FiO2]; NWBV: 21.0% FiO2). Isokinetic leg muscle strength was evaluated using a Biodex System-3 isokinetic dynamometer. Body composition was obtained with dual-energy X-ray absorptiometry. There were no significant differences between groups in either strength or body composition parameters. The NWBV group showed statistically significant improvements in the maximal strength of knee extensors, with a small effect size (p = 0.004; d = 0.54). No significant differences were found in any variable of the HWBV group. The combination of WBV training and exposure to normobaric cyclic hypoxia carried out in the present study did not have an effect on strength parameters in healthy elderly subjects.
Introduction
Muscular strength is reduced by 15% per decade after the age of 50 years, and by 30% after the age of 70 years (Verdijk et al., 2007). Among other risk factors, the loss of muscle strength in the lower limbs has been considered responsible for a higher risk of falls (Goudarzian et al., 2017a), which is a major cause of morbidity and mortality in present-day society (Marin-Cascales et al., 2015). The majority of falls among the elderly take place in situations that demand reactive postural control, such as the recovery from external perturbations (Niino et al., 2000). Muscle fatigue has been shown to alter the peripheral proprioceptive system and the central processing of sensory inputs, both of which are essential for this reactive postural control (Taylor et al., 2000).
On these matters, research suggests that physical activity designed to make lower extremity muscles more fatigue-resistant may improve postural control (Papa et al., 2015a, 2015b) and decrease the risk for falls (Paillard, 2012; Nam et al., 2013). However, very few older adults are meeting the recommended levels of physical activity due to a large number of barriers, such as ill-health, pain, and injury (Taylor, 2014). Heavy resistance exercises provide greater muscular adaptation (Miller et al., 2018), and due to age-related factors, such as cardiac limitation, weak balance, or lack of sufficient motivation or interest, many elderly people are unable or reluctant to do these exercises (Goudarzian et al., 2017a). Furthermore, multicomponent exercise programs with balance and muscle strength training could be the most effective to prevent falls (Karlsson et al., 2013).
In this sense, whole-body vibration (WBV) training has been reported as a safe and tolerable alternative for this population (Ko et al., 2017). Some studies have shown the same level of improvement in muscle strength and other physical fitness factors after WBV training when compared with resistance training (Delecluse et al., 2003; Bogaerts et al., 2007). WBV training generates simulated mechanical vibrations, which in turn activate the neuromuscular control system, increase the level of excitement and the number of motor units recruited and coordinate synergistic and antagonistic muscles during rapid muscle contractions, thus enhancing muscle function (Delecluse et al., 2003). As muscle strength and lean mass are highly interrelated, WBV training could have a positive effect on muscle mass (Chen et al., 2017). Numerous intervention studies have been carried out to increase muscle mass (Chen et al., 2017) and muscle function (Goudarzian et al., 2017b; Ko et al., 2017) in the elderly. However, some of them have shown controversial results. The different vibration frequencies, durations, and amplitudes used in the aforementioned studies could explain these contradictory results. In this context, durations from 6 weeks to 1 year seem to be required to get these benefits (Goudarzian et al., 2017b). Other factors, such as training volume could also alter the effects of the treatment, gains peaking at 12–15 minutes of vibration stimulus per session (Marin and Rhea, 2010).
Studies from the last decade have reported that altering the intramuscular environment via hypoxia could be used as a method to enhance the physiological experience of resistance training (Scott et al., 2014). In response to resistance exercise in hypoxia, anaerobic metabolism is activated (Scott et al., 2016), increasing the metabolic stress (Ko et al., 2017; Ramos-Campo et al., 2017a) and, as a consequence, the recruitment of motor units (Scott et al., 2017). Therefore, the increase of muscle strength under hypoxic conditions could be mediated by hypertrophic adaptations (Scott et al., 2014) and/or neural adaptations (Inness et al., 2016). Thus, these benefits could be achieved with lower volume programs on strength and muscular mass. On a related note, strength training under systemic hypoxia also causes a greater increase in skeletal muscle, vascular endothelial growth factor and capillarization, which may potentially lead to increased muscular endurance (Kon et al., 2014), but little research has paid attention to the effects of exercise under hypoxia on muscular endurance and muscle fatigue.
Therapeutic benefits of hypoxic training have been suggested for clinical populations, such as the elderly who could suffer musculoskeletal impairments (Millet et al., 2016). Development of exercise in an environment with lower oxygen availability could enhance the physiological experience of training (Scott et al., 2014). In this sense, cyclic hypoxic training may contribute significantly to improvements in exercise capacity of elderly adults, being a safe and noninvasive strategy (Bayer et al., 2017). A previous study that combined additional exposure to hypoxia and strength endurance training augmented the positive effects on quality of life in the elderly, but the 18 sessions of this treatment were not enough to improve muscle strength (Schega et al., 2013). Conversely, walking at altitude has been shown to impair cognitive performance and postural stability during short exposures of a few hours (Stadelmann et al., 2015). On the contrary, previous studies have also shown a substantial loss of fat-free mass after 8 weeks of stay in Everest (Wandrag et al., 2017) and that the modest altitude could spare lean muscle mass (Palmer and Clegg, 2014). Despite these potential benefits, evidence for greater muscle strength gains and structural physiological changes in response to resistance training under hypoxic conditions is not conclusive (Feriche et al., 2017). Differences in the nature of hypoxia (normobaric or hypobaric hypoxia), such as training intensity (light or moderate loads), number of sets (3–6), rest period between sets (30–180 seconds), muscles worked (arms, legs, or chest), training program duration (4–8 weeks), training frequencies (2–3 sessions per week), total sessions (10–24), and severity of hypoxia (from 12% to 16% fraction of inspired oxygen [FiO2]), may have modified the strength adaptations observed (Feriche et al., 2017; Ramos-Campo et al., 2017c).
To the best of our knowledge, there are no studies in the scientific literature that investigate the effects of WBV training in hypoxia on the muscle strength parameters of an elderly population. So, the aim of the present study was to identify if 18 weeks of WBV training combined with exposure to normobaric cyclic hypoxia (CH) could cause higher increases in the strength parameters and muscle mass of elderly people (age >65 years) than WBV performed in normoxia.
Materials and Methods
Participants
The voluntary participation of elderly subjects was requested by letter and verbal communication in senior universities and local pensioners associations. Inclusion criteria, assessed during a screening visit, were as follows: (1) women and men aged 65 years or older, (2) absence of participation in any other type of intervention based on physical exercise in the last 6 months, (3) subjects have not been above 1500 m during the last 3 months, and (4) subjects did not have any current medical condition for which exercise was contraindicated. Exclusion criteria were mainly based on contraindications for WBV (severe cardiovascular disease, ocular disease affecting the retina, neuromuscular and heart diseases, stroke, implant, bypass, stent, arthritis and other joint disease, or epilepsy) or a frequency of participation in the stipulated program lower than 80% (participants who missed more than 20% of training sessions were excluded).
Forty-six volunteers (13 males and 33 females) were informed of the study procedures and were requested to sign a consent form to participate in this research. The eligible volunteers, who met the inclusion criteria, were randomly divided into three groups: (1) hypoxic whole-body vibration group (HWBV; n = 14), who performed WBV treatment under normobaric hypoxic conditions; (2) normoxic whole-body vibration group (NWBV; n = 14), who performed WBV treatment under normoxic conditions; and (3) control group (CON; n = 15), who were instructed to continue with their normal daily activities for the duration of the study. Four participants of the HWVB group, three from the NWBV group, and five participants from the CON group dropped out because of prolonged illnesses or personal reasons during the training period (Fig. 1). The study design was approved by the Bioethical and Biosecurity Commission of the University of Extremadura (17/2016).
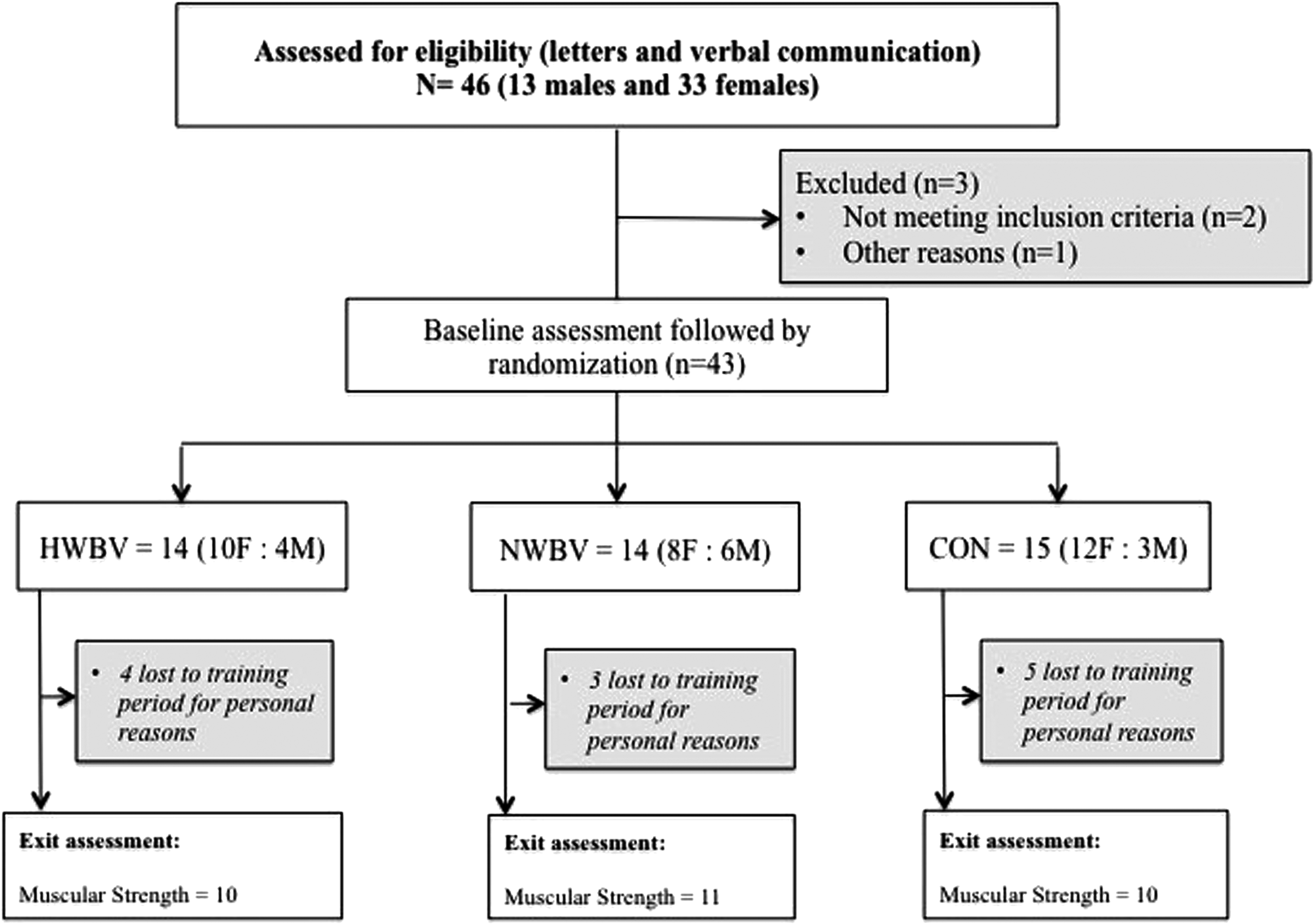
Flow of participants through each stage of the trial. CON, control group; F, female; HWBV, hypoxic whole-body vibration group; M, male; NWBV, normoxic whole-body vibration group.
Procedures
This was a randomized double-blind control study. There were separate intervention and assessment teams. We blinded the study at the participants; they were not informed of the study's hypothesis and were trained/tested separately. Over 18 weeks, the volunteers completed 36 training sessions supervised by an experienced member of the research group. The frequency of training was twice a week; sessions were scheduled with at least 1 day of rest in between for optimal recovery. All patients were assessed at two time points by a group of researchers who were blinded to the treatment assignment. Outcomes were measured at baseline (pre-) previous to the 18 weeks of intervention and reassessed 7 days after the last session (post-). Participants were instructed to maintain the absence of participation in any other type of physical exercise during the duration of this trial.
Training protocol
During sessions, the HWBV and NWBV groups performed the vibration exercise in a standing position with feet side by side on a specific landmark on the board, while barefoot to eliminate any damping of the vibration caused by footwear. The angle of flexion of the knee during the vibration exercise was set at 120°. The participants were allowed to hold the vibration platform with their hands for postural control. The vibration stimulus (12.6 Hz) was produced by a sinusoidal vibration platform (Galileo 2000; Novotec GmbH, Pforzheim, Germany), and the distant position formed by the axis of rotation was 4 mm peak-to-peak. The effective acceleration was 2.54 g force (g represents the Earth's gravitational acceleration at 9.81 m/s2). Subjects performed four sets of 30 seconds of vibration per session, separated by 60 seconds of rest. The total duration of the training session was about 16 minutes, which included a 10-minute warm-up with 5 minutes bicycling at 25–50 W and 40–50 rpm and another 5 minutes of stretching exercises. All these took place in a hypoxia chamber (CAT 310, Louisville, CO) placed in the laboratory.
For safety reasons, the FiO2 in the HWBV group was set at 16.1% to simulate an altitude of 2500 m above sea level (Millet et al., 2016); FiO2 was controlled regularly with an electronic device (HANDI+; Maxtec, Salt Lake City, UT). To blind subjects to altitude, the system was also run for the NWBV group with normoxic airflow into the chamber (up to 1000 L/min) and produced the same audible noise as in the hypoxic condition. NWBV subjects inspired an FiO2 of 21.0% to simulate an altitude of 459 m above sea level. Furthermore, all systems were covered with fabric to prevent participants from visually identifying the normoxic or hypoxic conditions.
At each session, the oxygen saturation (SpO2) was measured using a finger pulse oximeter (Konica Minolta, Japan) and heart rate (HR) using a HR monitor (Polar Team 2, Polar, Finland) to know the physiological challenges posed on the participants at different times of the session. The above parameters were controlled during the 2nd minute of the warm-up (warm-up), previous to the start of the WBV protocol (pretraining), between the second and the third set of the WBV protocol (mid-training) and after the WBV protocol (posttraining).
Outcome measures
Sociodemographic data and lifestyle questionnaires
A general questionnaire was administered to collect medical and demographic data to check the inclusion/exclusion criteria. As control variables, calcium intake and alcohol were estimated by using a food frequency questionnaire adapted to Portuguese traditional foods and dishes (Ribeiro et al., 2006). The bone-specific physical activity questionnaire was used to assess the physical activity level of the participants. Respondents recorded type, frequency, and years of physical activity involvement to assess the effects of mechanical loading on the skeleton.
Muscle strength assessment
Isokinetic leg muscle strength was evaluated using a Biodex isokinetic dynamometer (System-3; Biodex, NY) by performing unilateral tests in the right leg. Each subject was attached to the seat of the dynamometer so that the axis of their knee coincided with the axis of the dynamometer, following standardized protocols. The procedure of the test was explained to all subjects before placing special emphasis on exerting maximal effort within each individual's tolerance threshold. At the start of each single test, the subject was asked to relax his/her leg to determine the effect of gravity on the limb. Testing was performed using a hard deceleration cushion. The motion ranged from 80° of knee flexion to full extension. Participants rested for 2 minutes between each trial. First, the maximal strength test was measured by performing a three-repetition unilateral test of knee extension (Ext)-flexion (Flex) (concentric/concentric) at 60°/s. To analyze the strength balance between the hamstrings (H) and quadriceps (Q), the H/Q ratio was calculated as the quotient between peak torque (PT) values of the Flex and the Ext (PTFlex/PTExt). Endurance strength was evaluated through a 20-repetition unilateral test of knee Ext-Flex (concentric/concentric) at 180°/s. Mean work (Wmean) was calculated from the recorded force curves of these series of exercises for each direction of movement. Muscle fatigue was determined in terms of the relative change in mechanical work (W) between the first and the last third of the repetitions: [(Wfirst–Wlast)/Wfirst] × 100.
Body composition
Height (0.1 cm, SECA 769; seca gmbh & co.kg, Hamburg, Germany) and body mass (0.1 kg, SECA 769; seca gmbh & co.kg) were measured through recommended standardized techniques. Body mass index (BMI) was determined by the accepted method (BMI = weight/height2 [kg/m2]). Percentages of lean mass were obtained with dual-energy X-ray absorptiometry (DXA, Norland Excell Plus; Norland, Inc., Fort Atkinson, WI). The same experienced technician performed all the scans.
Statistical analysis
Statistical analyses were carried out with the statistical analysis software SPSS v.20 for Mac (IBM, NY). The compliance for the subjects who completed the 18 weeks of training was calculated as the number of sessions completed divided by the 36 possible sessions available per participant. Standard statistical methods were used for the calculation of the mean, standard deviations. Kolmogorov–Smirnov tests were conducted to show the distribution of the studied variables and Levene's test for homogeneity of variance. Before training, chi-squared tests and one-way analysis of variance (ANOVA) were used to determine whether differences existed between groups. Upon completion of the training period, mixed factorial ANOVA was performed, thereby taking into account the interaction between group, time, and sex, with adjustments made for age. The effect size was calculated for all variables between baseline and after 18 weeks of training. The resulting magnitude of change was considered trivial (<0.5), small (0.5–1.25), moderate (1.26–1.99), or large (>2.00). The p < 0.05 criterion was used for establishing statistical significance.
Results
Participant characteristics
The characteristics of the subjects (n = 31) at baseline are presented in Table 1. No significant pretraining differences were observed between the groups for any variable. The compliance with training prescription was 100% in the NWBV group and 91.39% in the HWVB group. None of the dropouts left the program as a result of injuries or adverse responses to the training. Because of the neutral smell of the conditioned air, subjects could not tell if they were in a hypoxic or normoxic environment. Blinding was successful, as more than 60% of subjects guessed their group incorrectly.
Descriptive Characteristics of the Participants
Values are given as the mean ± SD. p-Values of the ANOVA.
Values expressed as n (%). p-Values of chi-square analysis.
ANOVA, analysis of variance; CON, control group; BMI, body mass index; HWBV, hypoxic whole-body vibration group; NWBV, normoxic whole-body vibration group; SD, standard deviation.
Control training
SpO2 was lower (p < 0.01) for the hypoxia groups in all measured points during the training sessions. HR during the training sessions was not significantly different between groups (Fig. 2).

Physiological challenges of
Muscle strength
Results of maximal and endurance strength are summarized in Table 2. Because responses to the training showed no sex differences, the results for male and female participants were analyzed together as aggregate data. There were no significant differences between groups in either maximal or endurance strength after 18 weeks of training. In-group analysis showed no significant differences in any of the variables of the HWBV group. The NWBV group showed significant improvements in the maximal strength of knee extensors with a small effect size (p = 0.004; d = 0.54). The H/Q ratio of the NWBV group decreased with a small effect size after 18 weeks of training (d = 0.58).
Maximal and Endurance Strength at Baseline and After 18 Weeks of Normoxia Whole-Body Vibration Exercise (n = 11) of Combined Hypoxia Whole-Body Vibration Exercise (n = 10) and in the Control Group (n = 10)
Values are given as the mean ± SD.
Significant differences between pre- to post- (p < 0.05).
Δ, absolute change (post- minus pretraining absolute change); Endurance strength, 20-reps for 180°/seconds; Fatigue, muscle fatigue as % of Δ in20-reps; Fmax, maximal force; H/Q ratio, hamstring-quadriceps ratio (maximal strength flexor/maximal strength extensor); Maximal strength, 3-reps for 60°/second; Wmean, average work.
Body composition
Whole-body percentages and trunk and right leg lean masses are presented in Table 3. Because responses to the training showed no sex differences, the results for male and female participants were analyzed together as aggregate data. There were no significant differences between groups for any of the three variables. In-group analysis did not show any significant differences in any of the variables among groups (the HWBV, NWBV, nor CON groups). Effect sizes were trivial in all body composition parameters.
Body Composition Parameters at Baseline and After 18 Weeks of Intervention
Values are given as the mean ± SD.
Discussion
The aim of the study was to determine the effects of 18 weeks of WBV training combined with exposure to normobaric CH on strength parameters in elderly people (age >65 years). The findings of this study reject the aforementioned hypothesis with respect to the combination of WBV training and CH exposure, as this new treatment did not have any effect on maximal or endurance strength parameters.
Previous studies have shown that strength training in hypoxia seems to cause functional adaptations in skeletal muscle (Lundby et al., 2009). Moderate hypoxia (13%–16% FiO2) increases the metabolic stress that is caused by the exercise performed under hypoxic conditions (Kon et al., 2012; Ramos-Campo et al., 2017a, 2017b; Scott et al., 2017). Increased motor unit recruitment has been reported after strength training in hypoxia, which stimulated a larger portion of the muscle during exercise (Scott et al., 2017). However, in the elderly, hypoxia could be ineffective with regard to strength-endurance measurement, and strength training may go beyond the effect of hypoxia (Levine, 2002). In a study by Schega et al., 2013, a group of elderly adults was supplied with intermittent hypoxic training before a strength-endurance exercise program. Analyzing the strength-endurance capacity, there were no significant differences between the intermittent hypoxic training group compared with the control group. It is also possible that a high level of hypoxia may result in performance decrements during training, which could limit any hypoxia-mediated benefits derived from such training (Scott et al., 2016). Ramos-Campo et al. (2017a) reported lower muscle performance during two sets of half-squat exercises due to limited oxygen availability.
When exercising in hypoxia, the decrease in oxygen availability increases the contribution of anaerobic metabolism rather than aerobic energy production (Bowtell et al., 2014). An increase in intracellular acidosis due to glycolytic pyruvate production results in higher concentrations of blood lactate, which may contribute to muscular fatigue (Bowtell et al., 2014) and a decline in performance (Balsom et al., 1994). In addition, limited oxygen availability and brief rest intervals affect the muscle's ability to maintain the balance between adenosine triphosphate (ATP) breakdown and ATP production, thereby limiting cellular recovery after each exercise set (Hogan et al., 1999). In the present study, SpO2 was significantly lower in the HWBV group when compared with the NWBV group during all training sessions. Decreases in SpO2 during the four sets of WBV training in hypoxia could be associated with greater anaerobic energy production (Alvarez-Herms et al., 2015). Thus, strength performance in the HWBV group could be due to an inadequate supply of ATP to meet the demand of vibratory exercise with the resulting accumulation of metabolic products and ionic imbalance (Scott et al., 2017), which in turn involves higher levels of muscular fatigue and a decrease in voluntary effort during the training. Previous studies suggest that resistance training in hypoxia was perceived as more difficult than in normoxia (Alvarez-Herms et al., 2015; Ramos-Campo et al., 2017a). Therefore, it has been observed that the training protocol and the level of hypoxia used during the strength sessions could cause different adaptations (Scott et al., 2016; Ramos-Campo et al., 2017a). In addition, the specific work/rest ratio and the accumulated volume to achieve metabolic overload could also be dependent on the prior training status of each individual (Scott et al., 2016). Participants in the present study were untrained elderly people, so the combination of WBV training and exposure to hypoxia may have provoked high stress during the session, which could limit their capacity for improvement.
In the present study, the participants who underwent WBV training under normoxic conditions significantly increased the maximal strength of knee extensors. Consequently, a decrease in the H/Q ratio in this group was shown after 18 weeks of WBV training alone. However, WBV training had no effect on body composition, as it was expected due to the results reported in previous studies (von Stengel et al., 2012). A recent meta-analysis about the effects of WBV training on lean mass demonstrated that this could lead to improvement in lean mass or muscle mass in younger adults, but not in other populations (Chen et al., 2017). Therefore, neuronal mechanisms may predominantly contribute to the observed strength gains in the NWBV group. WBV training consists of two components: reflex muscle contraction induced by the vibration stimulus and the unloaded exercises performed on the platform (Roelants et al., 2004; Rees et al., 2007). This method of training generates simulated mechanical vibrations, activates the neuromuscular control system, increases the level of excitement and the number of motor units recruited, and coordinates synergistic and antagonistic muscles during rapid muscle contractions, thus enhancing muscle function (Delecluse et al., 2003).
The intervention has to last for at least 8 weeks to improve muscle strength (Mikhael et al., 2010) and the volume must be set at around 12–15 minutes of vibration per training session to obtain maximum gains (Marin and Rhea, 2010). Longer and/or more intensive WBV exercise sessions might result in higher motor unit activation, thus achieving better training effects (Delecluse et al., 2003). Also, it appears that the vibration stimulus, while standing with bent knees or squatting on a platform, may exhibit nonlinear adaptations in strength (Rees et al., 2007). Therefore, the standing position, which was adopted on the platform in this study, only allowed the improvement of knee extensor strength, which might have resulted in the strength imbalance between knee extensors and flexors. Adding dynamic exercises (such as deep squats or wide stance squats) to traditional standing with bent knees may facilitate the delivery of vibration to the muscles that would not have been otherwise stimulated (Delecluse et al., 2003; Rees et al., 2007). Although further research is necessary to ascertain this, WBV training, including dynamic exercises, could potentially benefit mobility and functional performance in an older population.
A limitation of the present study was the different characteristics of the open-chain approach of isokinetic testing versus the closed-chain one of the WBV exercises (squat positions). Although some studies have reported on the relationship between isometric and isokinetic strength measures and other functional measures (Burnfield et al., 2000; Broekmans et al., 2013), their validity in isokinetic measuring tests is not conclusive. On the contrary, metabolic stress markers, such as blood lactate concentrations, cortisol or muscle deoxygenation (Formenti et al., 2018) were not measured, which could have offered more information about the metabolic stress during WBV training in hypoxia. Finally, results were obtained in the context of an 18-week trial, and the long-term clinical effects remain unknown. Other authors proposed that between 2 and 90 days and most long-lasting protocols on consecutive or alternating days could be necessary to achieve potentially beneficial effects (Navarrete-Opazo and Mitchell, 2014). However, as intervention length remains unclear, an intermediate and detraining measurement might be appropriate to understand kinetic changes.
Conclusion
In conclusion, the combination of WBV training and exposure to CH did not cause any effect on maximal or endurance strength parameters. This finding suggests that the work/rest ratio and the accumulated volume could be important factors when untrained elderly people are subjected to WBV training in hypoxic conditions. High stress during the session could limit their capacity for improvement.
Further research has to be carried out to determine the most effective training program in hypoxia to improve muscular strength parameters in an elderly population.
Footnotes
Acknowledgments
The project has been supported by the Government of Extremadura with funding from the European Regional Development Fund under Grant (Ref: GR18003); and the Ministry of Education, Culture and Sports, under Grant FPU15/00450 and FPU15/00452.
Author Disclosure Statement
No competing financial interests exist.