
Abstract
Abstract
Background:
We compared acute psychophysiological responses with a single intermittent hypoxic exposure (IHE)/normoxic exposure trial with varying cycle lengths in adults with obesity.
Materials and Methods:
Eight obese adults (body mass index = 33.0 ± 2.2 kg/m2) completed three 60-minute IHE trials (passive seating), separated by 7 days. Trials comprised 30-minute hypoxia/30-minute normoxia (inspired oxygen fraction = 12.0%/20.9%) over Short (15 × 2/2 minutes), Medium (10 × 3/3 minutes), and Long (5 × 6/6 minutes) hypoxic/normoxic cycles and a control trial (60-minute normoxia).
Results:
Arterial oxygen saturation was lower during hypoxic periods of Long versus Medium and Short trials (90.1% vs. 93.0% and 94.2%; p = 0.02 and p = 0.05), with no differences between Short and Medium. Prefrontal cortex oxygenation was lower (−5.1%) during all IHE interventions versus control (p < 0.02), independent of cycle length. Perceived breathlessness was unaffected during IHE but increased 15 minutes after exposure versus baseline (+34%; p = 0.04). Breathlessness was lowest after Short versus control from 15 to 60 minutes (−7%; p = 0.01).
Conclusions:
When implementing IHE, greater desaturation is observed during longer compared with shorter hypoxic/normoxic cycles in adults with obesity. However, IHE tends to be better tolerated perceptually with shorter rather than longer cycles.
Introduction
In the United Kingdom, ∼26% of adults are overweight (body mass index [BMI] = 27–29.9 kg/m2) and ∼35% obese (BMI = 30–40 kg/m2) (Baker, 2018). In addition to exacerbated weight-bearing (Wearing et al., 2006), obesity is associated with negative health conditions, such as hypertension (Hall et al., 2015) and type II diabetes (Toplak et al., 2016). To reduce body weight and improve health in obese populations, lifestyle interventions (i.e., dietary manipulation, physical activity) have been implemented, yet with low adherence and success (Forman and Butryn, 2015). Therefore, there is an urgent need for new strategies to reduce obesity prevalence and improve the health and well-being of this population. One innovative strategy evidencing therapeutic benefits in this demographic is passive hypoxic exposure (Urdampilleta et al., 2012; Verges et al., 2015; Hobbins et al., 2017).
Normobaric hypoxia is defined as a reduced/insufficient oxygen supply (lower inspired oxygen fraction or FiO2) to tissues leading to decreased arterial oxygen saturation (SpO2) (Heinonen et al., 2016). Workman and Basset (2012) found increased energy expenditure in overweight males immediately following one continuous resting 3-hour session at a target SpO2 of 85% versus normoxia. However, continuous hypoxic exposure (several hours) versus normoxia may exacerbate sympathetic nervous system activity, raising the risk of elevated blood pressure, tachycardia, and rate pressure product in “at-risk” individuals (White et al., 1985; Wulsin et al., 2018).
Intermittent hypoxic exposure (IHE) includes cycles of hypoxia and normoxia lasting from a few minutes to hours (Urdampilleta et al., 2012). Decreased cerebral oxygenation and blood pressure, during and immediately after one ∼1-hour IHE session, were found in healthy and overweight individuals versus a normoxic baseline (Chacaroun et al., 2017; Costalat et al., 2018). Although positive physiological responses have been reported, the aforementioned studies utilized individually tailored hypoxic intervals (∼5 minutes) to reach a target SpO2 (∼75%), rather than replicable standardized hypoxic/normoxic cycles. Currently, no consensus regarding best practice IHE (i.e., optimal cycle length and frequency) for maximizing physiological responses primarily exists for implementation in adults with obesity.
Between 3 and 15 cycles per session of moderate hypoxia (FiO2 = 9.0%–16.0%) are suggested to reduce blood pressure and increase blood glucose tolerance (daily sessions over 4 weeks) (Naverrete-Opazo and Mitchell, 2014). Evidence from animal studies indicates that longer less frequent cycles will induce higher physiological (i.e., tissue deoxygenation) stress versus shorter more frequent cycles (Almendros et al., 2014). However, this is currently unknown in regard to obese individuals completing IHE for beneficial psychophysiological responses.
Perception is a necessary component for investigating behavior changes toward health (Schutzer and Graves, 2004). Stavrou et al. (2018) reported impaired mood state (i.e., greater depression and tension) during a 21-day hypoxic bed rest (FiO2 = 15.0%) versus normoxia. To date, there is a lack of data including perceptual measures during and following (∼60 minutes) IHE. A low level of enjoyment is commonly cited as a reason for low/nonadherence to lifestyle interventions (King et al., 1988). Therefore, it is relevant to assess perception during IHE and potential influences of different cycles. Although exercise-based, studies have found lower perceived exertion when SpO2 is >94% during hypoxic exercise versus <94% (Romer and Dempsey, 2006; Khaosanit et al., 2018). For IHE, perhaps more frequent reoxygenation phases during shorter versus longer hypoxic cycles will permit more positive perception as SpO2 will likely increase during normoxic cycles (Urdampilleta et al., 2012).
The aim of this study was to therefore compare the acute effects of 60-minute IHE sessions including short, medium, and long hypoxic/normoxic exposure cycles (matched total hypoxic and normoxic exposure time) versus a control on the magnitude and time course of psychophysiological responses. We hypothesized that the physiological stimulus (i.e., tissue deoxygenation) would be greater, yet with less favorable perceptual responses (i.e., perceived breathlessness), during longer versus shorter cycles, with medium being the “optimal” trade-off.
Materials and Methods
Participants
Eight adults with obesity (five women, three men; age: 37.0 ± 11.1 years; height: 169.8 ± 0.1 cm; weight: 93.9 ± 8.7 kg; BMI: 33.0 ± 2.2 kg/m2; systolic and diastolic blood pressure: 117.4 ± 18.3 and 70.6 ± 11.4 mmHg, respectively) were recruited. Participants were enrolled into the study following the eligibility assessment that consisted of having a BMI of 30–40 kg/m2, being normotensive (90–120 and 60–80 mmHg systolic and diastolic blood pressure, respectively), no known cardiovascular, metabolic, or physiological illness/disease, sedentary (<1 hour of moderate-intensity exercise/week), and no exposure to altitude (≥2500 m) for >48 hours within 6 months. Written informed consent was obtained from all participants. This study was carried out in accordance with the Declaration of Helsinki. Ethical approval was received from the School of Applied Sciences Ethics Committee, London South Bank University (SAS1705).
Experimental design
Participants attended the laboratory on five separate visits. First, they were familiarized with the study, including procedures/measures involved, and eligibility was determined. Eligible participants returned on four occasions at a similar time of day for the main experimental trials, each separated by 7 days to enable a washout period (Kelly and Basset, 2018). Each experimental trial included a 60-minute intervention, three of which included 30-minute hypoxia (FiO2 = 12.0%) and 30-minute normoxia, and one in continuous normoxia (control) completed in a randomized order. The cyclic interventions were (i) 15 × 2/2 minutes (SHORT), (ii) 10 × 3/3 minutes (MEDIUM), and (iii) 5 × 6/6 minutes (LONG) in hypoxia/normoxia. All trials included a 60-minute postintervention period (normoxia). Participants arrived at the laboratory following an 8-hour fast but were permitted to consume water. Participants were asked to replicate their dietary intake for remaining trials after the first (24 hours prior) and continue their habitual routine during their time spent enrolled on the study.
Intervention
Figure 1 illustrates the intervention. Participants rested in a seated position for 10 minutes to enable hemodynamic stabilization (Thijssen et al., 2011). Baseline assessment of blood pressure and perception was made. Participants were fitted with an “intervention” facemask, which provided exposure to hypoxic/normoxic gas for 60 minutes. Perception was assessed at 0 (T0), 10 (T1), 22 (T2), 34 (T3), 46 (T4), and 58 (T5) minutes (corresponding to 0%, 20%, 40%, 60%, 80%, and 100% of the 60-minute intervention) in normoxia. Arterial and brain oxygenation was recorded throughout the intervention. The “intervention” facemask was removed after 60 minutes, and blood pressure and perception were reassessed at 15, 30, and 60 minutes after the intervention. Entertainment (films/television programs with similar neutral content across trials) was provided during the intervention.

Overview of the 60-minute intervention completed during each experimental trial. Participants were passively exposed to hypoxia (colored bars) interspersed with exposure to normoxia (white bars). The time spent in hypoxia and normoxia per intervention was 30 minutes, achieved via different cyclic variations: 2/2 minutes (Short; black bars), 3/3 minutes (Medium; dark gray bars), and 6/6 minutes (Long; light gray bars). An additional control trial involving continuous exposure to normoxia was also completed. Measurements were taken in normoxic conditions at 0 (T0), 10 (T1), 22 (T2), 34 (T3), 46 (T4), and 58 (T5) minutes, as denoted by the arrows.
Hypoxic simulation
Participants wore a facemask (Altitude Training Mask; Hypoxico Altitude Training Systems) connected via corrugated plastic tubing to a hypoxic generator (Everest Training Summit II; Hypoxico Altitude Training Systems) to simulate hypoxia. The FiO2 provided was 12.0% (simulated altitude of ∼4500 m), deemed safe in the population studied (Naverrete-Opazo and Mitchell, 2014). An additional hypoxic generator was set at a 20.9% FiO2 for normoxic cycles, both outside of participant viewing, for blinding. A Hans Rudolph two-way valve positioned along the corrugated tubing permitted switching between gases. Participants' remained seated at all times during the intervention and instructed to maintain a normal breathing pattern by the investigator (“breath as normally as you would without wearing a facemask”) before each trial.
Physiological measures
A pulse oximeter (Nellcor N-200E Pulse Oximeter; Medtronic) attached to the participants' index finger continuously estimated SpO2 (%) during the 60-minute intervention.
Near-infrared spectroscopy bipolar optode sensors (NIRO-2000NX; Hamamatsu, Japan) attached via double-sided adhesive tape and housed (3 cm apart, 775 Nm wavelength) within rubber-cased hoods assessed oxygenation via tissue saturation index (TSI; %) of the left prefrontal cortex. Probes were placed over the left prefrontal cortex to illuminate cortical area between standard Fp1 and F3 locations according to the international EEG 10–20 system (Chacaroun et al., 2017). TSI was calculated via emission and absorption of near-infrared light to tissue, in accordance with the Beer–Lambert law. The data signal was arbitrarily set to zero via internal factory settings. SpO2 and TSI data were continuously sampled during the 60-minute intervention at 10 Hz (Chacaroun et al., 2017) and recorded into Spike2 (v8; CED, England).
Blood pressure was assessed by attachment of a pressure cuff secured with Velcro around the participants' biceps. The cuff was inflated to 170 mmHg and deflated alongside pulse rate (Omron M4; Omron, Japan). Systolic and diastolic values were recorded following the assessment at baseline and 15, 30, and 60 minutes after the intervention. A single measurement was completed unless there was uncertainty in the values (due to machinery error) by the investigator (Beevers et al., 2001).
Perceptual measures
Perceived mood state, breathlessness, and motivation to exercise were assessed at baseline, T0–T5, and 15, 30, and 60 minutes after the intervention. Participants were asked “How are you feeling right now?”, “How breathless do you feel right now?” and “How motivated do you feel to complete exercise right now?” by the investigator. Participants were instructed to verbally specify a number on an 11-point scale anchored “very bad” (−5) up to “very good” (+5) for mood state (Hardy and Rejeski, 1989), a 12-point scale anchored “nothing at all” (0) up to “very, very severe” (10) for breathlessness (Ward and Whipp, 1989), and to adjust a 20 cm visual analog scale anchored “extremely low” (1) up to “extremely high” (20) for motivation (Crewther et al., 2016). Positive and negative affects were assessed via a 20-item 5-point Likert scale at baseline and 15, 30, and 60 minutes after the intervention. Participants were instructed to answer how they feel toward 20 emotions including “interested”, “distressed,” and “excited”, ranging from “very slightly or not at all” (1) to “extremely” (5). Items were totaled for positive and negative responses (Watson et al., 1988) and the ratio between the two (Diehl et al., 2011). Scale order presentation was held constant across time points and participants.
Data analysis
Data were processed offline into Excel (Microsoft Office, 2016). SpO2 data were averaged for time in hypoxia (30 minutes) and normoxia (30 minutes) for each IHE condition, and 60 minutes of normoxia for control. TSI data samples (2 minutes) were exported in hypoxia (before T1–T5) to compare an equal hypoxic duration between conditions at matched time points. Perceptual data were obtained in normoxic conditions to allow meaningful comparisons between IHE cycle variations and the control trial, all under normoxic conditions. TSI data were smoothed using a five-point moving average and truncated via removal of the first and last 30 seconds of each 2-minute (T0–T5) data collection period (1 minutes). TSI data were normalized by calculating the percentage change from T0 (in normoxia) in each respective condition for statistical analysis, due to possible sensor placement differences. Perceptual data collected during the 60-minute intervention and postintervention periods were expressed as percentage change from T0 and baseline, respectively.
Statistical analysis
Data distribution was assessed via the Shapiro–Wilk normality test. Normally distributed data were analyzed with a parametric two-way analysis of variance, aligned with the Sidak confidence interval adjustment, to investigate the main effects of condition (SHORT, MEDIUM, LONG vs. control), time (during intervention: T0, T1, T2, T3, T4 vs. T5; after intervention: baseline, 15, 30 vs. 60 minutes postintervention), and the condition × time interaction for TSI, blood pressure, and perceptual responses. SpO2 data were compared for main effect of condition (SHORT, MEDIUM, LONG vs. control) and environment (hypoxia vs. normoxia). Sphericity was assessed via the Mauchly test, if violated, the Greenhouse Geisser correction was applied. Partial eta-squared was calculated as an estimation of effect size (ES). Values of 0.01, 0.06, and >0.14 were considered as small, medium, and large, respectively (Cohen, 2013). If data were nonnormally distributed, a related sample of nonparametric Friedman's test was used. If any significant effects were found, further post hoc analysis was carried out via pairwise comparisons to assess where the significance lay. Statistical testing was carried out in SPSS (v21; IBM, Cambridge). Data are presented as mean ± standard deviation and considered statistically significant if p ≤ 0.05 and a trend for significance if p ≤ 0.07. Perceptual data are presented as raw values if statistical significance was not reached for context.
Results
Responses during IHE
Physiological measures
SpO2 was lower during SHORT, MEDIUM, and LONG hypoxic versus normoxic cycles (−6%; p < 0.001, F = 32.351, ES = 0.822; Fig. 2). Pairwise comparisons revealed that SpO2 during hypoxic LONG cycles was lower versus MEDIUM (−3%; p = 0.023) and SHORT (−4%; p = 0.054; Fig. 2).

Arterial oxygen saturation (SpO2) during the intervention. Values are presented as mean ± SD during hypoxic and normoxic periods (average of 30 minutes) for Short, Medium, and Long, and average of 60 minutes for control. Short = 2/2 minutes; Medium = 3/3 minutes; Long = 6/6 minutes. “*” Denotes a statistically significant difference (p < 0.01) versus control; “” denotes a statistically significant difference (p = 0.03) versus normoxia for a given condition; “§” denotes a statistically significant difference (p = 0.05) versus Long. SD, standard deviation.
TSI decreased during SHORT (68.9 ± 3.6%), MEDIUM (69.1 ± 4.4%), and LONG (68.7 ± 5.3%) versus control (72.6 ± 4.9%; p = 0.009, F = 8.237, ES = 0.543; Fig. 3). Compared with T0, TSI from T1 to T5 was lower (−3%; p = 0.011, F = 6.107, ES = 0.543; Fig. 3). There was no interaction effect on TSI (p = 0.080, F = 2.997, ES = 0.300).
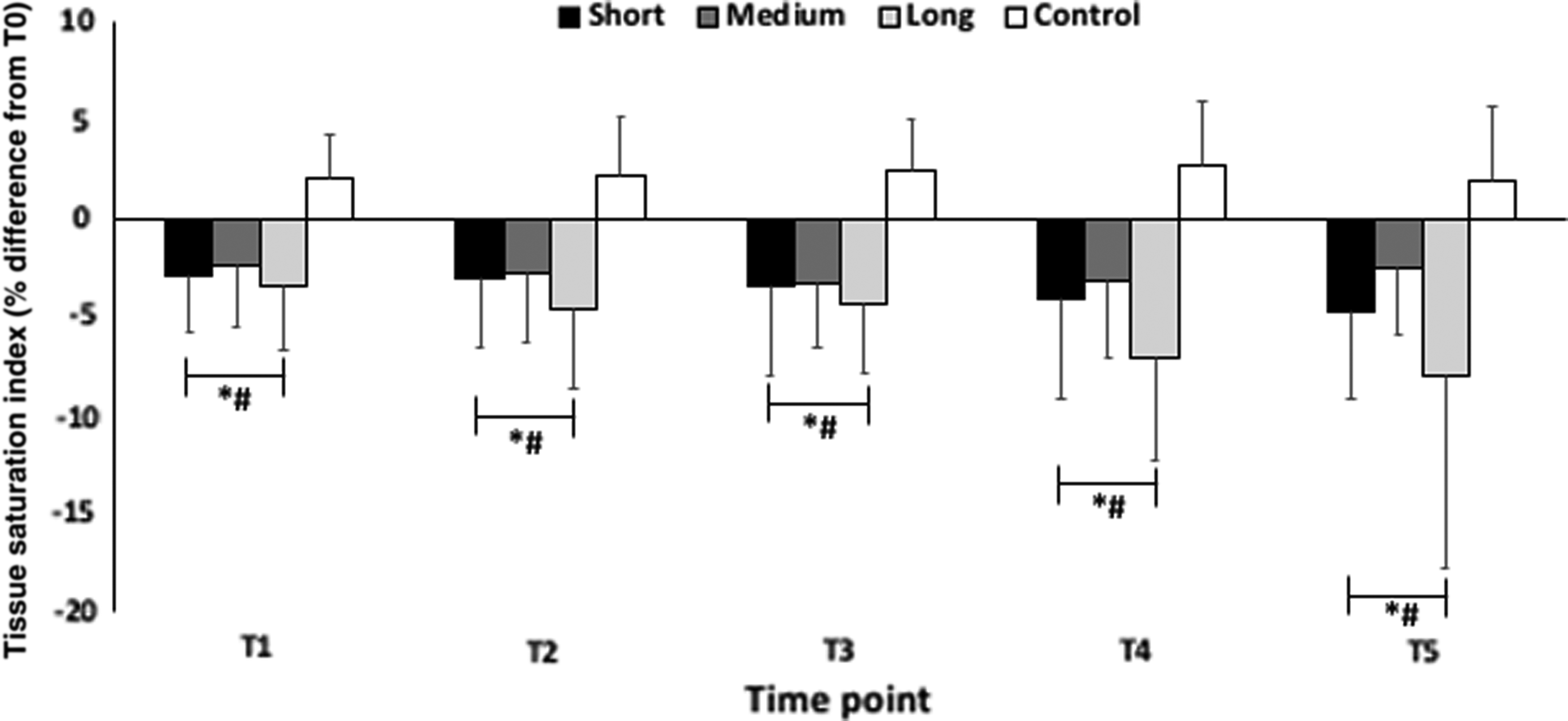
Tissue saturation index data of the prefrontal cortex measured during the intervention at 8 (T1), 20 (T2), 32 (T3), 44 (T4), and 56 (T5) minutes in hypoxia during Short, Medium, and Long cycles and in normoxia during control. T1–T5 values are calculated as a percentage difference from T0 and are presented as mean ± SD. Short = 2/2 minutes; Medium = 3/3 minutes; Long = 6/6 minutes condition. “*” Denotes a statistically significant difference (p < 0.01) versus control; “#” denotes a statistically significant difference (p < 0.01) versus T0.
Perceptual measures
No condition, time, or interaction effects were observed for perceived mood, breathlessness, and motivation to exercise during the 60-minute intervention (p ≥ 0.05; Table 1).
Perceptual Measures Recorded at 0 (T0), 10 (T1), 22 (T2), 34 (T3), 46 (T4), and 58 (T5) Minutes During Short, Medium, and Long Intermittent Hypoxic Exposure Interventions As Well As the Control Trial
Values are presented as group means ± SD. Short = 2/2 minutes; Medium = 3/3 minutes; Long = 6/6 minutes.
SD, standard deviation; ANOVA, analysis of variance.
Responses after IHE
Physiological measures
No condition, time, or interaction effects existed for blood pressure (p > 0.05; Table 2).
Physiological and Perceptual Measures Recorded at Baseline and 15, 30, and 60 Minutes Postintervention During Short, Medium, and Long Intermittent Hypoxic Exposure Interventions As Well As the Control Trial
Values are presented as group means ± SD. Short = 2/2 minutes; Medium = 3/3 minutes; Long = 6/6 minutes.
Perceptual measures
There was a significant effect of condition (p = 0.003, F = 6.617, ES = 0.486) and time (p = 0.001, F = 17.779, ES = 0.717), but no interaction (p = 0.146, F = 1.946, ES = 0.218; Fig. 4a) on perceived breathlessness. Pairwise comparisons revealed perceived breathlessness increased 15 minutes after the intervention versus baseline (+34%; p = 0.040; Fig. 4a). Breathlessness during SHORT was lower versus control 15–60 minutes after the intervention (p = 0.001; Fig. 4a). Furthermore, SHORT tended to be lower than LONG 15–60 minutes after the intervention (p = 0.06). Positive affect decreased from 15 to 60 minutes after the intervention versus baseline (p < 0.05) but was unaffected by condition (p > 0.05; Fig. 4b). Perceived mood state, motivation to exercise, negative affect, and the ratio between positive and negative affect were unaffected by condition and did not change over time (p > 0.05; Table 2).

Perceived breathlessness
Discussion
To the best of our knowledge, this is the first study to compare the acute psychophysiological responses to SHORT (15 × 2/2 minutes), MEDIUM (10 × 3/3 minutes), and LONG (5 × 6/6 minutes) cyclic variations of IHE. During one 60-minute (30 minutes of hypoxia/30 minutes of normoxia) IHE session, arterial and brain oxygenation decreases versus control, independent of cycle length. Compared with baseline, perceived breathlessness increased 15 minutes after IHE completion. This increase tended to be smaller following SHORT than LONG. When implementing IHE, greater desaturation is observed during longer compared with shorter hypoxic/normoxic cycles in adults with obesity. However, IHE tends to be better tolerated perceptually with shorter rather than longer cycles.
Responses during IHE
Physiological measures
We found that IHE decreased SpO2 (during hypoxic cycles) versus control. Furthermore, LONG (−7%) led to larger decreases than MEDIUM (−3%) and SHORT (−1%) versus normoxic cycles of each respective condition. Although the hypoxic duration was matched across IHE (30 minutes), the extent of SpO2 decrease is aligned with hypoxic/normoxic cycle length. This may be due to acute hypoxic exposure inducing a progressive decline in SpO2 (Botek et al., 2015) that is more evident in longer versus shorter cycles. SpO2 has been found to decrease continuously during exposure to hypoxia at rest (FiO2 = 9.6%) for up to 10 minutes versus a normoxic baseline in healthy individuals (−26%, 0–10 minutes) (Krejčí et al., 2018). However, SpO2 values during hypoxic cycles of IHE presented in the current study (SHORT = 94.2%; MEDIUM = 93.1%; LONG = 90.1%) may be considered clinically insignificant. Hence, SpO2 <90% has been defined as a state of hypoxemia (Basnet et al., 2006). To reach greater levels of desaturation (hypoxemic state) alone, it is likely that IHE protocols consisting of longer rather than shorter hypoxic/normoxic cycles would be recommended. Overall, cyclic variations of IHE impact on the subsequent decreases in SpO2, with longer cycles inducing lower values.
TSI of the prefrontal cortex decreased during all IHE cycles in reference to control. Here, we speculated that longer cycles of IHE would lead to larger decreases in prefrontal cortex oxygenation versus shorter cycles (Verges et al., 2012), but this was not the case. Rupp et al. (2016) reported decreases in prefrontal cortex oxygenation (−3%) and SpO2 (−9%) during 2-minute IHE cycles (FiO2 = 11.0%) for 45 minutes versus a normoxic baseline in healthy individuals, similar to the current study (TSI: −3%; SpO2: −5%). Chacaroun et al. (2017) also reported decreases in cerebral oxygenation (−6%) during IHE (7 × 5-minute hypoxia/3-minute normoxia) at a target SpO2 of 70%–80%. Overall, it seems that larger SpO2 decreases lead to measureable differences in prefrontal cortex deoxygenation. A greater hypoxic dose than that used in the current study (FiO2 = 12.0%) may have led to larger SpO2 decreases, and as such, prefrontal cortex oxygenation, during both SHORT and LONG. Notably, TSI decreases occurred and were maintained from T1 to T5 versus T0. It was previously stated that more than 30-minute continuous hypoxic exposure is required to obtain quantifiable decreases in TSI of the prefrontal cortex (Chacaroun et al., 2017). Under the present circumstances, IHE composed of varying hypoxic cycles totaling 30 minutes induced similar deoxygenation levels in the prefrontal cortex of adults with obesity, independent of cycle length, which was maintained for 60 minutes.
Perceptual measures
During IHE, no changes in perceived mood state, breathlessness, and motivation to exercise between IHE cycles were reported or versus control. During a 21-day bed rest in hypoxia (FiO2 = 15.0%), healthy individuals felt more depressed, tensed, and confused at days 14 and 21 versus baseline (normoxia) (Stavrou et al., 2018). Although IHE and bed rest are passive modalities, the negative affects during bed rest in combination with hypoxia are unlikely to occur during IHE due to reduced exposure duration and inclusion of normoxic cycles. It was previously reported that mood is negatively impacted during rest in continuous hypoxia (8 hours; FiO2 = 13.0%) versus baseline (normoxia) (de Aquino Lemos et al., 2012). Therefore, we anticipated that SHORT would likely lead to better overall perception. However, no perceptual differences were observed between conditions during IHE. This may be due to differences in exposure type (intermittent vs. continuous), duration (30 minutes vs. 8 hours), the hypoxic dose between studies (FiO2 = 12.0% vs. 13.0%), or little hypoxemia. We conclude here that perceptual responses during IHE are maintained with all tested cycle variations.
Responses after IHE
Physiological measures
Although with severe continuous hypoxic exposure (FiO2 <8.0%), elevations in blood pressure in humans and animals occur (White et al., 1985). Herein, we assessed blood pressure and found no differences between baseline and postintervention following IHE of a moderate hypoxic level (FiO2 = 12.0%). Previous studies have found normalized blood pressure in hypertensive patients following regular IHE (∼1- to 5-minute hypoxic/normoxic cycles, FiO2 = 10%–14%, daily for ∼60 minutes, 10–14 days) (Serebrovskaya et al., 2008). As there were no blood pressure assessments during IHE in the current study, we cannot support this evidence. No negative sympathetic nervous system activity effects are realized regardless of IHE cycle length and thus considered a safe therapy.
Perceptual measures
One unique finding includes greater perception of breathlessness 15 minutes after the intervention versus baseline, which tended to be exacerbated following LONG versus SHORT. We believe that this response occurred due to dyspnoeagenia, that is, an evoked respiratory exertion without increased physiological ventilation (Ward and Whipp, 1989). In adults with obesity, breathlessness is a symptom often felt during rest (Gibson, 2001), which may explain the increases in perceived breathlessness following control and IHE. Importantly, increases in perceived breathlessness tended to be smaller following SHORT and greater following LONG. In summary, shorter IHE cycles may be preferential over longer because of a marginal lowering in the magnitude of postintervention increases in perceived breathlessness after IHE.
Compared with baseline, positive affect was reduced 15–60 minutes postintervention in all conditions (including control). Stavrou et al. (2018) found reduced positive affect following a 21-day bed rest in hypoxic and normoxic conditions. Perceived mood state, motivation to exercise, and negative affect were maintained throughout IHE in the current study. As such, a reduced positive affect may not be due to hypoxia per se but the lack of activity over time (>3 hours). Although positive affect was reduced following the 60-minute intervention, it is unlikely that this was due to the effect of IHE, or in particular, cyclic variation.
Limitations and perspectives
The current study has several limitations. First, our sample size was small (n = 8) implying that our findings should be interpreted with caution. Conclusions from these data are made only from stage I obesity, which may differ to stage II and III, and between genders such as larger psychophysiological stress (Stengel et al., 2013). Second, we used one hypoxic dose (FiO2 = 12.0%) throughout IHE. Further studies should verify whether a more severe FiO2 (lower than that used in the current study) during longer hypoxic/normoxic cycles, which will likely maximize the desaturation achieved during IHE, does not lead to negative effects on perceptual responses. IHE combined with exercise may potentiate further positive responses, at least short-term, than IHE alone due to added physical activity. As such, chronic studies implementing 2-minute IHE (and exercise) cycles on a regular basis (3–4 times per week, over 4–6 weeks) (Hobbins et al., 2017), which are likely to improve aspects of health, are needed since the current study is acute-focused. The findings of this study shed some light on disregarded perceptual responses.
Conclusion
When implementing IHE, greater desaturation is observed during longer compared with shorter hypoxic/normoxic cycles in adults with obesity. However, IHE tends to be better tolerated perceptually with shorter rather than longer cycles.
Footnotes
Acknowledgments
The authors would like to thank the participants for the time and commitment to the study and Mr. Bill Anderson for technical advice and support.
Authors' Contributions
All authors contributed to the design on the study. L.H. was responsible for data collection, processing, and analysis. All authors contributed to production and revision of the article. All authors have reviewed and approved the final article before submission.
Author Disclosure Statement
No competing financial interests exist.