
Abstract
Abstract
Background:
Acetazolamide is the most common medication used for prevention of acute mountain sickness (AMS), usually administered the day or night before ascent. The objective of this study was to evaluate the efficacy of day of ascent dosing of acetazolamide for AMS prevention.
Methods:
Double-blind, randomized, controlled noninferiority trial of acetazolamide 125 mg twice daily beginning either the night before or the morning of ascent. Healthy low altitude adults ascended from 1240 m (4100 ft) to 3810 m (12,570 ft) during summer 2018 on White Mountain, California. Primary outcome was incidence of AMS with the two different dosing patterns, assessed by the 1993 Lake Louise Questionnaire (LLQ) of ≥3 with headache and a minimum of 1 for other symptom.
Results:
One hundred four participants completed the study, with 54 (52%) randomized to night before acetazolamide and 50 (48%) to day of ascent dosing, without differences in baseline characteristics. There was 9% greater incidence of AMS in the day of ascent acetazolamide group (48.0% vs. 39%, 95% confidence interval [CI] −11.8 to 30, p = 0.46, number needed to treat [NNT] = 5.6 vs. 3.7), with the CI just surpassing the predetermined 26% noninferiority margin. There was a lower incidence of severe AMS (1993 LLQ >5) in the day of ascent group (n = 5, 10%, NNT = 2.3) compared with night before dosing (n = 12, 22%, NNT = 3.1) (95% CI −28 to 3.6), and lower average symptom severity in the day of ascent group (3 vs. 3.5, 95% CI −0.5 to 1.4).
Conclusions:
Day of ascent acetazolamide demonstrated higher rates of AMS compared with traditional dosing by a small margin. With similar rates of severe AMS and overall symptom severity, the potential for improved convenience and compliance may support day of ascent use.
Introduction
Acute mountain sickness (AMS) is a distressing and potentially debilitating disease common in the estimated 100 million who rapidly ascend from low altitudes to elevations above 2500 m (8250 ft) around the world (Burtscher et al., 2001). AMS rates of 40%–85% are commonly observed in hikers (Purkayastha et al., 1995; Lipman et al., 2012), 22%–37% in disaster first responders (Xu et al., 2013; Du et al., 2016), and seen in 13% of evacuated military casualties (Peoples et al., 2005a). Prevalence and severity of AMS are largely dependent on ascent rate (Purkayastha et al., 1995). While gradual ascent has proven effective as a preventive strategy (Purkayastha et al., 1995; Beidleman et al., 2009), this is often logistically infeasible in both recreational and tactical situations. The carbonic anhydrase inhibitor acetazolamide is considered the first-line AMS chemoprophylactic (Eigenberger et al., 2014; Robach et al., 2016) and is the only U.S. Food and Drug Administration-approved medication for AMS prevention, with recommendations to administer the day or night before rapid ascent (drugs.com, 2019; Netzer et al., 2013).
Acetazolamide's main action in acclimatization is through a renal bicarbonate diuresis. The resultant metabolic acidosis induces compensatory increased minute ventilation that attenuates the diminished arterial oxygen availability at high altitude (Swenson, 2014). Prior investigations of acetazolamide's effects have studied administration of low doses (125 mg twice daily) taken the day or night before ascent to high altitude (Kayser et al., 2012; Ritchie et al., 2012), although optimizing oxygenation has led some researchers to recommend preventive dosing 2 days before ascent (Burtscher et al., 2014). Acetazolamide has a time to onset of 60–90 minutes, with peak diuresis between 2 and 4 hours for the immediate release tablet (Leaf and Goldfarb, 2007). These pharmacokinetics were clinically surmised when day of ascent acetazolamide significantly prevented severe AMS compared with placebo (Lipman et al., 2018). Furthermore, analysis of two recent high altitude trials showed no statistically significant difference between day of and night before ascent acetazolamide in AMS incidence (p = 0.6) (Burns et al., 2018; Lipman et al., 2018). However, the efficacy of day of ascent acetazolamide for AMS prevention has yet to be confirmed. Given the importance of AMS prevention, a novel day of ascent acetazolamide regimen may increase utilization and optimize safety for ascent.
The objective of this trial was to evaluate if acetazolamide administered the day of ascent to high altitude was no worse than night before ascent dosing in prevention of AMS incidence.
Materials and Methods
Study design and setting
This study was a double-blind, randomized, controlled noninferiority trial approved by the Stanford University School of Medicine Institutional Review Board. Clinicaltrials.gov Identifier: NCT03424226.
Selection of participants
Study participants were recruited through a variety of e-mail list-servers with both local and national distributions. Inclusion and exclusion criteria were presented for participants to self-screen for eligibility before enrollment. Eligible participants had to be healthy, reside at low altitude (<1240 m [4100 ft]), and be able to complete a moderately strenuous hike at high altitude.
Exclusion criteria included: participants younger than 18 years or older than 75 years; pregnant or thought to be pregnant; lived or slept at altitudes greater than 1240 m (4100 ft) in the past week; ingested nonsteroidal anti-inflammatory drugs, acetazolamide, or steroids the week before the study; history of allergy to acetazolamide or sulfa drugs; or any hazardous medical conditions that preclude the ability to moderately hike to high altitude, including sickle cell anemia, severe asthma, severe anemia, or severe coronary artery disease.
The study was conducted over four weekends in August and September 2018 on White Mountain, California. Participants were enrolled at Bishop, California. All participants were provided information on AMS risks and symptom reduction strategies and were instructed to avoid carbonated beverages, alcohol, and recreational drugs.
Interventions
The night before ascent to high altitude, participants signed informed consent, completed demographic questionnaires, and were randomized to either acetazolamide 125 mg or visually identical placebo, using a 1:1 ratio and computer-generated random sequence (Marine Pharmaceuticals, San Mateo, CA). The randomization code was unavailable to administrators and participants. The first dose of acetazolamide 125 mg or visually identical placebo was given before midnight the night before ascent. The day of ascent, all participants took both acetazolamide and placebo at 9 am and 6 pm. The study began at 1240 m (4100 ft), and participants first drove to a staging area at 3545 m (11,700 ft) for a 1.6 km (1 mile) hike and lunch. Participants then hiked ∼4.3 km (2.7 miles) to 3810 m (12,570 ft), after which the last dose of acetazolamide was administered.
Measurements
AMS incidence was calculated by the 1993 Lake Louise Questionnaire (1993 LLQ), a well-validated, self-reported symptom-based questionnaire (Roach et al., 1993). The 1993 LLQ score was measured the night of ascent and again the morning after ascent. The values recorded the morning after ascent (or at time of rescue medication) were used for primary outcome analysis to ensure that the maximum amount of time was allotted for the symptoms to declare themselves, as symptom severity is typically highest the day after ascent. Also, the 1993 LLQ score of the evening of ascent would, by necessity, include the quality of sleep from the prior night at low altitude, which would be less accurate.
Participants were randomized in a first come, first served manner to a nocturnal wrist continuous pulse oximeter. During sleep, peripheral oxygenation (SpO2) was recorded continuously using a wrist-worn pulse oximeter (Nonin 3100; Nonin Medical, Inc., Plymouth, MN). The wrist oximeters were initialized according to the manufacturer's recommendation and software (nVision; Nonin Medical, Inc.). Before sleep, participants adhered a flex sensor to the index finger of their nondominant hand. The flex sensor placement activated the wrist oximeter's continuous recording, and the flex sensor was removed upon awakening to stop the recording. The wrist oximetry data were then downloaded and analyzed using the nVision software.
Groningen Sleep Quality Scale (GSQS) score, a sleep quality perception survey previously validated at high altitude (Jafarian et al., 2008), was recorded the morning after ascent. If the participants requested treatment for AMS, they provided endpoint data before treatment that included acetazolamide (250 mg tablet), ondansetron (8 mg oral dissolving tablet), dexamethasone (4 mg tablet), and/or supplemental oxygen (2 L/min). No additional data were gathered on participants treated for AMS to avoid confounding results.
Outcomes
The primary outcome measure was AMS incidence defined by the 1993 LLQ score of ≥3 with headache and a minimum of 1 for other symptom. Secondary outcome measures included: incidence of severe AMS (1993 LLQ >5), 2018 AMS (≥3 with headache and a minimum of 1 for other symptom, as the recently revised 2018 LLQ eliminated the sleep quality question) (Roach et al., 2018), severe 2018 AMS (2018 LLQ >5), average 1993 LLQ score, GSQS, and nocturnal SpO2.
Analysis
Sample size was based on prior high altitude trials at the study site using identical ascent profiles that found consistent AMS rates of 63%–69% in placebo (Lipman et al., 2012; Lipman et al., 2018) and 43%–51% AMS in those administered acetazolamide (Burns et al., 2018; Lipman et al., 2018). To achieve 80% power (α = 0.05, two-tailed test), assuming 45% AMS incidence with night before ascent acetazolamide, a total of 90 participants were required to detect a significant difference, defined a priori as a 26% absolute difference in AMS incidence between the dosing regimens. This difference was deemed clinically significant, as it equated to a number needed to treat (NNT) of 4 (Lipman et al., 2012). Primary and secondary outcomes were analyzed in both the intent-to-treat population and per-protocol group to include those who ingested excluded medications in the week before the study start (but was recognized postrandomization) to evaluate real-world hiking conditions. Additionally, the per-protocol group analysis enabled us to assess any effect of potential reduced AMS incidence from chemoprophylaxis.
All demographic variables were analyzed by Pearson's chi-squared tests, with the Welch two-sample t-test used for weight, height, and age. Primary and secondary outcome measures of AMS incidence and severity were analyzed using a two-sample test of equal proportions and tests for differences in group central tendency, respectively. The 1993 LLQ scores were analyzed by the Wilcoxon rank-sum test with p-values corrected for multiple comparisons by the Holm method. GSQS and SpO2 were evaluated for their ability to predict AMS by the 1993 LLQ score using a linear least squares regression. Comparisons between the 1993 LLQ version incidences were evaluated with a confusion matrix for accuracy, sensitivity, and specificity. Placebo rates of AMS from prior studies with identical ascent profiles were utilized for NNT analysis. p-Values <0.05 were considered significant and 95% confidence intervals (CIs) were used. All analyses were conducted using the R statistical computing software version 3.
Results
One hundred five participants signed informed consent, with one excluded post hoc for not taking the study medications. Fifty-four (52%) were randomized to night before ascent acetazolamide and 50 (48%) to the day of ascent group. Of the 104 participants included in the intent-to-treat analysis who were randomized and administered medications, 8 ingested excluded medications within the week before the trial, with 95 participants (91%) analyzed in the per-protocol population (Fig. 1). Baseline characteristics were similar between the two groups (Table 1). No participant required evacuation.

CONSORT participant diagram. ITT, intent-to-treat.
Demographic Variables
BMI, body mass index; SD, standard deviation.
Intent-to-treat analysis showed that the day of ascent acetazolamide group had 9% greater incidence of AMS than the night before ascent group, just surpassing the predetermined 26% noninferiority margin (48.0% vs. 39%, 95% CI −12 to 30) (Fig. 2). The day of ascent group had an NNT of 5.6 and the night before ascent group had an NNT of 3.7 to prevent one case of AMS. For severe AMS, the night before ascent group had an NNT of 2.3 and the day of ascent group had an NNT of 3.1. The two groups had similar incidences of the secondary outcomes of severe AMS, 2018 AMS, severe 2018 AMS, and average symptom severity by the 1993 LLQ (Table 2). These outcomes were similar in the per-protocol population (Supplementary Fig. S1). No differences in significance were observed between the two groups when comparing age, sex, ethnicity, and history of altitude illness. Subgroup analysis of the 1993 LLQ symptoms did not reveal any significant differences between the dosing groups in any individual complaint except for gastrointestinal, which had statistically significant greater rates in the night before ascent group (Table 3). As there were no differences in SpO2 variables between the study arms (Supplementary Table S1), cohorts were combined and analyzed by AMS diagnosis. Table 4 shows that those with AMS had significantly greater high altitude sleeping desaturations, desaturation index, and number of hypoxic events <88% SpO2.

ITT primary and secondary outcomes. AMS, acute mountain sickness.
Per Group and Total Outcomes for Intent-To-Treat Analysis
Difference in estimate of severity between the treatment groups.
AMS, acute mountain sickness; CI, confidence interval; LLQ, Lake Louise Questionnaire.
1993 Lake Louise Questionnaire Components
Oxygenation Variables by Acute Mountain Sickness
N = 30.
N = 42.
There were no observed differences in sleep quality by the 1993 LLQ and GSQS between study arms in the intent-to-treat and compliant groups (Supplementary Tables S2 and S3), so both cohorts were combined and analyzed in the intent-to-treat population. There was a significant linear correlation between the 1993 LLQ sleep score and GSQS (adjusted R2 = 0.56, 95% CI 0.43–0.68) (Fig. 3). There was also a significant correlation between the total 1993 LLQ score (as a proxy for AMS) and GSQS (adjusted R2 = 0.37, 95% CI 0.23–0.53) (Fig. 4).
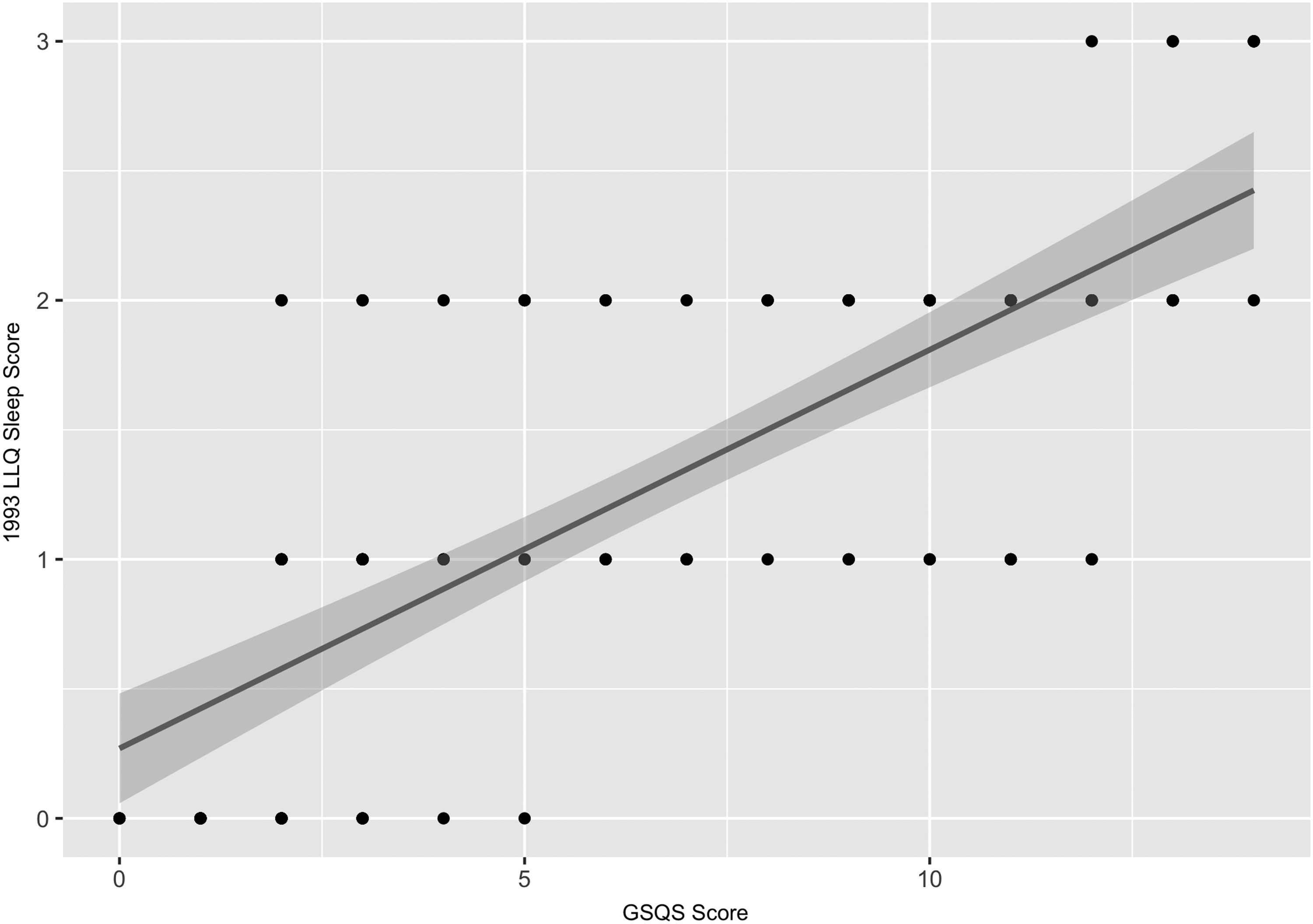
GSQS and 1993 LLQ sleep component. GSQS, Groningen Sleep Quality Scale; LLQ, Lake Louise Questionnaire.
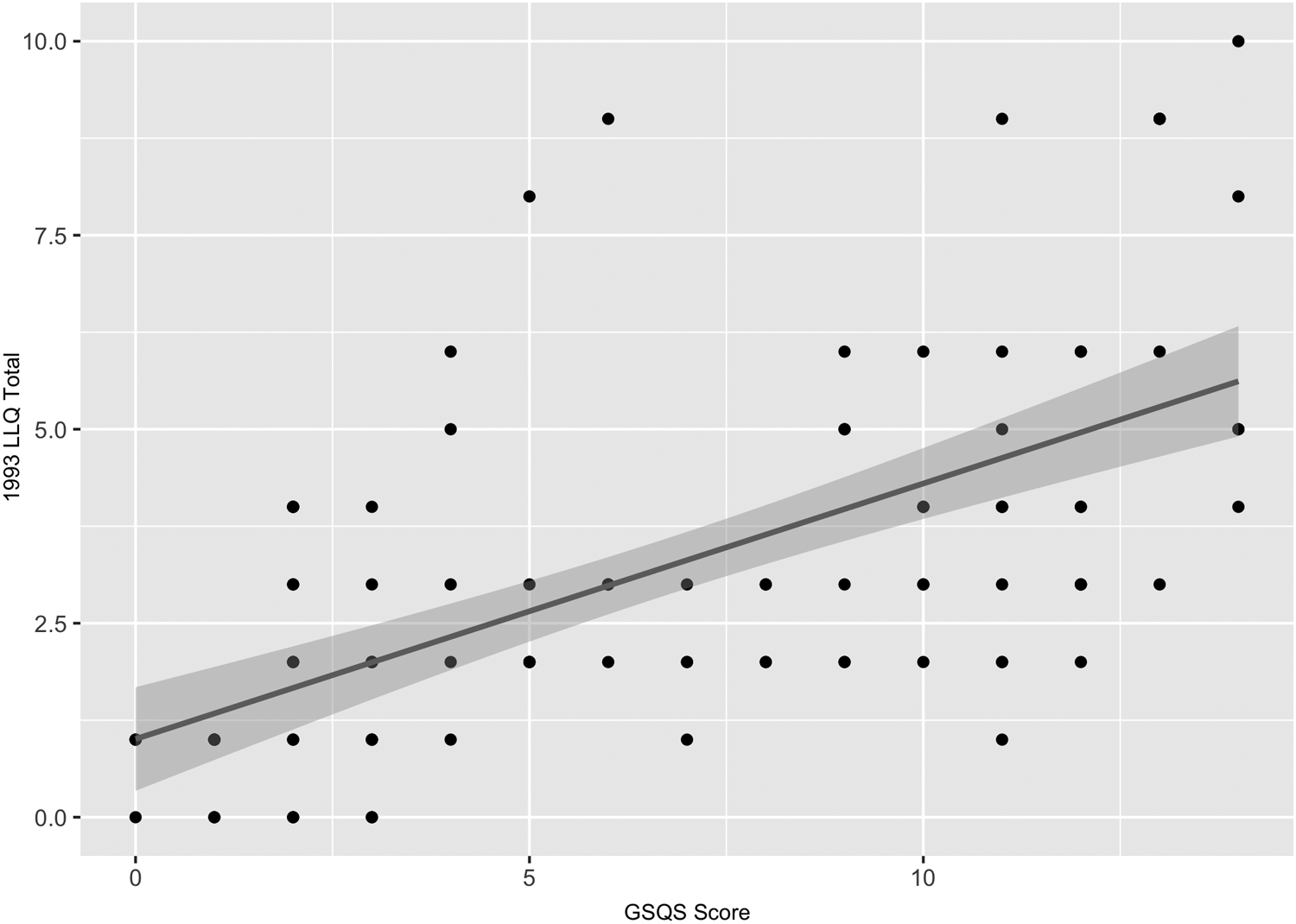
GSQS and total 1993 LLQ score.
Discussion
We found that the day of ascent acetazolamide had 9% greater incidence of AMS compared with the night before ascent acetazolamide. The upper 95% confidence limit exceeded our prespecified noninferiority margin when comparing the two groups by 4%. Therefore, the trial was unable to confirm that the day of ascent acetazolamide was no worse than the traditional acetazolamide dosing regimen for AMS prevention. It is unclear whether this small difference is clinically relevant, as day of ascent dosing showed a lower incidence of severe AMS, which has been shown to be more clinically relevant and accurate than the mere diagnosis of mild illness (Maggiorini et al., 1990). The overall symptom severity and individual AMS symptoms with the day of ascent acetazolamide were either similar to or significantly less than the night before ascent dosing. This may have been due to the greatest diuretic effect (and maximized compensatory ventilatory benefit) occurring in closer proximity to peak altitude obtained. An additional benefit of day of ascent dosing was significantly fewer participants with gastrointestinal symptoms. This could be attributed to the smaller total amount of ingested acetazolamide, as gastrointestinal distress is a well-known side effect of acetazolamide (Ellsworth et al., 1987). Considering that AMS incidence with the day of ascent acetazolamide was ∼20% lower compared with the historical 63%–69% AMS incidence in historical placebo groups at the study site (Lipman et al., 2012; Lipman et al., 2018), it is likely that day of ascent acetazolamide offers robust physiological and symptomatic protection. Although the observed rate of AMS was high even with acetazolamide, the observed NNT of 3.7–5.6 was equivocal to the reported NNT of 3–6 in the literature (Low et al., 2012).
A potential clinical benefit of day of ascent acetazolamide for AMS prevention is increased utilization among climbers, search and rescue, disaster response, and military personnel. These recreational and tactical missions often do not have the luxury of advanced notice before high altitude travel and deployment. Up to 20% of first responders and entire 300-member rescue teams at high altitude natural disasters have necessitated early evacuation due to AMS (Wu, 2011; Xu et al., 2013), with deaths from altitude illness in earthquake rescuers in China and Nepal (Wu, 2011; Du et al., 2016). Decreasing morbidity and mortality from altitude illnesses in these personnel could optimize resource allocation to target populations. Also, as altitude illness was found to be the largest contributor of illness and nonbattle casualties during early Afghanistan conflicts (Peoples et al., 2005b), pretreatment with acetazolamide the day of ascent would be more beneficial than nothing at all on rapid ascent to high altitude.
The hypobaric hypoxia of high altitude is accepted as the primary environmental insult leading to AMS (Roach et al., 1998; Kayser, 2009), but demonstrating this relationship has proved complex. Lower SpO2 is a common finding in those with AMS compared with healthy controls (Roach et al., 1998; Brierley et al., 2012), but there is enough overlap that SpO2 is acknowledged as an inaccurate test for diagnosis or prediction of disease (Roach et al., 1998; Faulhaber et al., 2014). AMS has been associated with nocturnal hypoxemic events (Burgess et al., 2004), and our findings support this pathophysiological role as multiple nocturnal oxygenation parameters were significantly decreased in those symptomatic with AMS.
Sleep disturbance is a common occurrence at altitude, with rates reported over 70% (Larson et al., 1982). While poor sleep at high altitude is almost universal, AMS is not. Since the initial inclusion of sleep as a symptom in the 1993 LLQ, researchers have debated its utility (Milledge, 2014). The 2018 LLQ recently dropped sleep from the diagnosis of AMS based on symptom discordance in network analysis studies (Macinnis et al., 2013; Hall et al., 2014). However, the strong positive correlation observed between the 1993 LLQ sleep scores, severity of AMS symptoms, and GSQS suggests that inclusion of high altitude (rather than low altitude) sleep quality is a parameter that may have useful diagnostic accuracy for AMS.
Several limitations should be considered. The incidence of AMS and severe AMS with placebo has been well established and consistently reproduced at the studied location with identical ascent rates (Lipman et al., 2012; Lipman et al., 2018). While this allowed both an accurate power analysis and historical benchmark for comparison and analysis of the NNT, the lack of a placebo arm in this trial introduces some uncertainty into the analysis. That being said, it has been argued that as acetazolamide's benefit over placebo has been so well established, a placebo arm in AMS prevention trials with acetazolamide may be unnecessary (Penninga et al., 2013). The trial's primary outcome of AMS incidence was based on the definition established in 1993 (Roach et al., 1993). After the trial's methodology had been established, the diagnostic criteria of AMS were changed (Roach et al., 2018). Because the study's power analysis was predicated on the previously observed AMS rates at the White Mountain study site, it was necessary to use the established 1993 LLQ. This was found to have a high sensitivity (97%), specificity (96%), and accuracy (96%) compared with the 2018 LLQ. The high degree of agreement according to these measures suggests the trial's outcome is generalizable to the most recent definition.
Participants spent their first night at 1240 m (4100 ft), making a mild degree of acclimatization possible. Caution should be exercised when results are extrapolated to higher altitudes than attained in our study, or when individuals ascend directly from at or near sea level. We were unable to control for environmental conditions, rate of ascent during participants' hike at altitude, liquid and caloric intake, and underlying physiological conditions. Participants were self-selected and their characteristics cannot necessarily be applied to those of other hiking populations. Direction for future studies on the optimal dosage of acetazolamide should take into account the study participants' body size to more fully to assess the varying pharmacokinetic effects.
Conclusion
Our study demonstrated that day of ascent acetazolamide resulted in slightly higher rates of AMS than traditional night before ascent dosing. However, the difference of AMS incidence between groups was a small margin. With similar rates of severe AMS and overall symptom severity, the potential for improved convenience and compliance may support day of ascent use.
Footnotes
Acknowledgments
This study was generously supported by the Wilderness Medical Society Herbert N. Hultgren grant by the Academy of Wilderness Medicine®, Institute for Altitude Medicine, and USARIEM material and personnel support. We deeply appreciate the logistical assistance of White Mountain Research Center personnel and facilities, and the enthusiasm and participation of our trial participants who made this research feasible.
Authors' Contributions
Study concept and design: G.S.L., C.J., and P.H. Acquisition, analysis, or interpretation of data: all authors. Drafting of the article: all authors. Critical revision of the article for important intellectual content: all authors. Statistical analysis: C.P. Funding: G.S.L. Study supervision: G.S.L. Dr. G.S.L. had full access to all the data in the study and takes responsibility for the integrity of the data. C.P. conducted the analyses and is responsible for the data analyses reported.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.