
Abstract
Aims:
Psychotic symptoms during exposure to high altitude (HA) have been linked to accidents or near accidents on the mountains. It is thus of great importance to directly identify psychotic symptoms in individuals who are exposed to HA quickly and reliably on the mountain, even in the absence of experienced medical personnel. Psychotic features at HA frequently include positive psychotic symptoms such as hallucinations, delusions, or disorganized thinking/speech. The aim of the current study was to develop the first self-administered questionnaire (High Altitude Psychosis [HAPSY] Questionnaire), which individuals may use in the future to self-assess altitude-related psychotic symptoms on the mountain.
Methods:
We utilized two existing self-rating questionnaires for psychotic symptoms (the Psychotomimetic States Inventory, PSI and the Cardiff Anomalous Perception Scale, CAPS) as the basis for a two-round Delphi process. As part of this process, additional statements were suggested by the 40 Delphi participants.
Results:
Eleven self-administered statements—all of them related to positive psychotic symptoms—were identified to be most useful for the self-detection of HA-related psychotic symptoms on the mountain.
Conclusion:
This is the first self-administered questionnaire that allows the identification of HA-related psychotic symptoms on the mountain. A subsequent validation study is needed to address the psychometric properties of this questionnaire. Clinical validation will have to be performed in a field study.
Introduction
Professional medical knowledge and high altitude (HA) climbers' awareness of somatic HA-related symptoms such as acute mountain sickness (AMS), HA cerebral edema (HACE), and HA pulmonary edema have increased over the past decades, but research on HA-related psychiatric symptoms is still scarce. We have recently identified isolated HA psychosis as a medical entity, which can occur at HA in the absence of HACE or delirium of other causes (Hufner et al., 2018). However, while organic-induced psychosis (e.g., in the context of HACE) are often associated with altered consciousness and prominent somatic symptoms such as headache and ataxia (Wu et al., 2006) or fever (Pendlebury et al., 2015), individuals with isolated HA psychosis show no or few associated medical symptoms and therefore often retrospectively report that they descended from the mountain without medical assistance (Hufner et al., 2018).
Symptoms of isolated HA psychosis were found to occur at a mean altitude of ∼7000 m and to be quickly reversible once lower altitudes are reached, which makes it likely that hypoxia plays a major role in the etiology of this disorder (Lempert et al., 1994). As with most altitude-related symptoms, the incidence of isolated HA psychosis is probably decreased at lower altitudes. In our previous work, 3800 m was the lowest altitude at which it was reported (Hufner et al., 2018). Exhaustion, sleep deprivation (Meyhofer et al., 2017), psychological stress, and social deprivation might also be contributing factors (Daniel and Mason, 2015). Other psychiatric disturbances which can occur during acute HA exposure are neuropsychological deficits, such as reduced concentration, memory and psychomotor performance, alterations in mood (mostly depressed mood), and irritability (Shukitt-Hale et al., 1991; Bolmont et al., 2000; Virues-Ortega et al., 2004; de Aquino Lemos et al., 2012).
The nature of psychosis at HA is not yet fully characterized. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association, 2013) defines psychotic symptoms as hallucinations, delusions, disorganized speech, abnormal psychomotor behavior, and negative symptoms, as well as impaired cognition, depression, and mania (American Psychiatric Association, 2013; Barch et al., 2013). Notably, psychotic symptoms are transdiagnostic (Fusar-Poli et al., 2017c) and can occur not only in schizophrenia but also in mood disorders, substance abuse disorders, due to other medical conditions or as part of the syndrome of organic brain dysfunction (classified as delirium in DSM-5). The predominant modality of hallucinations may vary depending on the underlying condition (e.g., they are often visual in nature in delirium, acoustic in schizophrenia (Chaudhury, 2010) while “the third man phenomenon” has been found frequently in isolated HA psychosis (Hufner et al., 2018)), but it is inadvisable to give weight to the presence of any featural properties of hallucination alone when making a diagnosis (Waters and Fernyhough, 2017). Psychotic symptoms can also be brief and self-remitting and are thus not invariably associated with persistent psychotic disorders (Fusar-Poli et al., 2016a, 2017a).
Yet, these psychotic features can have detrimental impact on the persons who experience them. This has recently been reported by the media in the case of rescued French climber Elisabeth Revol who reportedly removed her boot and suffered severe frostbite on a winter ascent to Nanga Parbat. She recollected, while being alone in her tent, feeling the hallucinatory presence of a friendly woman who offered her hot tea and requested that she took off her boot in return (BBC News, 2018). Similarly coauthor I.T. reported that during his climb as the medical doctor of an expedition on Dhaulagiri, auditory hallucinations in the form of guides suggested he should jump off the East face (an over 2000 m high, very steep wall) to shorten the descent (Hufner et al., 2018). These two prototypical examples highlight how psychotic symptoms in such extreme scenarios can expose individuals to high risks. Psychotic symptoms at HA are associated with increased accidents or near accidents (Hufner et al., 2018). Some climbers retrospectively assign a positive or helpful connotation to their psychotic experiences: For example, climber Stephen Venables described psychotic symptoms during his expedition to Mt. Everest, which in fact helped him survive when he was forced to spend the night above 8000 m unprotected. He reportedly felt the hallucinatory presence of an old man next to him, advising him on how to stay alive, and later he felt the hallucinatory presence of various other people warming his extremities (Venables, 2013).
It is thus of great importance to detect psychotic symptoms as soon as they emerge in individuals at HA, directly on the mountain, even in the absence of experienced medical personnel. Given the extreme environment, such an assessment tool for psychotic symptoms needs to be simple and easy to administer, as is the case for example, AMS scoring (Roach et al., 2018). It should be designed to rapidly detect emerging psychotic symptoms so that appropriate preventive or treatment measures can be implemented accordingly.
The aim of the current study was to develop the first self-rated questionnaire that can be used on the mountains, without the need for administration by specialized medical personnel, to identify symptoms of psychosis at HA.
Materials and Methods
This study was approved by the local Ethics Committee of Innsbruck Medical University.
The Delphi method
The Delphi Method (Dalkey and Helmer, 1963; Brown, 1968) is an established research tool which aims to obtain a reliable, unbiased consensus within a group of experts (see also Brodmann Maeder et al., 2018). The Delphi participants anonymously join a multiple round survey process with controlled opinion feedback. Direct confrontation between the experts is avoided to reduce bias, and their feedback/comments are made available to the other experts included in the process. An administrative group, entitled “core group” in the present study, is responsible for preparing the questionnaires, evaluating, and summarizing the results, as well as providing anonymous feedback to the Delphi participants until consensus is achieved.
Selection of Delphi experts
We included the following experts with specific expertise related to the topic of interest: (1) a group consisting of HA climbers, who themselves had experienced at least one symptom of psychosis and (2) a group of psychiatrists specialized on research and/or clinical management of psychosis.
Climber selection
We included only climbers who themselves had experienced at least one psychotic symptom while at HA. The climbers were recruited from a database previously established (Hufner et al., 2018) and through personal contact. Contact information of the climbers was obtained from the internet, social media, or third parties. Climbers whose psychotic episode at HA had not been previously validated for the database were questioned by one of the study authors before inclusion in the study to ascertain the nature of their symptoms. DSM-5 dimensional criteria (as reflected in the Clinician-Rated Dimensions of Psychosis Symptom Severity Scale, CRDPSS) were used for assessment of psychosis, at least two criteria had to be present, with one of them being delusions, hallucinations, or disorganized speech (primary symptoms of psychosis) (American Psychiatric Association, 2013; Barch et al., 2013).
Psychosis expert selection
Psychiatrists with research expertise in psychotic disorders (identified as psychosis research experts) were identified using the online scientific citation indexing service “Web of Science.” In a first step, we identified the highest ranked journals in the field of psychiatry and psychotic disorders, namely World Psychiatry, JAMA Psychiatry, Lancet Psychiatry, Schizophrenia Bulletin, and Schizophrenia Research. In a second step, the authors who were most successful in publishing in these high-ranked Journals on the topic of psychosis in the past 5 years (2014–2018) were selected. We included the first 20 hits (i.e., those individuals who had published the highest number of articles on “psychosis”) per journal. Contact information was then retrieved using internet search engines and social media. Psychiatrists with expertise in the clinical management of psychotic disorders (identified as psychosis clinical experts) were recruited in the alpine region of Austria, Germany, and Italy from large university or regional hospitals. Contact information was retrieved using the internet or requested personally. The ratings from psychosis research experts and psychosis clinical experts showed similar distributions (Mann–Whitney U test, p > 0.05), therefore their answers were analyzed as a single group.
Inclusion/exclusion criteria
Participants of the Delphi process had to be older than 18 years and were required to give informed consent. Since the questionnaire was available in English exclusively, only participants with fluent knowledge of English were allowed to participate.
Design of Delphi process
Round 1
The selected participants were contacted through e-mail/social media and provided with information about the study, the informed consent sheet and the Round 1 questionnaire in form of a “write in” pdf. The participants (subsequently referred to as the “Delphi experts”) were required to individually rate 80 symptom-related statements, which were postulated to be potential indicators of psychosis at HA. These statements had been taken from preexisting questionnaires (previously developed for a use other than psychosis at HA), namely the Psychotomimetic States Inventory (PSI) (Mason et al., 2008) and Cardiff Anomalous Perception Scale (CAPS) (Bell et al., 2006). The CAPS is a validated self-report psychometric method designed to measure perceptual anomalies. Patients with diagnosed psychotic disorders obtain an overall higher CAPS score than the average healthy population (Bell et al., 2006). The PSI is a questionnaire designed to measure psychotomimetic states, for example, in the context of cannabis and ketamine use or in social deprivation (Mason et al., 2008).
All 80 statements were presented in the order of the original questionnaires, starting with the CAPS questions. In an accompanying document, Delphi experts were informed about the purpose of the Delphi process being the development of a brief self-rating questionnaire to detect psychosis at HA, directly on the mountain. Each Delphi expert was asked to indicate which of the proposed statements they found either “very helpful”—“helpful”—“moderately helpful”—“slightly helpful”—“not helpful at all” to evaluate psychosis at HA. The climbers were asked to rate the statements based on their personal experience while mountaineering. The psychosis experts were instructed to answer the statements based on their research or clinical expertise. Specific open text sections were provided where Delphi experts were encouraged to suggest additional symptoms they deemed important, to explain why they performed a certain rating of a statement, and provide suggestions on how to improve the outcome of the study. In addition, climbers had the opportunity to describe their own HA psychotic experiences.
Personal information, including gender and age, was requested from all participants together with information pertaining to previous levels of altitude exposure and current altitude of residence. Psychosis experts were also asked to describe the amount of time spent during their careers on research and/or clinical work regarding psychosis. All participants were offered the opportunity to be acknowledged for their assistance in this study. Delphi experts were allowed 4 weeks to complete and return the questionnaires. Two weeks after the invitation e-mail, a reminder e-mail was sent out.
Round 2
The set of statements resulting from Round 1 was sent out to the same Delphi experts who had participated in Round 1. The statements had to be rated exactly in the same way as Round 1. Questions were presented in a random order, so that each statement could be evaluated individually, without the influence of a previous similar statement. Once again, the Delphi experts had the opportunity to add additional comments. Delphi experts were given 4 weeks to complete Round 2. Two weeks after the invitation e-mail to Round 2, a reminder e-mail was sent out.
Evaluation
Evaluation of open text sections
The freely inputted text generated from the Delphi experts was collected and presented to the study core group. The inputs were divided into statements for inclusion into the questionnaire and overall comments for improvement of the study. All members of the core group were asked to comment on the statements nonanonymously. The comments were then summarized by the two study coordinators (K.H. and F.C.). This summary was discussed with the core group members digitally, by telephone/Skype conference and/or face to face conferences (depending on the availability of the core group members), until a consensus was reached on all points.
Statistical analysis
The Delphi experts represent two specific groups with different backgrounds regarding HA as well as psychosis experience, so statistical evaluation was conducted separately for the two groups. As the obtained data for each round showed different characteristics, the assessment procedures were adopted ad hoc considering the data distributions. Statistical analysis of the results was based on exploring and measuring data distributions by the use of descriptive statistics such as quartiles and mode. The differences between the distributions were tested by the use of nonparametric Mann–Whitney U test.
All Delphi experts' responses to the proposed statements were transferred to an EXCEL® spreadsheet. The response options “very helpful”—“helpful”—“moderately helpful”—“slightly helpful” and “not helpful at all” were then coded numerically from 4 to 0 points, respectively.
Data were analyzed using statistical software IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp, 2016) and “R” software (R Core Team, 2018).
Results
Round 1: results of Delphi experts' ratings
Forty-four percent (14/32) of all the climbers who were initially identified as having experienced psychosis at HA, and for whom contact information was available, plus 26% (26/102) of all psychosis experts, for whom contact information was available, participated in the study (Supplementary Fig. S1). Demographic information on Delphi experts and data on their HA exposures are given in Table 1.
Demographic Information of Delphi Study's Participants
All of the climbers (14 participants) and 24 out of the 26 psychosis experts completed the demographic section of the questionnaire.
p-values were calculated using Mann–Whitney U test and Chi Square test, respectively.
Absolute numbers (%).
NA, not applicable; SD, standard deviation.
To identify the statements that rated most relevant for the detection of psychosis at HA, principal statistical indices were calculated separately for each statement. Descriptive statistics of the data from the climbers' group differed from the psychosis experts' group (Mann–Whitney U test, p < 0.05). Thus, a differential statistical approach considering the structure of the data was applied for the both groups to identify the most relevant statements. In the case of psychosis experts' data, the index Q1 (first quartile: 75% of the values in the data positioned above Q1) resulted in the most appropriate threshold value. Selection of statements for which Q1 was at least 3 in the Likert scale codification (“helpful” or “very helpful”) ensured that at least 75% of experts judged a selected statement as “helpful” or “very helpful.” We identified 11 statements from the original questionnaire for inclusion in Round 2 (Table 2).
Round 1: Statements with the Highest Ratings in the Psychosis Experts Group
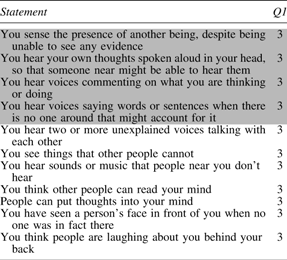
Statements that were selected by both Delphi groups (psychosis experts and climbers) in Round 1 were identified as “consensus statements” (in grey). These statements were not subject to evaluation in the second Round, although Delphi participants were given the opportunity to comment on them. The order of statements corresponds to the order of the original questionnaire.
In the case of climbers group, generally statements obtained lower ratings than were given by the psychosis experts. None of the statements reached a threshold value identified for experts' group; therefore a different approach was used to identify the most relevant statements in this group. To yield a number of statements comparable with the psychosis experts group, we selected the statements for which the most frequent values (modal values) were at least 2 (“moderately helpful”) (Table 3).
Round 1: Statements with the Highest Ratings in the Climbers Group
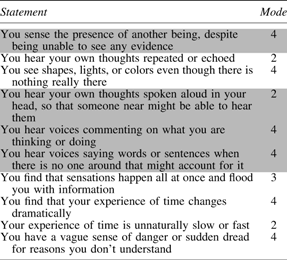
Statements that were selected by both Delphi groups (psychosis experts and climbers) in Round 1 were identified as “consensus statements” (in gray). These statements were not subject to evaluation in the second Round, although Delphi participants were given the opportunity to comment on them. The order of statements corresponds to the order of the original questionnaire.
Round 1: results of open text fields
The open text fields from Round 1 were evaluated by the core group, and seven new statements were identified, which were found to cover important symptoms not present in the Round 1 questionnaire (Table 4).
Eight Additional Statements Suggested by the Delphi Experts in Round 1 Which Were Included for Round 2
Many comments given in the open text fields by the Delphi experts pointed toward interesting topics (e.g., how frequent are the symptoms, do they disappear after using dexamethasone, do symptoms occur in a state of dehydration) and were deemed to be interesting questions for future research by the core group but not suitable for a questionnaire to diagnose psychosis at HA on the mountain. General comments by the Delphi experts pertaining to how the study may be improved were taken into consideration (e.g., keep the questionnaire short, evaluate the questionnaire also outside of a HA setting for comparison, compare the questionnaire with a prodromal screening tool, and analyze the statements on a continuous scale).
Round 1: core group evaluation and analysis
The core group classified all statements resulting from the Delphi process Round 1 according to the PSI Symptom Classification (Delusional Thinking, Perceptual Distortion, Cognitive Disorganization, Anhedonia, Mania, and Paranoia) (Mason et al., 2008) to make sure that a large spectrum of symptoms was also available for ratings in the next round. Since the category “anhedonia” was empty, the statement with the most favorable ratings (using the mode) was added for evaluation in Round 2.
Round 2: results of psychosis experts and climber ratings
All Delphi experts who participated in the Round 1 were again invited to join Round 2. A response rate of 82.5% was attained overall resulting from a 79% contribution from the climbers group and 85% from the psychosis experts group. A total of 11 climbers and 22 psychosis experts took part in Round 2 of this Delphi procedure. The goal of this round was to reduce the number of statements to a number considered acceptable to utilize the questionnaire on the mountain (10–15 statements was the predefined goal).
Similarly to the steps applied in Round 1, descriptive statistics were calculated for both groups' response data and the differences between two groups were found to be statistically different (Mann–Whitney test, p-value <0.01). Psychosis experts and climbers data were thus again analyzed separately. In this phase, considering the characteristics of the data distributions, the choice of consensus statements was based on the mode. Statements with the modal value at of least 3 (“helpful” or “very helpful”) were selected in both groups, and four statements reached this threshold in both groups and were included in the next version of the questionnaire (Round 2 consensus statements, Table 5).
Statements That Were Selected by Both Delphi Groups in Round 2 Were Identified as “Consensus Statements”
Finally, the core group aimed to identify those statements, which, over all Delphi participants and statistical parameters were those with the highest ratings. As a result, the remaining 18 statements from Round 2 were analyzed as 1 final set. To be included in the final questionnaire, a statement had to reach the following conditions together: a mode of 3 or 4 (the most frequent values in the statement are “helpful” or “very helpful”) and a median of 3 or 4 (50% of participants find the statement at least “helpful”) and a Q1 of at least 1 (75% of participants find the statement at least “slightly helpful”). Six additional statements were identified (Table 6).
Additional Statements Derived from Delphi Round 2 Which Received the Highest Ratings Overall in Both Delphi Expert Groups
Round 2: evaluation of free text
The consensus statements of Round 1 were presented to the Delphi experts without possibility to rate them. It was pointed out that in case of disagreement, an open text field at the end of the questionnaire could be used to express their opinion. No further comments were received concerning the consensus statements of Round 1. Additional comments from the Delphi experts in Round 2 included the suggestion, to compare the final rating system to a prodromal screening tool or to remove the statement on pseudohallucinations.
Finalization of the HAPSY questionnaire by the core group
In a final core group meeting, the following steps were performed.
Statements relating to the same modality of perceptional distortion were analyzed, leaving only the statement with the most comprehensive wording in the questionnaire. We acknowledge that this might lead to a loss of accuracy, but was done to keep within the frame of brevity and to avoid overemphasis of a certain symptom of psychosis at HA through simple repetition. This led to the removal of the statements “You hear voices commenting on what you are thinking or doing” and “You hear two or more unexplained voices talking to each other” as they were included in the statement “You hear voices saying words or sentences when there is no one around that might account for it.”
The statement “You are able to distinguish your hallucinations from reality while experiencing them” relating to pseudohallucinations was removed because they are not a hallmark of psychosis, and the core group members believed that only after the episode of psychosis, the climbers were able to distinguish their hallucinations from reality (also argued by one of the psychosis experts and one of the climbers).
During our previous work (Hufner et al., 2018), we ascertained that the third man phenomenon is a frequently reported perceptual abnormality at HA. However, only the sensing of another being (i.e., the statement “You sense the presence of another being, despite being unable to see any evidence”) or a conversation with another being (i.e., the statement “You have a conversation with a person who is not really there”) was covered by the questionnaire, but not so visual hallucinations of another person. Therefore, a decision was taken by core group consensus to revise the statement “You see a person's face in front of you, even if no one is in fact there.” This statement was changed to “You see a person or a person's face in front of you even if no one is in fact there.”
A randomization of the single items was performed by permutation of all statements.
The final HAPSY questionnaire after the Delphi procedure can be seen in Table 7. When applied to healthy individuals, this questionnaire can be completed in an average time of 1 minute.
Final HAPSY Questionnaire
Discussion
In the present study, we developed a short, new self-rating questionnaire—the HAPSY questionnaire—to measure psychotic symptoms at HA directly on the mountain. To the best of our knowledge, this is the first questionnaire to measure symptoms of psychosis at HA. We used a Delphi methodology with highly qualified experts to generate this questionnaire.
The ideal group of experts for this Delphi process would have been psychiatrists with expertise in HA medicine and specifically psychosis at HA. However, such a group was not available when we set out to perform the study mostly due to the fact that psychosis at HA has only been recently characterized in more detail in the medical literature. We included two groups of experts in this Delphi process: a group consisting of HA climbers, who themselves had experienced at least one symptom of psychosis; and a second group consisting of psychiatrists specialized in the research and/or clinical management of psychosis. We observed differences in data distribution between the two groups during statistical analysis: while climbers were instructed to evaluate only symptoms they had already experienced, psychosis experts were asked to base their evaluation on their previous experience of all patients with psychosis they had evaluated in their career. This led to fewer “positive” ratings in the climbers group. These distributions were taken into account during the statistical analysis.
For the development of the HAPSY questionnaire, we used statements from preexisting questionnaires (previously developed for a use other than psychosis at HA), namely the PSI (Mason et al., 2008) and CAPS (Bell et al., 2006). These two questionnaires were chosen on the basis of them being self-rating questionnaires for psychotic symptoms, covering domains found suitable also in psychosis at HA and free availability under an open license agreement (allowing for future distribution of the questionnaire). Additional statements suggested by the Delphi experts were also included.
The newly developed questionnaire may be particularly useful, in light of the paucity of self-rating questionnaires in psychosis research (Mass et al., 2005; Bell et al., 2006; Mason et al., 2008). This is due to the phenomenological nature of an acute episode of psychosis, which is intrinsically gestaltic, that is, it can only be appraised in the context of a contextual environment, which makes it especially helpful to have a screening questionnaire specifically for the use on the mountain (Fusar-Poli et al., 2017b). In fact, self-ratings at the time of the first onset of psychosis are difficult to perform, particularly with reference to delusions and hallucinations. Problems with concentration and comprehension of complex statements can also occur. In addition, there is a high difficulty of phrasing statements to detect hallucinations, delusions, and other psychotic symptoms, which we partly avoided by making use of the two established self-rating questionnaires for psychosis, which have both been successfully used both in healthy and psychotic individuals (Bell et al., 2006; Mason et al., 2008). These two questionnaires also have the advantage of relating to the current situation and not making reference to psychotic symptoms experienced in the past (Konings et al., 2006). Furthermore, they have been evaluated and validated for use also in mentally healthy general populations, in which psychotic symptoms can be observed, even in the absence of an established mental disorder (Mason and Brady, 2009).
The present HAPSY questionnaire consists only of statements concerning perceptual abnormalities. This may be due to the fact that positive symptoms of psychosis are more prominently remembered and therefore weighted stronger by the experts. This potential bias could actually prove advantageous for a self-rating questionnaire since the most easily detectable symptoms are measured. Problems with cognition are much more difficult to assess, especially when they are subtle.
Psychotic symptoms at HA can on the one side be a symptom of an organic disease such as HACE, infection, or dehydration (classified as delirium) or occur in isolation (so called isolated HA psychosis) without further psychiatric or somatic pathology (Hufner et al., 2018). The current HAPSY questionnaire can be used to detect symptoms of psychosis, but nothing can be inferred regarding the origin of these symptoms. Therefore, when psychotic symptoms are detected, further measures need to be taken to determine which diagnostic category they fall into and to allow for appropriate treatment. Altered levels of consciousness (operationalized as “reduced level of attention and awareness” in DSM-5) can help distinguish delirium from isolated HA psychosis (European Delirium Association and American Delirium Society, 2014).
However, In the acute setting on the mountain, the priority is to detect such symptoms early so that important decisions, for example, regarding route planning and whether or not to continue with the climb, will be undertaken by a person with symptoms of psychosis. Screening of psychotic symptoms should thus be performed on a regular, at least daily, basis alongside with screening for other HA disorders such as AMS. In addition, such individuals cannot be left alone but need to be accompanied during descent. For individuals climbing alone, psychotic symptoms could be detected using such a self-rating questionnaire, and cognitive techniques such as “reality testing,” which can be practiced beforehand, can then by applied once psychotic symptoms have been detected (Smailes et al., 2015).
Our study has several limitations. Since the questionnaire was developed using a Delphi process, its inherent deficits are present, such as the fact that this is not a controlled study but an expert opinion (Dalkey and Helmer, 1963). The most important limitation is that the questionnaire is not yet validated and will need to be validated against established ratings for psychotic symptoms before its use can be recommended. Possible established rating instruments which could be used include the Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987), the Brief Psychiatric Rating Scale (BPRS) (Overall and Gorham, 1962) or the Mini-International Neuropsychiatric Interview (M.I.N.I.) (Sheehan et al., 1998). In addition, comparison with and an established psychometric rating for attenuated psychotic symptoms (Loewy et al., 2011; Fusar-Poli et al., 2016b, 2017d) would be ideal.
Conclusion and further perspectives
Using a Delphi process, we developed a self-administered questionnaire which allows detection of HA-related psychotic symptoms on the mountain. It is planned to use the HAPSY questionnaire in a field study at Everest Base Camp (EBC) and validate it using an established physician's rating and a self-rating questionnaire for prodromal symptoms, as suggested by one of the Delphi experts, for example, the “Prodromal Questionnaire-16 item (PQ-16)” (Loewy et al., 2011). This questionnaire is usually used as a self-report screening measure for attenuated psychotic symptoms; therefore it could be ideal to test an emerging psychosis. Interestingly, the symptoms listed in the PQ-16 are quite similar to the HAPSY-Questionnaire. Cutoff values will need to be developed. Further research is needed to clinically characterize psychotic symptoms at HA, their pathophysiology, and treatment. It will be important to compare these features of psychotic symptoms at HA to psychotic symptoms occurring at sea level. The HAPSY Questionnaire might prove helpful in accomplishing this.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.