
Abstract
Introduction:
Cardiopulmonary resuscitation (CPR) quality may be impacted by location and setting of an out of hospital cardiac arrest. This study compared the quality of CPR performed on a moving ski patrol toboggan versus stationary CPR, both performed outdoors in winter.
Materials and Methods:
Compression-only CPR was performed on a manikin attached to a backboard secured into a toboggan. A CPR device was used to measure compression rate, depth and recoil, and elapsed time. A convenience sample of 30 patrollers, in weather-appropriate clothing, participated in this nonrandomized, crossover study. Each first performed 5 continuous sets of 30 compressions of stationary CPR straddling the manikin while kneeling. After 15 minutes rest, participants performed CPR while moving down the designated ski run (fixed length, vertical drop, and slope angles). Each ski run was video captured with a GoPro camera. Quality was defined as compliance with 2015 International Liaison Committee on Resuscitation (ILCOR) guidelines for CPR.
Results:
Overall, stationary and moving chest compressions complied with ILCOR guidelines, but there was a statistically significant degradation of CPR quality while moving and over time. Fewer compressions met ILCOR guidelines in comparison to stationary CPR compressions: (1) stationary mean depth 87% compliant, moving mean depth 35% compliant, 95% confidence interval: 39–65 (p < 0.001); (2) stationary mean rate 90% while moving mean rate 64% compliant; and (3) stationary recoil 74%, while moving recoil 77% compliant. Noncompliant compressions were typically too shallow, and noncompliance for rate was typically too fast. There were no pauses over 10 seconds once compressions were started.
Conclusions:
Despite CPR quality being reduced while moving, there were sufficient compliant compressions to support the use of CPR in this setting. Maintaining regular CPR training in a working environment and optimal body position in relation to the patient may be keys to performing high quality CPR on a moving toboggan.
Introduction
Cardiac arrests at ski areas are relatively rare events (Viglino et al., 2017). Cardiac arrest may be the result of a primary cardiac event, significant trauma (primarily blunt force), or postburial due to avalanche or falling into a tree well. At some point during resuscitation, transportation of the patient will be required as advanced care is rarely available at the scene. The most commonly used transportation modality is a commercially available ski patrol toboggan.
Cardiopulmonary resuscitation (CPR) training is a requirement for ski patrollers. The training usually occurs in an indoor setting, wearing indoor clothing. The training manikin and the student are stationary. There is little correlation with the conditions found in the ski patroller's working environment. A review of the pertinent literature found only one article assessing quality of CPR performed in the ski patrol setting. Thomassen et al. (2017) found nonsignificant differences in compression rates, depth, and leaning (recoil) in moving versus stationary conditions, although greater variance in these measures in the moving situation.
The aim of this study was to evaluate the quality of compression-only manual CPR (Sayre et al., 2008) when performed by ski patrollers in a moving ski patrol toboggan compared to their performance in a stationary on-hill toboggan.
Methods
A convenience sample of 30 ski patrollers was recruited from the staff of the Nakiska Ski Resort. Both females and males participated. All participants had requalified for CPR to the 2015 International Liaison Committee on Resuscitation (ILCOR) standard within the preceding year.
Quality was defined as compliance with the 2015 Guidelines for cardiopulmonary resuscitation as published by the ILCOR. The guidelines define high quality CPR as “compressions to a depth of not less than 5 cm but no more than 6 cm, at a rate of 100–120 compressions per minute, without pauses longer than 10 seconds. Chest recoil between compressions should be 100% (Nolan et al., 2015; Heart and Stroke Foundation—Canada Edition, 2017).
A Laerdal Mini-Anne 2010 CPR manikin was bolted to a wood backboard. “Legs” were fabricated and added to the manikin, secured by hook and eye fasteners on each side. Shoulders in the form of foam head immobilizer bolsters were added and secured by tape. The manikin was positioned in the toboggan with the head toward the rear of the toboggan. The backboard was secured by toboggan cross straps and paracord to prevent fore/aft movement.
A Physio-Control TrueCPR device was used to measure compression depth, chest recoil, compression rate, elapsed time, time with compressions, percentage time with compressions, and duration of no compressions (Physio-Control TrueCPR Coaching Device Owners Manual, 2012). The device included a visual indicator of compression depth and a metronome set at a rate of 104/min. The data were stored electronically. The posterior plate of the TrueCPR was placed under the left shoulder of the manikin and secured there with a velcro strap. The anterior puck was positioned over the sternum, but not secured.
All participants were advised of the research protocol that participation was voluntary and could be discontinued at any time. A review of this research project using the ARECCI tools (Alberta Innovates, 2010) determined it to be quality assurance research with low risks and not requiring formal ethical approval.
The research design was a crossover study with participants acting as their own controls. The protocol was:
Perform 5 sets of 30 compressions (compression-only CPR with no pause for ventilations) in a stationary toboggan, straddling the manikin in a kneeling position. Minimum 15-minute rest period. Perform compression-only CPR (no pause for ventilations) in a moving toboggan, straddling the manikin in a kneeling position, until reaching the bottom of the ski run.
The research was conducted outdoors from January to April 2017 and one day in April 2018. At the start of the day, the manikin was cooled in ambient temperature, before testing. During data collection the temperatures ranged from −16°C to +6°C. There was no noticeable wind on any testing day. Both phases of the protocol for each participant were conducted on the same day and completed within 60 minutes. The participants wore their regular weather-appropriate clothing, including ski gloves or mitts, helmets, and ski or snowboard boots. The only pieces of gear they removed before participating were backpacks. The patroller was not secured in the toboggan, although the manikin was secured.
The same ski run was used for the moving portion of this study. It was classed as an intermediate level run. It had a vertical drop of 440 m and was 1500 m long, with three short pitch changes of 27°, 23°, and 21°. The average slope angle was 12°. Participants drove the toboggan for each other. An unmodified Ferno-Traverse Rescue Squadra ski patrol toboggan from the Nakiska Ski Patrol fleet was used for the testing. The drivers were instructed to drive to deliver a smooth controlled ride. Velocity was not directly measured, but elapsed time was measured. All runs were video captured using a GoPro III camera on a handheld “selfie stick” carried by one of the researchers. The visual/auditory aids built into the TrueCPR were operating during the stationary and moving components of the trial. Each participant received immediate verbal feedback of their performance following both stationary and moving CPR from the TrueCPR. This included percentage of compliant compression depth, percentage of adequate chest recoil, compression rate, elapsed time, and percentage of elapsed time with compressions. We did not analyze each cycle of compressions individually, as we collected data for all compressions in each phase of the study. We did not analyze data in relationship to the outdoor temperature on any testing day.
After each trial day, the data from the TrueCPR were uploaded to an Apple Macintosh laptop running PhysioControl CodeStat software in a Windows operating system using Parallels to a Microsoft Excel spreadsheet. Descriptive statistics was calculated for compression depth, compression rate, and elapsed time using StatPlus Mac version 6. Two-tailed t tests were calculated for compression depth and rate. Significance was established at p < 0.05.
Results
The 30 ski patrollers ranged in age from 18 to 63 years old; mean age was 30 years. Each performed 5 sets of 30 CPR compressions while stationary in the toboggan. The median elapsed time was 149 seconds (2.48 minutes). During the moving phase of the study, the duration of CPR was dependent upon how quickly the toboggan descended the 1500 m of ski run length. The median duration was 202 seconds (3.4 minutes) (Fig. 1). In the following figures, the listing of subject is consistent. That is, Subject 1 is the same person in each figure, as is the case for all other subjects. There were three runs when the duration of moving CPR was less than stationary CPR. In the other 27 runs, the duration of moving CPR was substantially longer.
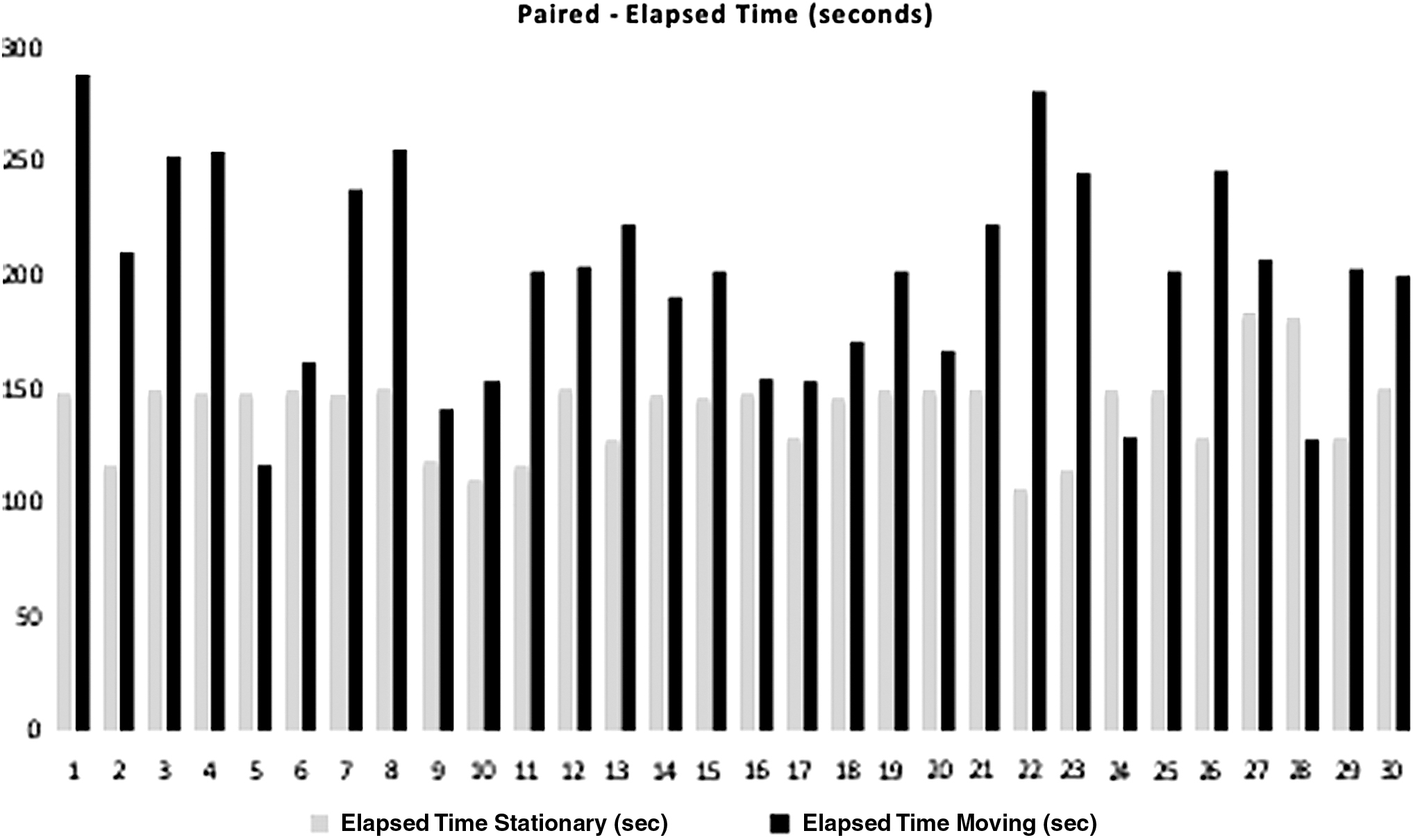
Paired times of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario. CPR, cardiopulmonary resuscitation.
There were significant differences in compression depth and rate in the stationary versus moving CPR results. Table 1 provides an overview of the descriptive statistics for compression depth in centimeters, compression rate per minute, and elapsed time in seconds. The mean depth of compression while stationary was 5.64 cm. In comparison, the mean depth of compressions while moving was 5.02 cm. These differences were statistically significant. The mean compression rates were similar and within the ILCOR standard for compression rate, although the difference between stationary and moving rates was statistically different.
Descriptive Statistics for Compression Depth, Rate, and Elapsed Time
CI, confidence interval; SD, standard deviation.
Table 2 shows the percentage compliance of stationary and moving CPR in relation to the 2015 ILCOR Guidelines. The table provides the standard for each of the ILCOR criteria, as well as the percentage compliance to each component for stationary and moving CPR.
Percentage Compliance with 2015 International Liaison Committee on Resuscitation Cardiopulmonary Resuscitation Parameters
CCF, chest compression fraction; ILCOR, International Liaison Committee on Resuscitation.
Figure 2 demonstrates the differences between stationary CPR (light gray) and moving CPR (black) in terms of the mean percentage of compressions delivered to a depth of 5–6 cm. The difference is statistically significant (p < 0.0001). There were large differences, but both stationary and moving compressions met ILCOR guidelines for depth. In addition to the difference between stationary and moving depth compliance, a reduced compliance in the stationary CPR was noted.

Paired depth compliance of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario.
Figure 3 shows that 9 of 30 subjects exceeded a mean of 6 cm of compression depth while stationary, 6 were too shallow and 15 were within the standard. In 20 cases, the mean depth of compressions when moving was shallower than when stationary. Eight subjects had deeper compressions when moving, and two subjects compressed at virtually the same mean depth.
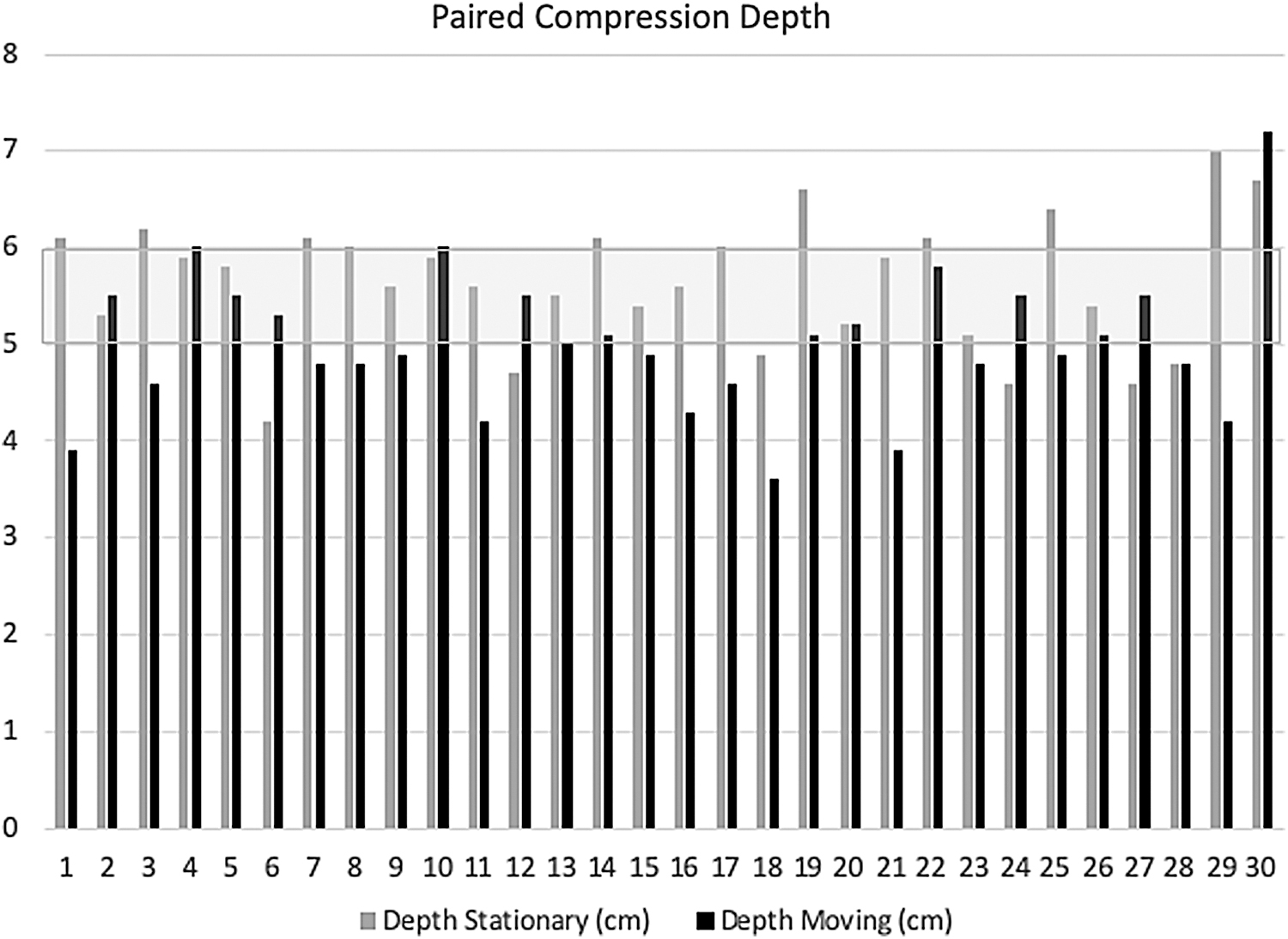
Paired compression depth (cm) of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario.
There was a statistically significant difference in maintaining a compression rate of 100–120 compressions per minute when moving versus stationary (p < 0.001). Figure 4 compares moving versus stationary compliance by subject. Twenty-three of the 30 subjects were compliant greater than 80% of the time when stationary. However, when moving, only 9 of 30 met the standard more than 80% of the time. Compressing at a rate of greater than 120/min was more common in the moving scenario and was the primary reason for noncompliance. These data were calculated by the TrueCPR which presented the number and percentage of compressions at the target rate and the number and percentage of compressions that were too fast or too slow.
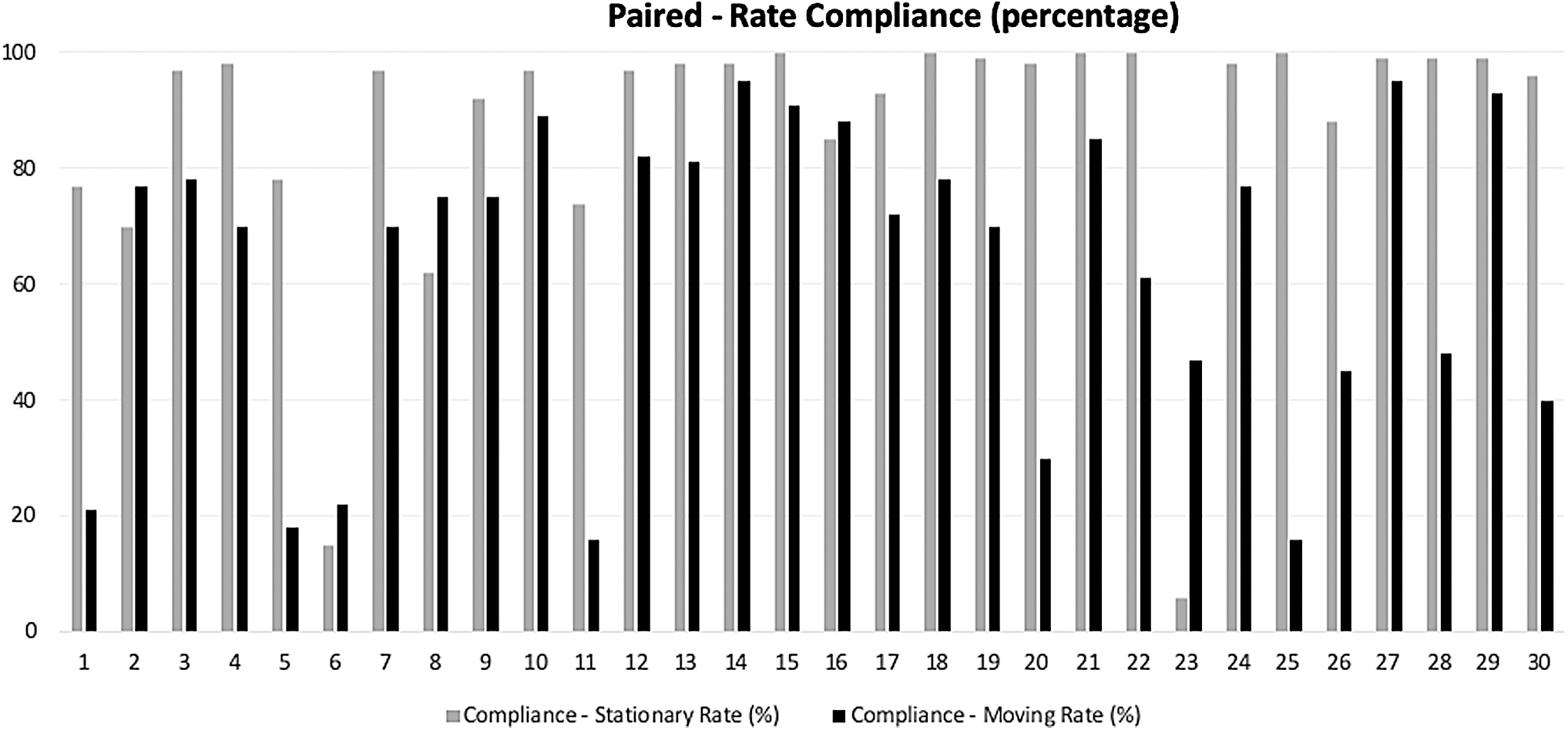
Paired rate compliance (using ILCOR guidelines) of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario. ILCOR, International Liaison Committee on Resuscitation.
Figure 5 shows that the mean stationary rate was 110.7/min, with standard deviation (SD) 7.96, while the mean moving rate was 116.7/min, with SD 8.7. When stationary, 27 of 30 subjects compressed at a rate within the ILCOR standard. When moving 20 of 30 subjects were compressing at the target rate range. This difference was also statistically significant (p = 0.007).
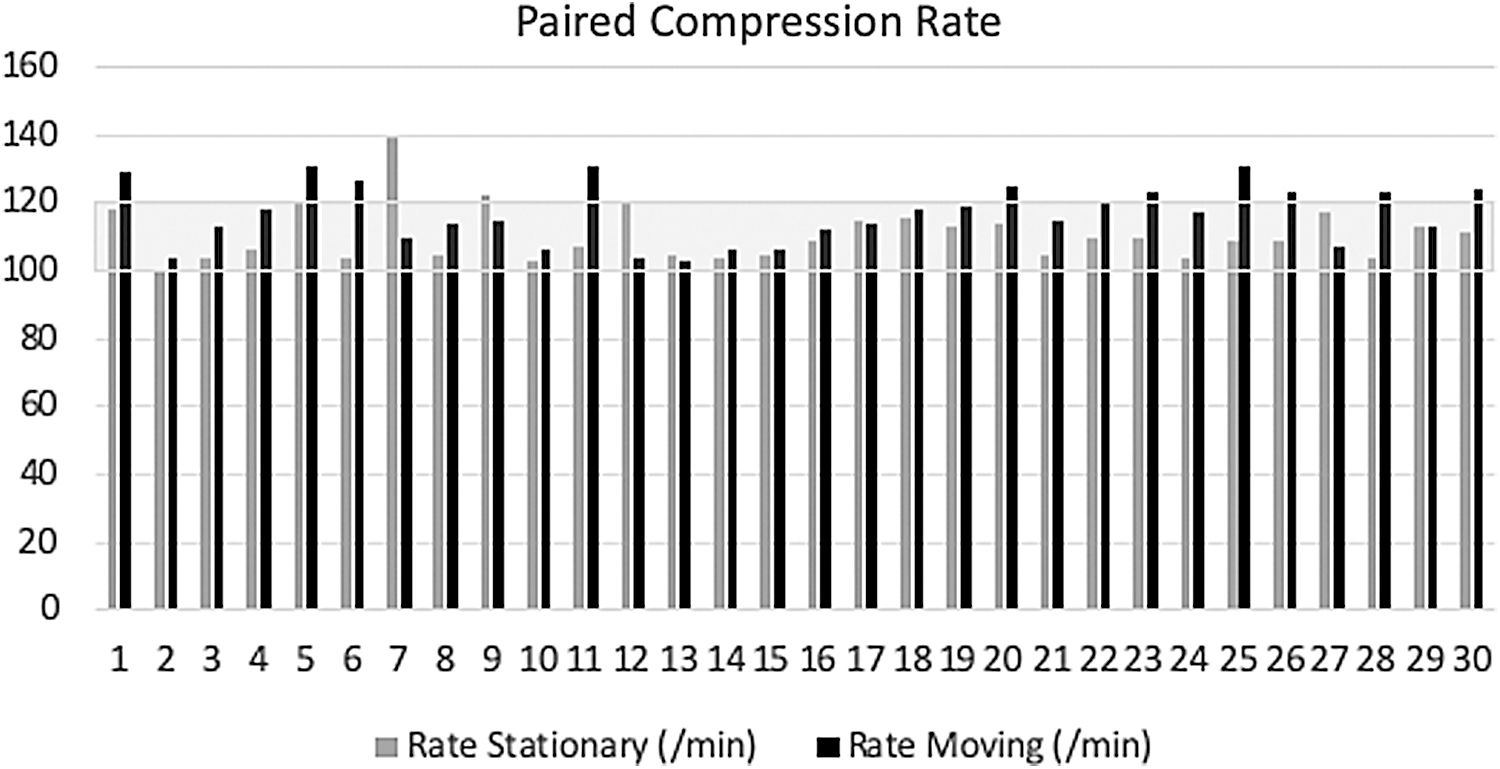
Paired compression rate of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario. ILCOR guidelines are shown with stippling. The box shows the paired compression rates and demonstrates their similarity despite whether they are moving or stationary.
Chest recoil was measured by the TrueCPR and presented as a percentage of compressions that allowed for full re-expansion of manikin's chest between compressions. Figure 6 shows that full chest recoil was achieved for 74.0% of stationary compressions, while full recoil was achieved in 77.1% of moving compressions. The difference was found to not be statistically significant (p = 0.65).
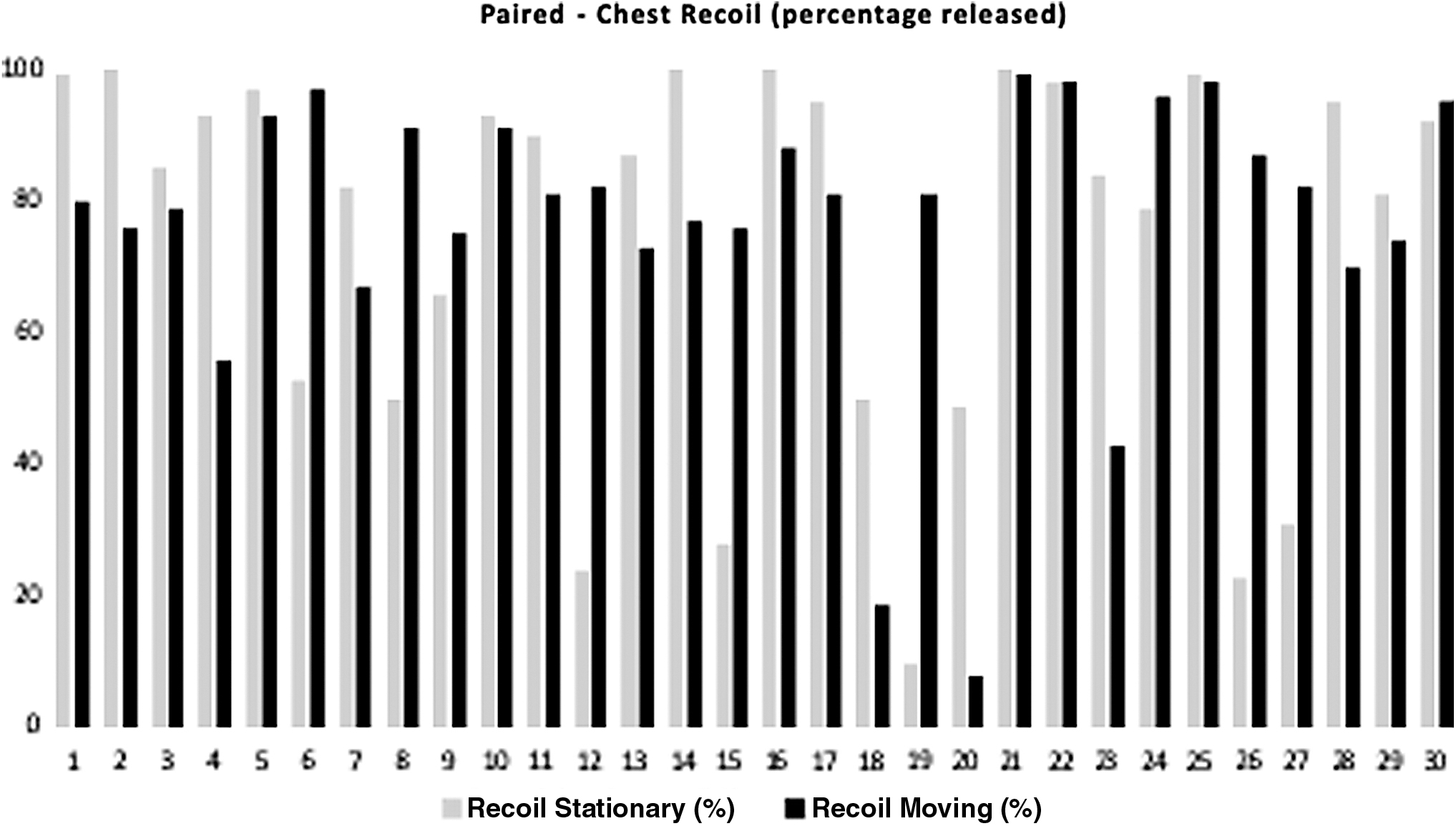
Paired chest recoil (percentage released) of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario.
There were no pauses over 10 seconds once compressions were started, in either the stationary or moving phases of the study.
The starting point for calculation of chest compression fraction (CCF) was from the first compression on the manikin's chest to stopping compressions and turning off the TrueCPR at the end of the toboggan run or at the end of the five sets of compressions when stationary. Figure 7 shows that CCF was very high for stationary CPR (mean 99.8%). CCF was relatively high during the moving phase (mean 94.5%) with two subjects having a CCF of 73% and 74% during their runs. The difference was statistically significant (p = 0.002).

Paired chest compression fraction (percentage) of single patrollers (n = 30) doing CPR on a manikin. The patrollers were either in a stationary position or on the hill in a moving scenario.
Discussion
The relationship between the quality of CPR and cardiac arrest survival has been well established (Tomlinson et al., 2007; Steill et al., 2012, 2014; Talikowska et al., 2015). The 2015 ILCOR Guidelines were the first to define both a minimum compression depth and a maximum compression depth for adults, as well as compression rates, recoil, and other parameters comprising effective CPR (Nolan et al., 2015).
We noted a reduction in standard-compliant compression depth when CPR was performed outside, wearing weather-appropriate clothing, even in the stationary toboggan. The authors anticipated that all subjects would be able to achieve high compliance when stationary rather than just 8 out of 30 subjects exceeding 80%.
Others have found compression depth compliance ranging from 46% compliance (Cheskes et al., 2016) to 89% compliance (Chew et al., 2018). The subjects in our study had never trained or practiced providing CPR in winter conditions. There may be benefits in training patrollers utilizing both high fidelity manikins and encouraging CPR practice while wearing their usual outdoor clothing to improve these results.
Unlike our results, studies of CPR while moving have been focused on situations in the EMS environment: providing CPR on a moving stretcher or CPR in a moving ambulance (Kim et al., 2006; Park et al., 2016; Russi et al., 2016). To our knowledge, this is the second study of CPR quality during toboggan transport in the ski patrol mountain setting. Thomassen et al. (2017) found no significant difference in CPR compression rate, depth, or recoil in stationary versus moving testing, unlike these results which did show significant differences. We did find, as they did, that compression depth and recoil showed significantly larger variance during the moving phase.
There are many differences between the study of Thomassen et al. (2017) and ours. Our stationary setting was outdoors, rather than indoors, and their method of transport was with snowmobiles pulling toboggans instead of ski patrollers. We used a longer active ski run (1.5 km vs. 1.1 km) with more vertical drop (440 m vs. 204 m) and three pitch changes during the run rather than a snowmobile track. These factors may have contributed to more difficulty performing compliant CPR in the moving phase.
There was a significant decrease in the number of compressions of standard-compliant depth when moving in a toboggan, compared to stationary CPR. Pushing too deeply (greater than 6 cm) was often the cause of noncompliant compressions when stationary. Compressing too lightly (less than 5 cm) was the issue for patrollers when moving in the toboggan. However, the differences between compliant and noncompliant compression depth were often within single digit millimeters. A combination of feedback and coaching may improve compression depth compliance in either scenario.
Similarly, there was a significant difference in compression rate when moving compared to when stationary, although most subjects still met ILCOR guidelines. Occasionally, while moving downhill, the compression rate exceeded the 120 compressions per minute standard (Idris et al., 2012; Nolan et al., 2012). This may have been due to a compensatory speeding up of compressions if they were momentarily paused for the patroller to hold on while going over a terrain change or when reestablishing balance.
The manikin was positioned with the head uphill at the back of the toboggan and the patroller kneeling and straddling the manikin, facing uphill. This position was chosen based on data from tilt table experiments with a porcine model, which found that cerebral blood flow was better when the head was up, compared with level or head-down position (Debaty et al., 2015; Frascone, 2017). This was confirmed in a recent study by Pepe et al. (2019), showing a doubling of patient survival when CPR was performed in a head/torso up position bringing patients to hospital, by trained paramedics.
The narrowness of the toboggan made it difficult for some subjects to find a comfortable position with their knees inside the toboggan walls. The physical size of the patroller and the manikin may be important for the patroller's ability to perform compliant compressions. Some patrollers experienced profound movement along the manikin's body during toboggan transport. Good body mechanics for compression at the start of the run (Fig. 8) often deteriorated into less ideal mechanics by the end. The patrollers slid downhill away from the manikin's chest ending in a bent-knee pushup position (Fig. 9). A strap placed and secured across the bottom of the patrollers' boots as a footrest may help reduce this movement. This technique was not tested here but could be assessed in future studies.

Starting position of patroller in the toboggan doing CPR as the toboggan moved downhill during the moving portion of the study. Note the knees start directly under the hips of the patroller.

Final position of patroller in the toboggan doing CPR as the toboggan finished the moving portion of the study. Note the knees are no longer under the hips of the patroller but very stretched out.
The speed and skill of the toboggan drivers differed among drivers and likely affected the quality of CPR. The drivers had to maintain control, deliver a smooth straight ride, use the chain braking system when necessary, and still reach the base of the run quickly, as they would in a real situation. The drivers were directed to choose a route down the most constant slope of the ski run and to make any changes in direction as gradual as possible to minimize side to side motion. Route selection is important; the fastest route may not allow provision of quality CPR along the route.
The use of metronomes, gauges, lights, and other devices has been investigated for their effect on improving CPR performance by providing feedback to the compressor (Chest Compression Feedback, 2015). Many of these aids are available on the TrueCPR. All were in operation during both phases of the study. The visual indicators of the TrueCPR device were obscured by hand position while wearing gloves/mitts or blanked out by the high ambient light levels. The audibility of the metronome was affected by wind noise across the patroller's helmets and the sounds generated by the toboggan moving over the snow. In this study, most subjects commented that there was no perceived benefit of the audiovisual aids to their performance of CPR, particularly in the moving portion of the trial.
The strengths of this study include its ability to assess the quality of CPR performance objectively and in relation to a clear definition of quality. The definition had both a minimum standard and a maximum standard for compression depth and rate. The instrumentation used was calibrated to both limits. The study was conducted under “real world” conditions and was filmed to determine dynamic changes during the study. By having the participants perform both phases within 60 minutes, possible confounding effects of differing manikin temperature and weather conditions were eliminated.
Limitations
There were some limitations in this study. The sample size of patrollers was small and drawn from a single ski resort. There was no ability to blind the subjects to the stationary versus the moving phases of the trial. The testing was performed over four separate days, under a variety of weather conditions, but we did not analyze the data in relation to the weather conditions.
Each toboggan driver had different skills, so it was not possible to ensure consistent rides between subjects, apart from using the same ski run and start/finishing points on that run. Only one method of performing CPR in a moving toboggan was studied. There have been anecdotal reports of other methods (Association of Professional Patrollers, 2012), but these were not evaluated. The manikin was the size of a small adult but weighed less. This may under-represent the weight challenges for both the toboggan driver and the kneeling patroller in a moving toboggan on a ski slope. Although the TrueCPR provided real-time feedback during the performance of CPR, it could not be utilized by subjects.
Accuracy of hand position over the sternum during chest compressions was not independently evaluated; poor position could contribute to noncompliant compressions. The duration of CPR while moving was longer than in the stationary scenario. It is possible that the degradation of compression depth may have been due to fatigue. There was no randomization between the two phases of the study; all subjects first performed CPR in the stationary situation, then in the moving toboggan. There may have been a consistent learning effect between these two phases of the study. We recognize that adequate ventilation and oxygenation (by rescue breaths or high flow passive oxygen administration) are necessary for successful CPR over a prolonged time period (Sayre et al., 2008). This was not the focus of this study and our patrollers may have found this difficult in a moving toboggan. It is worthy of further study.
Conclusions
Effective CPR in a moving toboggan is feasible, even in winter conditions on a ski slope. Although CPR quality is reduced while moving, there were sufficient compliant compressions to support the use of CPR in this setting. Maintaining body position in relation to the patient may be a key to improving the quality of CPR in a moving toboggan. Regular CPR training in outdoor “real world” environments may be beneficial.
Footnotes
Acknowledgments
The authors wish to recognize the assistance of the staff and management of the Nakiska Ski Resort for their encouragement and participation in this study. The authors recognize the support of members of the Nakiska Ski Patrol who participated. The authors also thank Dr. Richard Buckley, MD, FRCS for his advice, suggestions, critique, and editing of this article.
Authorship Confirmation Statement
T.A. conceived of the project, set up experiment, performed experiment, wrote article, and established references. L.T. conceived of the project, set up experiment, performed experiment, wrote article, and established references. Both authors have reviewed and approved of the article prior to submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.