
Abstract
Background:
Perfusion of intrapulmonary arteriovenous anastomoses (IPAVA) is increased during exercise and in hypoxia and is associated with variations in oxygen saturation (SPO2), resulting in blood bypassing the pulmonary microcirculation. Sildenafil is a pulmonary vasodilator that improves SPO2 and endurance performance in hypoxia. The purpose of this study was to determine if 50 mg sildenafil would reduce IPAVA perfusion (QIPAVA) and if the decrement in maximal exercise capacity (VO2max) in hypoxia is related to QIPAVA. We hypothesized that during progressive levels of hypoxia at rest (FIO2 = 0.21, 0.14, 0.12), sildenafil would increase SPO2 and reduce bubble score (estimate of QIPAVA) compared to placebo, and that the decrement in VO2max in hypoxia would be positively correlated with bubble score at rest in hypoxia.
Materials and Methods:
Fourteen endurance-trained men performed a graded maximal exercise test at sea level and at a simulated altitude of 3000 m, followed by two experimental visits where, after randomly ingesting sildenafil or placebo, they underwent agitated saline contrast echocardiography during progressive levels of hypoxia at rest.
Results:
All participants experienced a decrement in power output in hypoxia that ranged from 9% to 19% lower than sea level values. Compared to normoxia, bubble score increased significantly in hypoxia (p < 0.001) with no effect of sildenafil (p = 0.580). There was a negative correlation between SPO2 and bubble score (p < 0.001). The decrement in peak power output at VO2max in hypoxia was unrelated to IPAVA perfusion in resting hypoxia (p = 0.32). Several participants demonstrated QIPAVA greater than zero in room air, indicating that arterial hypoxemia may not be the sole mechanism for QIPAVA.
Conclusion:
These results indicate that the VO2max decrement caused by hypoxia is not related to QIPAVA and that sildenafil does not improve VO2max in hypoxia through modulation of QIPAVA.
Introduction
The existence of intrapulmonary arteriovenous anastomoses (IPAVA), blood vessels that bypass the pulmonary microcirculation, has been well described in the literature (Tobin, 1966). More recently, researchers have attempted to quantify the perfusion of these IPAVAs (QIPAVA) using injected microspheres in dog (Stickland et al., 2007) and human (Lovering et al., 2007) lungs, and transthoracic contrast echocardiography (Eldridge et al., 2004), among other techniques (Duke et al., 2015). While some humans display evidence of QIPAVA at rest (Elliott et al., 2013; Duke et al., 2015), the majority of participants experienced increased QIPAVA during increasing levels of exercise (Eldridge et al., 2004; Lovering et al., 2009b) and normobaric hypoxia (Lovering et al., 2008a; Laurie et al., 2010), which can be almost completely abolished with hyperoxia (Lovering et al., 2008b).
The impact of IPAVA on gas exchange has not been demonstrated experimentally. Research using labeled aggregated albumin has estimated that IPAVAs are responsible for a mean 1.2 ± 0.8% anatomic shunt in humans (Lovering et al., 2009b) and 1.42 ± 0.75% shunt in dogs using microspheres (Stickland et al., 2007). The impact of this anatomic shunt on gas exchange is unclear. Research using the multiple inert gas elimination technique (MIGET) and 100% oxygen methods has not demonstrated an impact of intrapulmonary shunt on the alveolar-arterial oxygen difference (A-aDO2) (Wagner et al., 1986; Hopkins et al., 1994, 1996), suggesting that the observed A-aDO2 during exercise is the result of pulmonary ventilation/perfusion heterogeneity and diffusion limitation (Dempsey and Wagner, 1999; Hopkins, 2006).
While the hemodynamic significance of increased QIPAVA is unclear, its mechanism has also been the subject of extensive experimentation. Increases in QIPAVA during exercise and hypoxia were initially attributed to be the result of increases in pulmonary artery pressure (PAP) and cardiac output (CO) (Stickland et al., 2004); however, more recent evidence that changes in QIPAVA occur independent of PAP and CO manipulations suggests that direct sensing of hypoxia itself is a major controller (Lovering et al., 2015; Tremblay et al., 2015; Duke et al., 2016). Although increased QIPAVA is correlated with a reduction in SPO2 (Laurie et al., 2010), it is unclear the extent to which QIPAVA is affected by redistribution in pulmonary blood flow, the hypoxic (HYP) stimulus, an unknown stimulus, or some combination.
While the effect of exercise as a mediator of QIPAVA is well described in the literature (Lovering et al., 2009b), less is known about the relationship between exercise capacity and QIPAVA. La Gerche et al. (2010) found that subjects with low bubble scores (0–2) had a lower mean VO2max in normoxia compared to those with higher bubble scores (3–5), with no effect on SPO2. While Norris et al. found age (<50 years) to be associated with greater QIPAVA, they did not find any significant difference in VO2max between high and low bubble scores. If both exercise performance in hypoxia (Chapman, 2013) and QIPAVA are modulated by variation in SPO2, we would expect to see some relationship between the two. Alternatively, if increased QIPAVA is in fact associated with increased VO2max in normoxia, but not negatively affecting the A-aDO2, it is possible that increased QIPAVA could be associated with improved performance in hypoxia.
Several studies have hypothesized that vasoactive drugs may increase QIPAVA directly through their vasodilatory properties. Nitroglycerine, norepinephrine, and aminophylline had no effect on QIPAVA in resting participants in normoxia (Lozo et al., 2014). Sildenafil, nifedipine, and acetazolamide had no effect on QIPAVA in resting participants inspiring 100% O2 (Elliott et al., 2014). In both of these studies, participants had normal values of resting sea level SpO2, which may account for the lack of effect on QIPAVA. It is possible the chance of observing an effect using some or all of these medications may be greater in HYP conditions.
Sildenafil citrate inhibits phosphodiesterase type-5 from degrading cyclic guanosine monophosphate (cGMP), promoting pulmonary smooth muscle relaxation through reduced intracellular calcium levels as part of the nitric oxide pathway. Several studies have shown an improvement in endurance performance in hypoxia as a result of orally administered sildenafil (Ghofrani et al., 2004; Richalet et al., 2005; Snyder et al., 2008). These reports suggest that improved endurance performance is related to an increase in SPO2 caused by a decrease in PAP, which reduces right ventricular afterload, and increases CO (Ghofrani et al., 2004; Faoro et al., 2007); however, the mechanism(s) for improved performance remain unclear (Carter et al., 2019a).
As sildenafil has been shown to increase SPO2, and QIPAVA appears to be at least partially regulated by SPO2, it is possible that QIPAVA could be stimulated by sildenafil, either directly through its vasodilatory properties as hypothesized by Elliott et al. (2014) or indirectly by sildenafil-induced increases in SPO2. The purpose of this study was to determine if a therapeutic dose (50 mg) of the pulmonary vasodilator sildenafil could be used to reduce QIPAVA during hypoxia at rest. The secondary purpose was to explore the relationship between QIPAVA at rest and the decrement in power output at VO2max in hypoxia.
Hypothesis
During progressive levels of hypoxia at rest (FIO2 = 0.21, 0.14, 0.12), sildenafil will increase SPO2 and reduce the QIPAVA (as estimated by bubble score) compared to placebo. In addition, the reduction in power output at VO2max in hypoxia will be positively correlated with bubble score at rest in hypoxia.
Materials and Methods
Sixteen male competitive cyclists were recruited, and after screening for patent foramen ovale, 13 participated in the study. All participants resided below 150 m above sea level and had not travelled above 2000 m (excluding commercial air travel) in the preceding 6 months. The nature of the terrain around the South Coast of British Columbia is such that occasional short exposures (e.g., driving over mountain passes) to altitudes of 1000–1800 m occur, but are brief and uncommon, so the participants were considered residents of sea level and altitude naive. Participants maintained a consistent volume of endurance training (five sessions per week for more than 1 year) and competed regularly in endurance cycling or triathlon (≥3 competitions per year). The study was approved by the Clinical Research Ethics Board at the University of British Columbia and all procedures were in accordance with the ethical standards of the 1964 Helsinki Declaration. Participants were informed of the procedures and possible risks involved in the study and informed consent was obtained.
Participants visited the University of British Columbia Environmental Physiology Laboratory on three occasions. During the first visit, participants completed two graded maximal exercise tests on a magnetically braked cycle ergometer (Velotron, Racermate, SD) under a normoxic (NOR; FIO2 = 0.209) and normobaric HYP condition (FIO2 = 0.147, equivalent to a simulated altitude of 3000 m).
The HYP exercise condition was produced using a custom HYP enclosure (Colorado Altitude Training, CO) that reduces the O2 concentration of room air and delivers it to the participant using large bore tubing and a one-way non-rebreathing valve with breathing mask (Hans Rudolph, KS). The HYP enclosure was programmed to deliver an FIO2 of 0.14; however, mean FIO2, as measured by fast response O2 gas analyzer (Vacumed, CA), was 0.147. The order of the tests in the HYP and NOR condition was randomized. Workload started at 100 W and increased in a ramp manner by 1 Watt every 2 seconds until exhaustion. During the test procedure, respiratory gases were collected using fast response O2 and CO2 gas analyzers and a pneumotachometer (Vacumed). Participants' SPO2 and heart rate (HR) were collected with a Nonin 9600 ear clip pulse oximeter (Nonin Medical, MN). The signals from these devices were stored digitally on a PowerLab data acquisition system (ADInstruments, Dunedin, New Zealand) and averaged every 10 seconds.
During the two remaining visits, participants completed experimental trials with either the placebo or study medication, sildenafil, using a double-blinded, randomized crossover design. Sildenafil was administered as a single oral dose of 50 mg. This dose is used most commonly in studies of athletic performance in hypoxia and was previously shown to elicit a decrease in PAP (Carter et al., 2019a). Participants and researchers were blinded to the condition and medication. The placebo and sildenafil capsules were compounded locally (McDonalds Pharmacy, British Columbia, Canada) and were indistinguishable. Study sessions were completed a minimum of 7 days following maximal exercise testing and with 7 days between each session.
Experimental visits began with a 4 mL venous blood draw followed by ingestion of a placebo or sildenafil capsule with a glass of water. At 46 ± 3 minutes after ingestion, participants underwent a second blood draw and a venous catheter was inserted in the right forearm. Participants were placed in a recumbent semi-left lateral decubitus position on an examination table and outfitted with the same one-way non-rebreathing valve and mask (Hans Rudolph) used for the exercise component, with gas supplied through large bore tubing from a mixing chamber connected to a pressurized gas canister containing varying concentrations of O2 (FIO2 = 0.21, 0.14, and 0.12, equivalent to a PIO2 of 148, 98, and 84 mmHg, respectively). These exposure levels were chosen to correspond to altitudes of sea level, 3000 m, and 4500 m, common moderate altitudes at which athletes compete. Participants were fitted with the pulse oximeter and expired gasses were collected with the same analyzers used in the exercise component.
At 62 ± 3 minutes after ingestion of the study capsule, participants began breathing gas supplied by the mask, while lying quietly, and recording equipment was started. An apical view of the heart was obtained using a Vivid I ultrasound and 3S cardiac probe (General Electric, MA). Ventilatory data were recorded throughout the entire testing protocol, but only minutes 10–14 were included in the analysis. At 15 ± 1 minutes of breathing, a bolus of agitated saline contrast (1 mL air in 4 mL saline) was forcefully injected into the venous catheter. The passage of the contrast solution through the pulmonary circulation was recorded using the ultrasound from the moment of injection through ∼20 cardiac cycles and saved for posttest analysis by two blinded reviewers. As soon as recording was complete for the FIO2 = 0.21 condition, the procedure was repeated using the remaining levels of HYP gas (FIO2: 0.14 and 0.12) in order.
Ultrasound videos were stripped of identifying data and coded using a simple number system in a randomized order (1–81), and then distributed digitally to the reviewers who scored the presence of IPAVA according to the bubble score grading system described by Lovering and Goodman (2012). Bubble score uses a scale of 0–5 with the score approximating QIPAVA, depending on the amount of contrast that bypasses the pulmonary circulation and re-enters the left heart. The number of cardiac cycles between appearance of saline contrast in the right heart and left was counted. Three participants were excluded from participation after contrast appeared in the left heart in ≤3 beats on suspicion of patent foramen ovale. Two blinded raters scored all 81 video files, resulting in identical scores for 70 videos and a one-point disagreement on the remaining 11 videos. These 11 were rescored by a third blinded rater and the mode value of all three raters was used for the analysis. An enzyme-linked immunosorbent assay (BioScientific) was used to quantify serum cGMP in the predrug and postdrug blood samples.
Statistical analysis
All data are presented as mean ± standard deviation, unless specified. Due to the nonparametric nature of the bubble score, Friedman's test was used to evaluate the effect of FIO2, sildenafil, and their interaction. To assess the effect of sildenafil on bubble score, for each treatment, the within-subject mean of bubble score across the three FIO2 levels was used. To examine the impact of FIO2 on bubble score, mean bubble score was calculated across the two treatments for each subject by FIO2 level. To evaluate the interaction (FIO2 × treatment), the within-subject difference between bubble score from the two treatments by FIO2 levels was used. For the remaining parametric variables, a two-way analysis of variance (ANOVA) with repeated measures was used. When the ANOVA revealed a significant main effect, a post-hoc Tukey-Kramer test was performed to identify differences. A linear mixed effects regression model was used to determine the relationship between SPO2 and bubble score. Spearman's rank order correlation (ρ) was used to compare the relationship between bubble score and the decrement in power output. Statistical significance was considered when p < 0.05.
Results
Participants' age, height, and body weight were 32 ± 11 years, 180 ± 7 cm, and 78.8 ± 11.6 kg, respectively. Participants' mean VO2max at sea level was 60.0 ± 11.0 mL/kg/min. Mean VO2max in hypoxia was 44.6 ± 10.1 mL/kg/min. Serum cGMP was significantly greater in the sildenafil group (p < 0.001) compared to pretest values and placebo (Table 1).
Effects of Sildenafil on Metabolic and Hemodynamic Variables in Normoxia and Hypoxia
Values are presented as mean ± standard deviation.
Data presented as median (interquartile range).
p < 0.01, main effect of FIO2.
p < 0.001, main effect of FIO2.
p < 0.01, main effect of drug.
p < 0.001, main effect of drug.
BP, blood pressure; MAP, mean arterial pressure; Fb, breathing frequency; VT, tidal volume; FIO2, fraction of inspired oxygen; VE, ventilation; VO2, oxygen uptake; SPO2, oxygen saturation; HR, heart rate; cGMP, cyclic guanosine monophosphate.
There was a significant increase in bubble score in hypoxia (p < 0.001; Fig. 1), but there was no effect of sildenafil on bubble score (p = 0.763; median difference: −0.17 [95% confidence interval, CI: −0.67 to 0.33]) or SPO2 (p = 0.580; median difference: −0.06 [95% CI: −1.22 to 1.10]). Sildenafil significantly increased HR (p < 0.01) and showed a trend toward increasing VO2 (p = 0.127), especially at lower FIO2 (0.14 and 0.12). Sildenafil had no effect on systemic BP (Table 1).
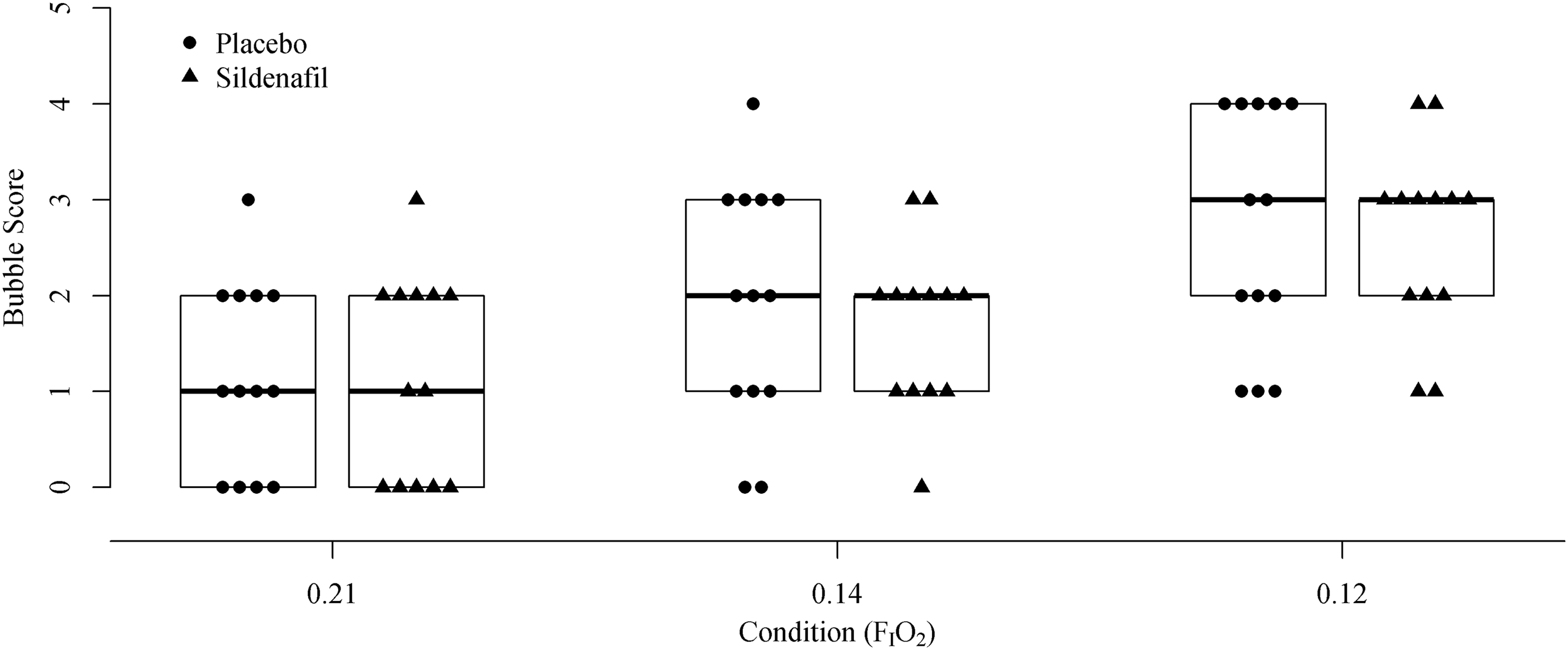
Bubble score in varying levels of hypoxia with placebo and sildenafil. Brackets indicated median and first and third quartile. FIO2, fraction of inspired oxygen.
The relationship between SPO2 and bubble score differed significantly by FIO2 level (p < 0.001) (Table 2), but not by treatment group (p = 0.732). There was a significant negative relationship when FIO2 = 0.12 (p < 0.001; Fig. 2). There was no difference between the SPO2 for bubble scores 0–2 and 3–5 in room air; however, at an FIO2 of 0.12, SPO2 for bubble scores 0–2 was significantly higher than for scores 3–5 (p < 0.001; Fig. 3).
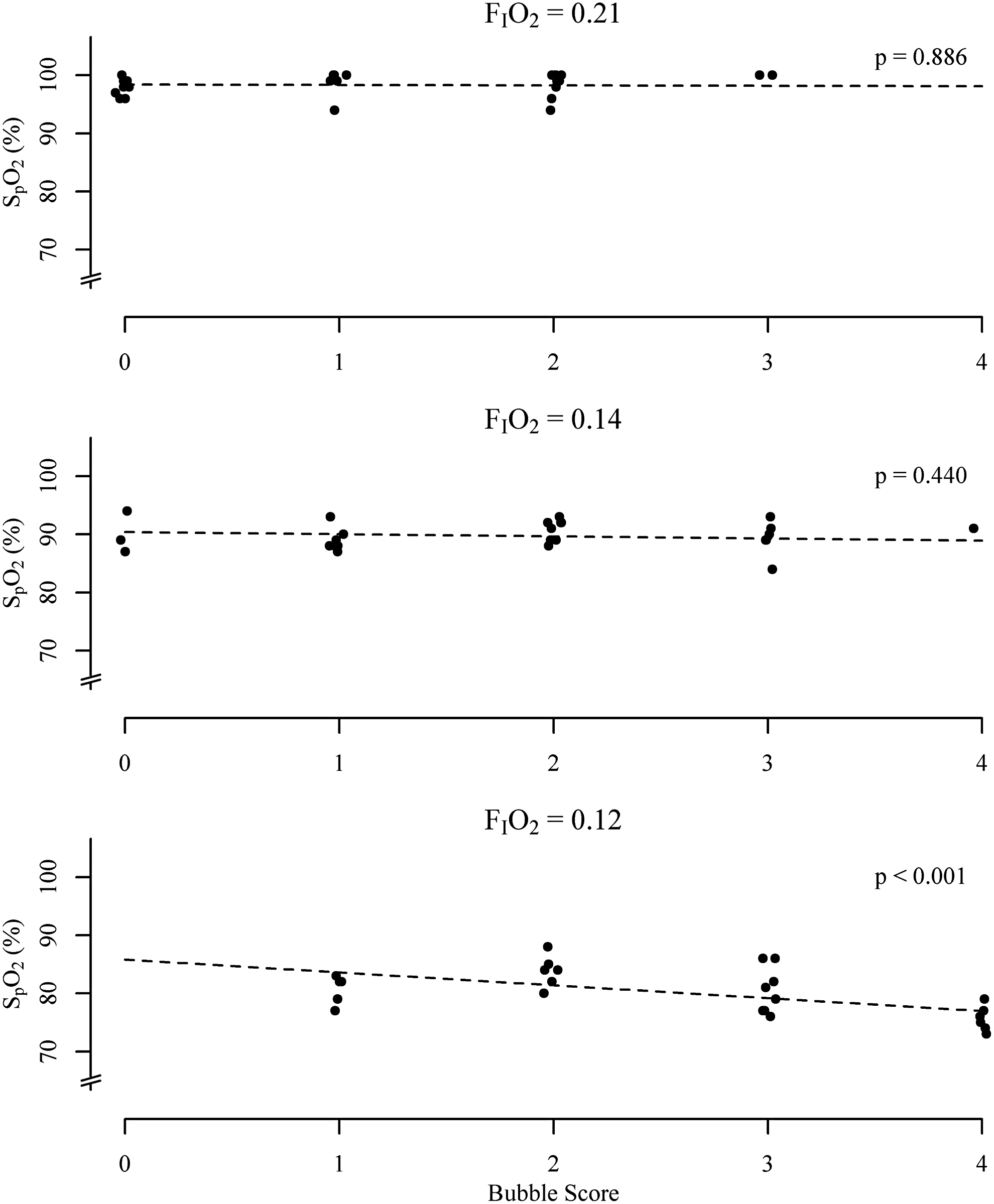
Linear mixed effect regression relationship between bubble score and oxygen saturation. SPO2, oxygen saturation.
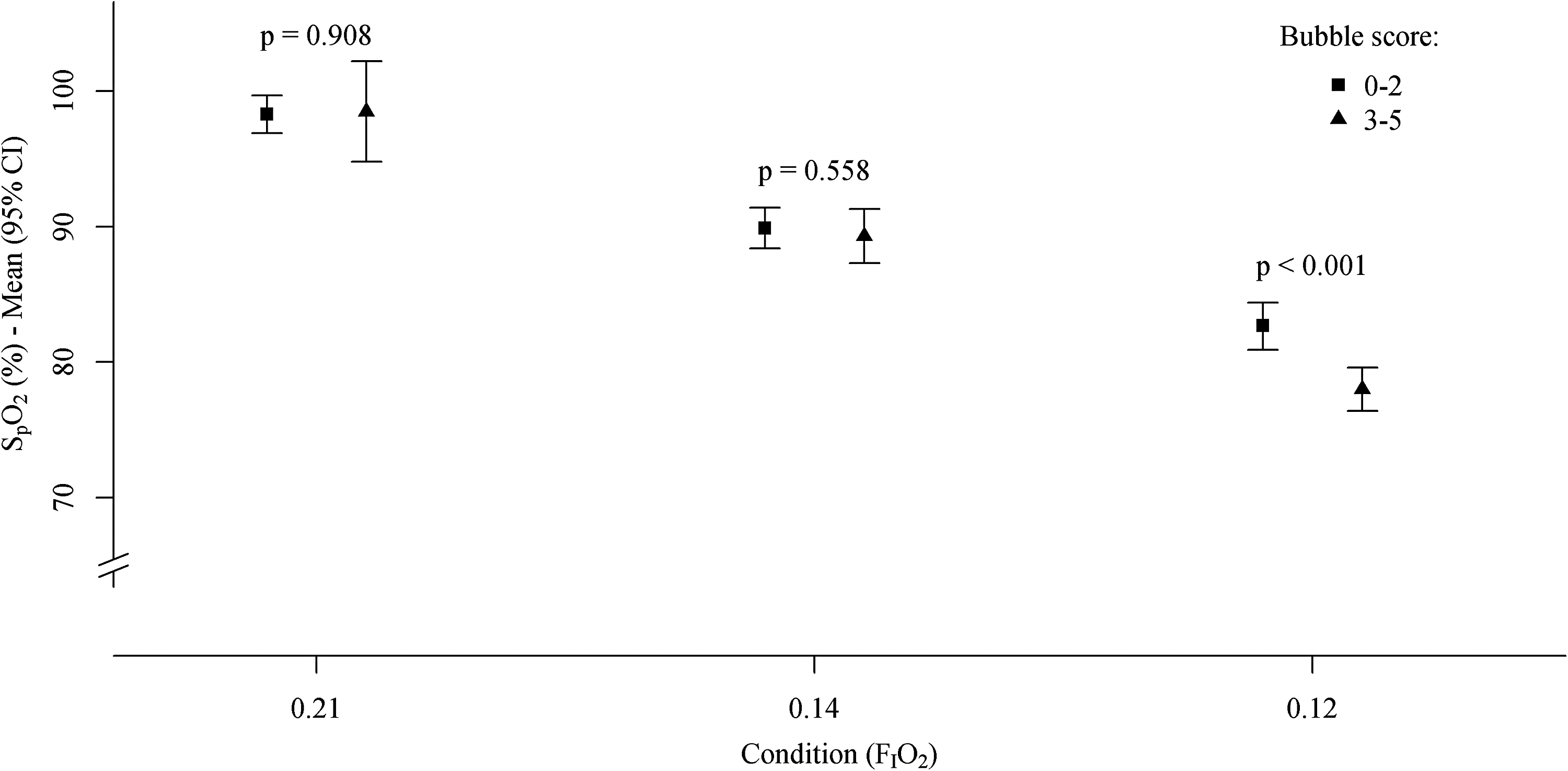
Mean oxygen saturation in high and low bubble scores at each level of hypoxia (0.21, 0.14, and 0.12). Error bars indicate 95% CI. CI, confidence interval.
Results from Linear Regression Analysis
CI, confidence interval.
All participants experienced significantly impaired (p < 0.0001) peak power output during exercise in hypoxia (353.8 ± 41.8) compared to normoxia (413.5 ± 55.1 W). The decrement in power output at VO2max (% of sea level power output in watts) ranged from a 9% to 19% below sea level values (Fig. 4). The decrement in power output in VO2max was unrelated to QIPAVA in resting hypoxia with placebo (ρ = −0.33, p = 0.32) or sildenafil (ρ = −0.38 p = 0.24).
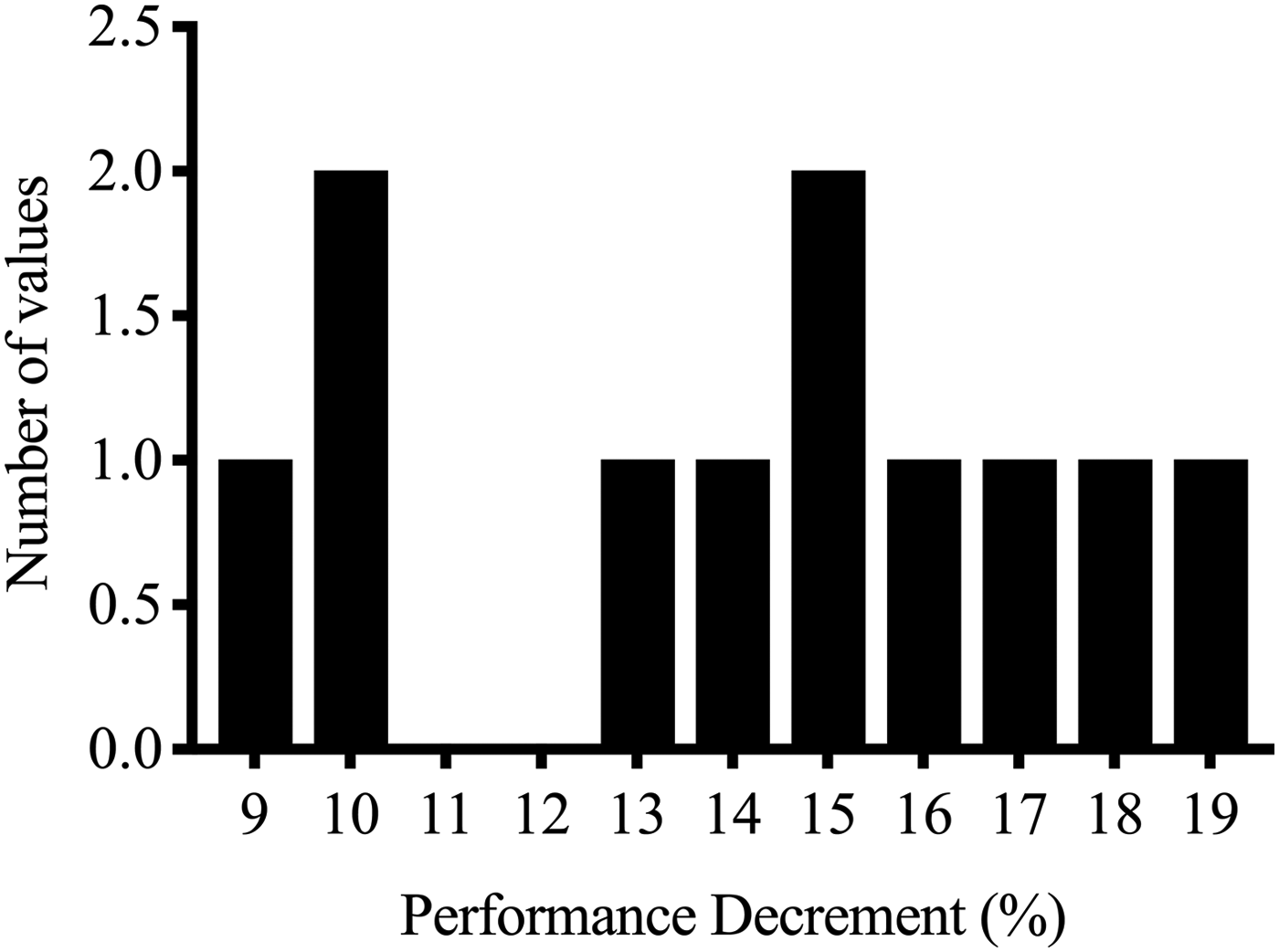
Histogram showing individual VO2max decrement in hypoxia in all athletes.
Discussion
As a result of our intervention, we observed small, but consistent systemic effects of sildenafil. There was no effect of sildenafil on systemic BP, but HR was significantly increased with sildenafil at every level of hypoxia. This has been attributed to a sympathetic response to sildenafil's reflex vasodilatory effect and has previously been reported in rats (Fazan et al., 2008). The trend for increased VO2 with sildenafil in hypoxia and normoxia suggests a small increase in metabolic rate that would typically be met with an increase in CO, supported by the observed increased HR. This increase in CO (compared to placebo in hypoxia where CO is limited) could raise SaO2 and exercise tolerance, but the difference may be very small and statistically insignificant. While elite athletes often seek marginal gains in the fraction of a percentage, the lack of an effect on endurance performance indicators is supported by several studies that found no ergogenic effect of sildenafil (Faoro et al., 2007; Jacobs et al., 2011; Kressler et al., 2011; Carter et al., 2019b).
We observed a greater bubble score under resting, HYP conditions when compared to normoxia. We interpret this to mean that exposure to increasing levels of hypoxia elicits an increase in QIPAVA. We discussed two possible mechanisms for sildenafil to increase QIPAVA, either through (i) direct vasodilation of IPAVA vessels or (ii) indirectly by increasing SPO2, one of the primary determinants of QIPAVA. Consistent with work by Elliott et al. (2014), our data showed that sildenafil did not affect bubble score in the NOR condition. This result confirms that QIPAVA is not directly affected by the vasoactive effects of sildenafil. Because SPO2 remains at normal values during the NOR exposure, the indirect effect of sildenafil on SPO2 is inconsequential in normoxia and no change is to be expected. The first novel finding of this study is that sildenafil did not affect QIPAVA during exposure to moderate hypoxia. We found no statistical difference in SPO2 between a 50 mg dose of sildenafil and a placebo. These results suggest the effects of sildenafil on pressure and blood flow were insufficient to increase QIPAVA. While we did not measure pulmonary pressure or flow, if sildenafil did decrease PAP and increase CO as previously demonstrated, HYP sensing may play a greater role in regulation of QIPAVA than initially believed (contrary to the pressure/flow hypothesis), consistent with work by Laurie et al. (2010) and Tremblay et al. (2015).
Our second main outcome was the significant relationship between QIPAVA and SPO2. This relationship, while indirect, may help shed some light on the IPAVA sensor mechanism. While breathing sea level air (FIO2 = 0.21), SPO2 was 98%–100% in all participants, so we would not expect to see a correlation with bubble score in normoxia based on the narrow distribution in saturation. It was not until FIO2 was reduced to 0.12 that we saw variability in SPO2 that could be compared with the corresponding variability in bubble score. When the dataset was analyzed separately for each FIO2, the negative correlation between SPO2 and bubble score became significant. This supports evidence by Laurie et al. (2010), who found a correlation between SPO2 and bubble score at all levels of hypoxia combined. Had we used a comparably low FIO2 (0.10), the correlation between SPO2 and bubble score at rest may have been stronger.
When participants were sorted into low (0–2) and high (3–5) bubble score categories, high bubble score participants were found to have significantly lower SPO2. Despite a link between SPO2 and bubble score in hypoxia, several participants showed evidence of significant QIPAVA in resting normoxia. This has been previously reported by several studies (Kennedy et al., 2012; Elliott et al., 2013; Duke et al., 2015). Kennedy et al. (2012) attribute differences in QIPAVA to the importance of body position and the effect of tethering in the lung. All participants in our research eventually showed some degree of QIPAVA below a threshold SPO2 of 87%. While reductions in ambient PO2 directly result in increased QIPAVA, hypoxemia caused by exercise (which does not occur in some participants) is an alternative mechanism for increased QIPAVA.
The relationship between SPO2 and bubble score leads us to speculate on two possible conclusions. PaO2 may be the primary mediator of QIPAVA, especially if regional differences in PAO2 could potentially account for increased QIPAVA in normoxia during exercise when SPO2 is normal, as has been shown in several studies of exercise in normoxia (La Gerche et al., 2010; Lalande et al., 2012; Norris et al., 2014). A more likely (but still speculative) conclusion is that PaO2 is one of several modulating factors alongside PvO2, PAP, and CO.
Our final, and perhaps the most novel, observation was the relationship between QIPAVA in acute hypoxia and the effect of hypoxia on exercise performance. Exercise performance in hypoxia has been repeatedly shown to be determined by gas exchange impairments that result in variation in SPO2 (Chapman, 2013). Similarly, previous research and our own results presented above attribute increased QIPAVA to reductions in SPO2. If reduced SPO2 is implicated in both the decrement in exercise performance in hypoxia and QIPAVA, it is reasonable to expect that the two may be related. Despite both exercise performance in hypoxia and QIPAVA being modulated by SPO2, we found that the two are unrelated, which we believe indicates that, while blood flow through IPAVA does appear to bypass the pulmonary microcirculation, increases in QIPAVA are hemodynamically insignificant.
Limitations
Bubble score was our primary outcome variable; we did not measure PAP and CO at rest. The lack of a direct measure of pulmonary pressures prevented us from directly observing and quantifying the vasodilatory effect of sildenafil; however, it does not discount our observation that 50 mg of sildenafil did not affect bubble score. For future research, including these measures would allow researchers to eliminate the contribution of pulmonary pressure and blood flow to QIPAVA.
The agitated saline contrast echocardiography method of bubble score measurement has been thoroughly discussed in the literature (Hopkins et al., 2009; Lovering et al., 2009a; Lovering et al., 2015). While bubble score clearly is affected by certain stimuli, bubble score has not been directly correlated with shunt fraction measurements, and therefore, the overall hemodynamic significance of bubble score has yet to be demonstrated, and as such, we must be careful not to overstate our findings.
Pulse oximetry is a commonly used, noninvasive estimate of arterial oxygen saturation employing a light-emitting diode and receptor that isolate the pulsatile portion of light absorption, which represents arterial blood and correlates it with percent oxygen saturation (Mardirossian and Schneider, 1992; Chan et al., 2013). This estimation method results in a margin of error calculated at ±2% (Nonin 9600 Technical Manual). To minimize sources of error from the blood pressure cuff and intravenous site, SPO2 was measured at the ear lobe, the participant was kept warm using a blanket, and changes in body position were minimized.
Conclusion
The results of this study show that 50 mg of sildenafil does not significantly affect QIPAVA in normoxia or varying levels of hypoxia (FIO2 = 0.14, 0.12), as measured by bubble score. We identified a threshold SPO2 of 87%, below which all participants displayed perfusion of IPAVA. Several participants demonstrated QIPAVA above zero in room air, indicating that arterial hypoxemia may not be the sole stimulus for perfusion, but perhaps, some combination of PaO2 and PVO2. Perfusion of IPAVA at rest in hypoxia does not appear to be related to the decrement in power output at VO2max in hypoxia, despite the relationship with SPO2. Based on our results, we conclude that changes in QIPAVA do not cause changes in power output at VO2max in hypoxia, and athletes would see no benefit from the use of sildenafil to affect the QIPAVA.
Footnotes
Author Contributions
E.A.C.: Project conception, planning, data collection, analysis, and article preparation. S.K.: Planning, data collection, analysis, and article review. J.P.O.: Data collection, analysis, and article review. A.W.S.: Project conception, planning, and article review. W.K.M.: Project conception, planning, and article review. M.S.K.: Project conception, planning, data collection, analysis, and article review. We confirm that all coauthors have reviewed and approved the article before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.