
Abstract
Background:
Intermittent hypoxia/normoxia training (IHT) is considered a possible means to alleviate chronic diseases such as diabetes. In the last decade, another method of intermittent hypoxia/hyperoxia training (IHHT) began to enter the clinical practice, when the periods of breathing with atmospheric air are replaced by breathing a hyperoxic mixture. The present study compared the impact of adaptation to IHHT versus IHT on some metabolic variables in prediabetic patients.
Methods:
A placebo-controlled trial included 55 patients with prediabetes, sea level residents, ages 51–74 years. Control Group (16 patients) took sham 3-week course, and the IHHT Group (17 patients) and IHT Group (22 patients) received similar actual sessions of IHHT or IHT five times a week for 3 weeks, each session consisting four cycles of 5 minutes of hypoxia (12% O2) followed by 3 minutes of hyperoxia (IHHT, 33% O2) or 5 minutes of normoxia (IHT, breathing room air). Fasting glucose, oral glucose tolerance test (OGTT), blood lipids, and the level of blood oxygen saturation (SpO2) were investigated at baseline, as well as 1 day and 1 month after IHHT/IHT termination.
Results:
The study showed the same positive effect of two types of training: equal reduction of serum glucose concentrations, both fasting and 2 hours of OGTT; decreased total blood cholesterol and low-density lipoproteins; and an equally smaller drop in SpO2 during acute hypoxic test (breathing with 12% O2 for 20 minutes). Improved parameters persisted 1 month after training termination in both groups.
Conclusion:
One of the advantages of IHHT over IHT observed in this study could be some reduction in the duration of the sessions due to shortening reoxygenation periods. Further studies are required to search for additional beneficial effects of IHHT when using other training modes or other pathologies.
Introduction
Intermittent hypoxia refers to episodic exposure to reductions in O2 in the inspired air separated by periods of normoxia (Serebrovskaya and Xi, 2016). In general, the biological responses to intermittent hypoxia may be either adaptive or maladaptive, depending on the severity, frequency, and duration of hypoxemia. The mechanisms of maladaptive responses to intermittent hypoxia, mostly associated with obstructive sleep apnea, were reviewed in several publications (Prabhakar and Semenza, 2012; Dempsey and Morgan, 2015; Mateika et al., 2015; Beaudin et al., 2017). On the contrary, the use of the so-called intermittent hypoxia/normoxia training (IHT), both in athletic practices and for clinical applications, has gained increasing attention and interests during the past few decades. Several reviews analyze the present scientific literature on this topic (Astorino et al., 2015; Mateika and Komnenov, 2017; Mallet et al., 2018; Neuhoff et al., 2018).
One of the key triggering mechanisms for adaptive responses to intermittent hypoxia is the induction of reactive oxygen species (ROS), which are involved in cell signaling, be it during cell growth or tissue repair. Moreover, exposure to ROS induces expression of certain genes, the products of which promote defence against cellular stress (Sen and Packer, 1996; Debevec et al., 2017). The induction of ROS occurs in the initial period of reoxygenation—when switching the gas mixture from hypoxic to normoxic. This effect is associated with the increase in antioxidant capacity (enzymatic and nonenzymatic) both in animals and humans (Serebrovskaya et al., 1992; Kolesnikova et al., 2003; Zepeda et al., 2013; Estrada et al., 2016; Heß et al., 2019). The main pathways in adaptive responses are considered to be reductive stress within the mitochondria, augmented catecholamine production, decreased mitochondria redox potential, and xanthine oxidase pathway activation (Lukyanova et al., 2009; Lukyanova and Kirova, 2011; Sazontova et al., 2012). Oxidative stress response depends on both the intensity and the duration of hypoxic/normoxic bouts. Short exposures to mild hypoxic episodes can afford protection to specific cells, tissues, or organs against more severe hypoxia and ischemia (Debevec and Millet, 2014; Debevec et al., 2015).
Several investigations suggest that mild hypoxic exposures provide a cost-effective strategy for improving metabolic function (see the reviews of Kayser and Verges, 2013; Mackenzie and Watt, 2016). In a mouse model of diet-induced obesity, intermittent hypoxic exposure reduced body mass, blood sugar, blood cholesterol, and liver fat cells, and increased serum leptin, insulin, and EPO concentrations (Qin et al., 2010). The glucose-lowering effect of IHT was also confirmed in patients with diabetes or prediabetes (Morishima et al., 2015; Camacho-Cardenosa et al., 2018; Costalat et al., 2018). In particular, it has been shown that short hypoxic impulses initiate an adaptive gene transcription program via hypoxia-induced factors (HIFs), in turn triggering several main target genes responsible for insulin reception and insulin secretion, facilitation of glucose transport, and regulation of glycolytic enzymes; in summary, these alterations optimize glucose uptake and normalize glycemia (Serebrovska et al., 2017, 2019). This point is particularly important for the elderly who are at greatest risk for developing type II diabetes.
The increasing interest in IHT has caused debate about the most beneficial regimens of hypoxic training. There are several articles devoted to analyzing the effects of various modes of IHT on the human organism (Navarrete-Opazo and Mitchell, 2014; Serebrovskaya and Xi, 2016; Chacaroun et al., 2017; Neuhoff et al., 2018). In the last decade, the method of intermittent hypoxic/hyperoxic training (IHHT) began to enter the clinical and sports practice. In IHHT, periods of breathing with atmospheric air are replaced by breathing with a hyperoxic mixture containing 30–40% oxygen (Bayer et al., 2017; Glazachev et al., 2017; Dudnik et al., 2018). According to some researchers, sequential delivery of hypoxic and hyperoxic (instead of normoxic) stimuli during IHHT allows to enhance the ROS-induced signal without increasing hypoxia. This leads to significant synthesis of protective intracellular protein molecules, mainly with antioxidant function (antioxidant protection enzymes, iron binding proteins, heat shock proteins) (Arkhipenko et al., 2005; Sazontova et al., 2008, 2016, 2017).
Recent studies examined IHHT's benefits in placebo-controlled clinical trials. Glazachev et al. (2017) investigated 46 patients with coronary artery disease (27 persons with real and 19 persons with sham hypoxic training program) and showed improved exercise capacity, reduced systolic and diastolic blood pressures, enhanced left ventricle ejection fraction, and reduced glycemia, but only at 1-month follow-up. Angina pectoris as a reason to stop exercising was significantly reduced after treatment and at 1-month follow-up. Dudnik et al. (2018) investigated how intermittent hypoxia/hyperoxia conditioning improves cardiorespiratory fitness in older comorbid cardiac patients and concluded that IHHT is safe in patients with cardiac conditions and common comorbidities. Bayer et al. (2017) investigated the cognitive performance in 34 patients, ages 64–92 years, in a placebo-controlled clinical trial and indicated significant improvements in a dementia-detection test and in physical endurance. Tuter and colleagues used IHHT for prevention of intra- and early postoperational complications in coronary bypass grafting (Tuter et al., 2018).
However, to the best of our knowledge, to date, no studies compared the effects of IHT and IHHT on similar patient groups. Thus, we explored whether hypoxic conditioning via IHT or IHHT may induce different physiological responses and whether one method may provide an advantage.
The purpose of the present study was to examine the potential differences in some metabolic parameters during the adaptation to IHT or IHHT in patients with prediabetes. We investigated the changes in blood glucose (fasting and after oral glucose challenge), blood lipid profile, and blood oxygen saturation (SpO2) before as well 1 day and 1 month after the 3-week course of hypoxic training.
Materials and Methods
Characteristics of participants
The clinical trial was conducted according to the laws of Ukraine and the principles of the Helsinki Declaration of Human Rights. The program of research, patient information, and informed consent forms were approved by the Ethics Committee of Chebotarev Institute of Gerontology, Kiev (protocol # 9, June 11, 2013).
Initially, 63 patients of both sexes with prediabetes, sea level residents, ages 51–74 years, who were observed at the Chebotarev Institute of Gerontology, have been involved in the research. Prediabetes was diagnosed in accordance with the criteria recommended by the expert committee on the diagnosis and classification of diabetes mellitus (Genuth et al., 2003), which include the following: (1) impaired fasting blood glucose level (from 5.6 to 6.9 mmol/L); (2) impaired glucose tolerance, that is, blood glucose level after 2 hours of standard glucose tolerance test (oral intake of 75 g glucose) was from 7.8 to 11.1 mmol/L; and (3) combined impairments with both elevated fasting blood glucose level and glucose intolerance defined above.
All subjects received detailed information of the study process, and a written informed consent was obtained from each of the participating subjects. All participants were nonsmokers and did not take any medication 2 weeks before and during the sessions of the study. They had no infections during the past month and no major cardiovascular or respiratory complications.
All participants were informed about the strict observance of lifestyle 1 month before, during, and 1 month after examination (including levels of physical activity, caloric content of daily diet, consumption of coffee and tea, and abstinence of alcohol). They followed the recommendations on diet ATP III [Diabetes Prevention Program (DPP) Research Group, 2002]. The daily caloric intake did not exceed 30 kcal/kg of body weight, and physical activity consisted in dosed daily walking for 40–50 minutes. All participants kept diaries in which they noted any lifestyle changes, if they occurred.
Selected patients were randomly (sealed envelope) allocated to control (Sham), IHHT, or IHT groups and started examinations. Eight patients did not complete the study due to personal reasons or nonobservance of lifestyle. As a result, 55 patients completed the planned study and were subsequently included in the analysis. The Sham Group consisted of 16 patients who underwent the course of IHHT placebo procedures, the IHHT Group consisted of 17 participants who underwent actual IHHT, and the IHT Group consisted of 22 patients who were trained with IHT.
Experiment protocols
All sessions of the present study were conducted in a quiet room at comfortable temperature within a clinical research center of the Chebotarev Institute of Gerontology. Measurement sessions were performed on two different days. On the first day, after a 3-day routine hospital diet (250–300 g carbohydrates) and normal physical activity, in the morning, after overnight fasting venous blood was drawn from the median antecubital vein of all three groups of patients to measure fasting glucose and blood lipids. Thereafter, the standard oral glucose tolerance test (OGTT) was conducted to identify prediabetic carbohydrate metabolism disorders according to Ryden et al. (2007). The test was performed using 75 g of glucose in 250 mL of water. Venous blood samples were drawn at 120 minutes after the oral glucose ingestion (2 hours post-OGTT). This procedure was repeated the next day and 1 month after the end of the sham/actual training course.
On the second day for the IHHT and IHT groups, the acute hypoxic test (AHT) was performed in the morning, after 2 hours of light breakfast to assess individual tolerance to hypoxia (Shatylo et al., 2016). It consisted of breathing a gas mixture with 12% O2 for 20 minutes. The baseline cardiorespiratory parameters were monitored for 5 minutes before AHT when participants sat in a comfortable chair and spontaneously breathed room air. Arterial oxygen saturation (SpO2) was recorded using Patient Monitor “UM 300-12” (“UTAS,” Ukraine). After that participants were connected to an open breathing circuit through a mask and breathed a standardized hypoxic gas mixture (12% O2 and 88% N2) for 20 minutes, and then were returned to room air breathing. AHT sessions were repeated 2 days and 1 month after the IHHT/IHT termination. The Control group did not undergo a hypoxic test to avoid any effects of hypoxia before the course of simulating IHHT.
From the next morning, after a light breakfast, all patients received IHT, IHHT, or sham training five times a week for the subsequent 3 weeks, for a total of 15 sessions. During the sessions, the subjects' SpO2 was continuously monitored and recorded. We applied hypoxic training regimens that are most commonly used in clinical studies: each session consisted of four cycles of 5 minutes of hypoxia (12% inspired O2) followed by 3 minutes of hyperoxia (IHHT, breathing with 33% O2 in nitrogen) or 5 minutes of normoxia (IHT, room air breathing). IHHT sessions were performed using the apparatus “CellAir One” (Cellgym Technologies GmbH, Germany). This instrument was also used for the imitation of IHHT sessions in Control group: sham subjects breathed through a mask during sessions but without switching to the supply of hypoxic gas mixture. For IHT sessions, the hypoxic apparatus—Hypotron® (Kiev Polytechnic Institute, National Technical University of Ukraine), was used.
Lipid, cholesterol, and blood glucose profiles
Fasting concentrations of serum total cholesterol, high- and low-density lipoprotein cholesterol (HDLC and LDLC), and triglycerides were determined using a Cholestech LDX device (Alere, San Diego, CA). Plasma glucose concentrations were analyzed by the glucose oxidase method on a semiautomatic biochemical analyzer BTS-330 using reagents “Glucose,” Bio LATEST Lachema Diagnostika.
Statistical analysis
All data were analyzed using SPSS software version 21.0 (SPSS, Inc.). Student t-test was used for comparing anthropometric characteristics of the participants between groups. For the assessment of SpO2 changes during one bout of first and last IHHT/IHT sessions, the paired-samples t-test was used. Two-way analysis of variance (ANOVA) with repeated measures followed by Bonferroni post hoc test was performed to determine Group Main Effect (sham vs. IHHT vs. IHT), Time Effect (for three time points: pre-IHT baseline, 1 day after IHHT/IHT, and 1 month after IHHT/IHT), and Group × Time interaction. Three-way analysis of variance (ANOVA) with repeated measures followed by Bonferroni post hoc test was used for the analysis of SpO2 during 20 minutes of AHT under the adaptation to IHHT or IHT at three time points. We determined Group Main Effect for two groups, which passed through AHT (IHHT vs. IHT), Time Effect (three time points: baseline, 1 day post, and 1 month post), Hypoxic Test Effect (responses to 20 minutes of AHT), and their interactions. The level of statistical significance was set at p < 0.05. All data are presented as mean values ± SD within the text, figures, and tables.
Results
In general, the entire process of medical examination and IHTT/IHT sessions was well tolerated by all subjects. No subjective discomforts and/or any other adverse effects were reported. The groups did not differ significantly in age, height, weight, body mass index (BMI), and waist circumference (Table 1).
Anthropometric Characteristics of the Participants (Baseline Measurement)
Data are presented as mean ± SD. Student t-test was used to evaluate the statistical significance of the differences between groups. No intergroup differences at p < 0.05.
BMI, body mass index; IHHT, intermittent hypoxia/hyperoxia training; IHT, intermittent hypoxia/normoxia training; WC, waist circumference.
Blood oxygen saturation
A level of SpO2 under hypoxic load is considered a main noninvasive parameter that characterizes hypoxic resistance. To illustrate similarities and diversities in IHHT and IHT methods, we present mean group SpO2 data at the first bouts of the 1st and 15th session (Fig. 1). During the first session (Fig. 1A), SpO2 slope was the same in both groups during hypoxic period, a similar level of SpO2 was reached by the end of the 5-minute hypoxic period. The main difference between the two methods becomes apparent during the period of reoxygenation: in IHHT Group, SpO2 recovered faster by the end of the second minute of hyperoxic breathing, while in the IHT Group, SpO2 recovered only by the end of the fifth minute of breathing room air. Three-week course of hypoxic training led to a significant and similar increase in SpO2 level at fifth minute of hypoxic bout and second and third minute of reoxigenation in both IHHT and IHT groups illustrating similar positive adaptive shifts (Fig. 1B).
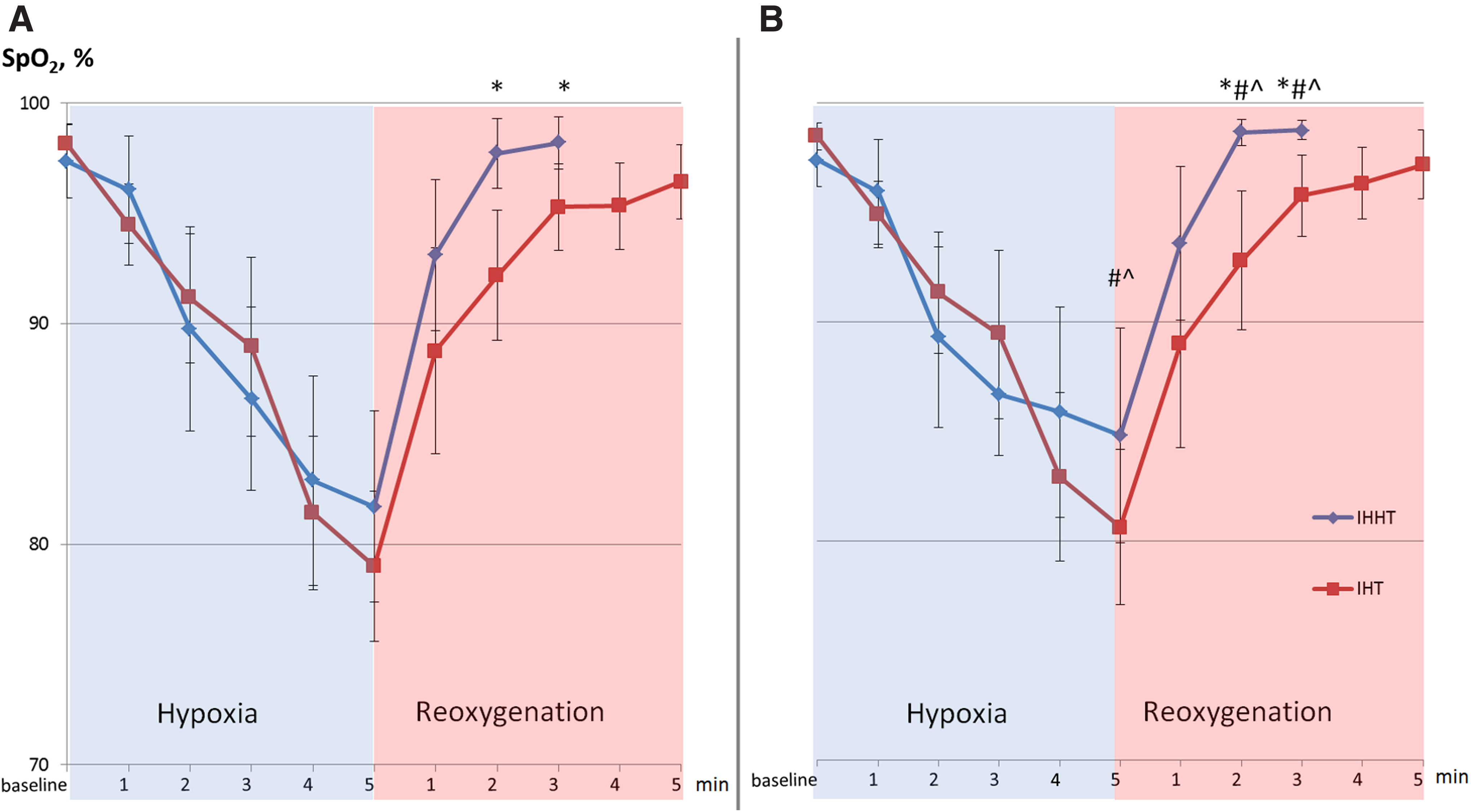
SpO2 during the first bout of the first
Figure 2 demonstrates changes in blood oxygen saturation during AHT under the adaptation to IHHT or IHT. Results indicate that at the 20th minute of breathing with 12% O2, SpO2 decreased equally in both groups reaching the values 79.4% ± 3.8% in IHHT Group and 80.3% ± 2.4% in IHT Group. After 15 sessions of IHTT/IHT, this drop was less than before training (81.5% ± 3.9% and 83.2% ± 2.5%, respectively). The elevated level of SpO2 during AHT was also maintained a month after the end of training in both groups. Three-way ANOVA confirmed the significance of changes in blood oxygen saturation during AHT at three measurement points (Time Effect: p < 0.01; Hypoxic Test Effect: p < 0.01, and Time × Hypoxic Test Effect: p = 0.002) and insignificance of differences between groups (Group Main Effect, Group × Time Effect, and Group × Hypoxic Test × Time Effect).

Time-dependent effects of IHHT or IHT training on blood oxygen saturation during AHT in patients with prediabetes. Data are mean ± SD and were analyzed with three-way ANOVA with repeated measures followed by Bonferroni post hoc test (the statistic results are represented in table). *p < 0.05 toward baseline (Bonferroni post hoc test). AHT, acute hypoxic test; ANOVA, analysis of variance.
Blood glucose levels
Table 2 demonstrates the effects of sham training, IHHT, or IHT on blood glucose in prediabetic patients. Before hypoxic training, the fasting glucose level was the same in all three groups and within the range specific to prediabetic conditions. After a 3-week hypoxic course, fasting glucose did not change in the Sham group and decreased significantly in both groups with actual hypoxic training. The reduced level of glycemia was maintained 1 month after IHHT/IHT termination (by 16% and 20%, respectively). The Bonferroni post hoc test showed significant differences in glycemia in IHHT/IHT groups compared with baseline and with the Sham group, and the absence of differences between IHHT and IHT groups (p > 0.05). Positive effect of the two types of hypoxic training is confirmed by the two-way ANOVA: Group Main Effect, Time Effect (three time points), and Group × Time interaction were statistically significant. Taken together, based on ANOVA indices, a positive effect was observed in both treatment groups when compared with the Sham-treated group, while no differences were observed when the two treatment groups were compared.
Glucose Blood Serum Concentration Before and After the 3-Week Sessions of Sham, Intermittent Hypoxia/Hyperoxia Training, or Intermittent Hypoxia/Normoxia Training
Data are mean ± SD and were analyzed with two-way ANOVA with repeated measures.
p < 0.05 versus pre-IHHT/IHT baseline (via Bonferroni post hoc test).
p < 0.05 IHHT/IHT versus Sham (via Bonferroni post hoc test).
ANOVA, analysis of variance; OGTT, oral glucose tolerance test.
The glucose tolerance test showed that before hypoxic training, the 2-hour post-OGTT glucose level was within the range specific to prediabetic conditions in all groups. After the 3-week course of sham/actual hypoxic training, the 2-hour post-OGTT did not changed in the Sham group and decreased equally in IHHT and IHT groups (by 16% and 15%). One month after the termination of training, the level of 2-hour post-OGTT decreased even more in these groups than just after the 3-week course (by 21% and 23%, respectively), and at this time point, no significant difference between IHHT and IHT was observed according to the Bonferroni post hoc test. Two-way ANOVA indicates a significant change in 2-hour post-OGTT level depending on the hypoxic training (Time Effect was statistically significant: p < 0.01, Table 2).
Blood lipid levels
Before hypoxic training, the level of the main blood lipids corresponded to the standards for prediabetes development and did not differ in all groups (Table 3). Intermittent hypoxic training led to a significant decrease in total cholesterol in IHHT and IHT groups (by 9% and 13%, respectively), but in a month, this positive effect was almost not preserved. Meanwhile, Time Effect (three time points) was significant. No differences were observed in Sham group according to the Bonferroni post hoc test.
Blood Lipid Levels Before and After the 3-Week Sessions of Sham, Intermittent Hypoxia/Hyperoxia Training, or Intermittent Hypoxia/Normoxia Training
Data are mean ± SD and were analyzed with two-way ANOVA with repeated measures.
p < 0.05 versus pre-IHHT/IHT baseline (via Bonferroni post hoc test).
p < 0.05 IHHT/IHT versus Sham (via Bonferroni post hoc test).
HDLC, serum high-density lipoprotein cholesterol; LDLC, serum low-density lipoprotein cholesterol; TC, serum total cholesterol; TG, serum triglycerides.
Training did not change significantly HDLC in all groups. However, hypoxic training significantly and equally reduced the level of LDLC in IHHT and IHT groups (by 17%). A low level of LDLC remained for a month after the end of training in these groups. No significant effect was observed in the Sham group (according to Bonferroni post hoc test). Two-way ANOVA confirmed the significance of positive hypoxic influences on LDLC (Time Effect: p < 0.01). Neither IHT nor IHHT affected serum triglyceride concentrations.
Discussion
During the last decade, various protocols of intermittent hypoxic training/treatment have rapidly entered medical practice, sports, and other areas of human activity. The diversity of protocols hampers comparison of results, and may lead to divergent conclusions regarding the effects of hypoxytherapy. More and more questions appear in the literature: “How much IHT is too much,” “how long does IHT protection last” (Sprick et al., 2019), “what are the effective modes for different pathologies,” “how to standardize protocols” (Navarrete-Opazo and Mitchell, 2014; Mateika et al., 2015), and so on.
The present study was devoted to a detailed comparison of two types of hypoxic training, namely hypoxic/normoxic and hypoxic/hyperoxic intermittent training, on glucose and lipid metabolism, as well as on some cardiovascular reactions to AHT in patients with prediabetes. We investigated two similar groups of patients and used two similar programs of hypoxic training, differing only in the reoxygenation periods: 3-minute inhalation of 36% O2 (IHHT) or 5-minute breathing of room air (20.9% O2) (IHT). In addition, a Control group that received sham training in the same mode as the IHHT group was investigated.
Our comparative study showed the same positive effect of the two types of actual training, namely: (1) equally reduced fasting and 2-hour post-OGTT glucose levels that were maintained for at least 1 month after the end of the training; (2) decreased blood total cholesterol in both groups after a 3-week training course, with no significant difference between the groups; (3) equally reduced levels of LDLC that were kept at this level for at least a month after the end of training; (4) equally raised level of SpO2 during a hypoxic test, which was maintained until 1 month after training in both groups. The sham hypoxic training of the Control group did not lead to significant shifts in the studied parameters. Given that the degree of improvement was the same in both groups with actual hypoxic training, it can be argued that one of the advantages of using IHHT over IHT in this training regimen and this pathology could be some reduction in the duration of sessions due to shortening the reoxygenation periods.
The idea of enhancing the positive effect of hypoxic training by replacing normoxia with hyperoxia during recovery periods was expressed quite long ago (Arkhipenko et al., 2005). It was shown on animals that hypoxia/hyperoxia adaptation resulted in a membrane-stabilizing effect in the heart, brain, and liver, which was more pronounced than after hypoxia/normoxia training. In contrast to hypoxia/normoxia, hypoxia/hyperoxic training resulted in a quicker adaptive response. Other authors (Gonchar and Mankovska, 2012) confirmed that moderate hypoxia/hyperoxia (five cycles of 5 minutes of hypoxia with 10% O2 and 5 minutes of hyperoxia with 30% O2, daily for 2 weeks) attenuated acute hypoxia-induced oxidative damage and improved antioxidant defense in lung mitochondria of rats. The authors concluded that mitochondrial protection during hypoxia/hyperoxia may be mediated through the modulation of mitochondrial antioxidant levels. More recent animal studies have shown that the adaptation to interval hypoxia/hyperoxia prevented disturbances caused by administration of low doses of toxicants and corrected, for example, abnormalities provoked by long-term alcohol consumption (Sazontova et al., 2016, 2017). These effects were accompanied by a suppression of free radical oxidation, a decrease in the levels of HIF-1α and inducible HOx-1, and improved tolerance to physical exercises.
In recent years, several publications described the effects of IHHT on humans. Glazachev et al. (2017) investigated the effects of repeated exposures (three sessions a week for 5 weeks) to hypoxia (5 minutes of 10%–12% O2) and hyperoxia (3 minutes of 30%–35% O2) in coronary artery disease patients: they found that such a regimen improved exercise tolerance, cardiometabolic profile, and quality of life. Syrkin et al. (2017) used the hypoxic/hyperoxic training method to treat patients with ischemic heart disease. IHHT was associated with significant improvement of exercise tolerance, subjective perception of quality of life, as well as a reduction in the number of angina attacks.
The effectiveness of hypoxic/hyperoxic training was also investigated on athletes with overtraining syndrome. Sazontova et al. (2012) have shown that 14 sessions of IHHT led to the normalization of autonomic balance, increased resistance to acute hypoxia in hypoxic test, and increased physical performance. Similar studies were conducted later (Susta et al., 2017): 15 athletes with overtraining syndrome undertook a conditioning program consisting of repeated exposures to hypoxia (O2 at 10%) and hyperoxia (O2 at 30%), six to eight cycles, three times a week, applied 2 hours after a low-intensity exercise session over 4 weeks. The combination improved exercise performance and sympatho-parasympathetic index.
The data obtained in this study are in line with previous studies on prediabetic patients using hypoxic/normoxic training (Serebrovska et al., 2017), as well as with the research of other authors that showed the glucose-lowering effect of IHT (Morishima et al., 2015; Camacho-Cardenosa et al., 2018; Costalat et al., 2018). However, to the best of our knowledge, no comparison of IHHT efficacy with other hypoxic training regimens has been reported so far.
The mechanisms underlying the beneficial effects of intermittent hypoxia in one or another mode are still rather vague, although they were investigated at the multiple biological levels, from systemic physiological reactions to genomic regulation (Xi and Serebrovskaya, 2012; Navarrete-Opazo and Mitchell, 2014; Mateika et al., 2015; Dempsey and Morgan, 2015; and Costalat et al., 2018). Here we should mention that beneficial versus pathogenic outcomes of IHT/IHHT are strongly associated with features of the respective protocol, including the level of hypoxemia within episodes and the duration and number of episodes per day (Navarrete-Opazo and Mitchell, 2014; Serebrovskaya and Xi, 2016).
According to literature data, while formation of adaptive signs occurs in the hypoxic period, the irritating effect of short hypoxic “pricks” may result in reorganization of mitochondrial energy metabolism aimed at more economical operation of the Krebs cycle during both normoxia and hypoxia (Kurhaliuk et al., 2002; Lukyanova and Kirova, 2015, Lukyanova et al., 2018). Moderate levels of intermittent hypoxia induce gene expression profiles that result in the activation of complex intracellular signaling cascades, which finally result in the induction of hypoxic tolerance. Our previous research has shown that IHT upregulates HIF-1α mRNA expression in healthy subjects and prediabetic patients, as well as several HIF-1α-regulated genes in blood leukocytes, such as energy-independent facilitative glucose transporter-1 (GLUT-1), insulin receptor (INSR), ATP-sensitive potassium channels (KCNJ8), and pyruvate dehydrogenase kinase 1 (PDK-1) that are most important for regulating glucose metabolism through the activation of glucose transport into the brain, upregulation of insulin secretion in the b-cells of pancreas, and so on (Serebrovska et al., 2017, 2019).
One of the important mechanisms responsible for adaptive responses to intermittent hypoxia is the induction of ROS (Arkhipenko et al., 2005; Sazontova et al., 2008). To our regret, we did not evaluate free radical production and the antioxidant defense capacity in our patients. However, our measurements of simple biochemical and physiological parameters that, meanwhile, are decisive for diabetic disorders have shown that the two chosen regimens of IHT and IHHT cause the same positive changes in carbohydrate and lipid metabolism, as well as an equal increase in tolerance to acute hypoxia. In our opinion, one of the advantages of IHHT over IHT in this training regimen is the possibility of shortening training sessions due to the reduced duration of the reoxygenation periods. Perhaps other modes of hypoxic regimens and other types of pathology may reveal novel advantages/disadvantages of the hypoxic/hyperoxic training method.
A major limitation of the present study is that we could not provide a fully blinded protocol as the investigator needed to know whether to set up the hypoxicator for sham or actual hypoxic training. However, patients did not know whether they had actual or sham hypoxic exposures. Another limitation is the small sample size and unequal number of patients in all groups due to uneven dropout. This limitation resulted mainly from our difficulty to recruit highly cooperative subjects for the entire long-term studies. However, given the clarity of the data obtained, it does not seem likely that a larger sample size would produce different results. Anyway, the reported findings should be regarded as preliminary and they need further evaluation in larger cohorts.
Moreover, we were able to examine patients only after 3 weeks of IHHT/IHT. However, it is possible that IHHT could establish its effects more rapidly, such that 1 or 2 weeks of training may shorten the overall training period.
Conclusions
Our comparative study provided novel evidence showing that 3 weeks of the IHHT and the intermittent hypoxic/normoxic training in the selected mode (four bouts of 5 minutes of 12% O2 and 3 or 5 minutes of reoxygenation, respectively) can trigger similar beneficial effects in lowering fasting and post-OGTT blood glucose levels, decreasing the total cholesterol and level of low-density lipoproteins, as well as improving blood oxygen saturation during hypoxic periods in prediabetes patients. These positive effects persisted for at least 1 month after the termination of the procedures. One of the advantages of IHHT over IHT seen in this study may be a reduction in the time of treatment session due to shortening of reoxygenation periods. Further studies are required to search for additional beneficial effects of hypoxic/hyperoxic intermittent hypoxia training/treatment, in particular when using other training modes or other pathologies.
Footnotes
Acknowledgments
The authors are grateful to Dr. Svitlana Naskalova and nurse Irina Partola for the technical assistance in conducting this study.
Authors' Contributions
All authors participated in the design and interpretation of the studies, data analysis, review, and final approval of the article. T.V.S. designed the study and wrote the article. T.V.S. and V.B.S. elaborated the study protocols. O.N.G., V.I.P., E.E., Z.O.S., E.E., and V.B.S. conducted physiological investigations and performed statistical analyses of the results. V.B.S. provided the enrollment and clinical examination of the subjects as well as general research management.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partly supported by the National Academy of Medical Sciences of Ukraine, Ukrainian National Academy of Sciences, and German company Cellgym Technologies GmbH, and by the Ukrainian State Budget Program “Support for the Development of Priority Areas of Scientific Research” (Code: 6541230).