
Abstract
Introduction:
Tolerance to high altitude in women might be influenced by hormonal status since female hormones modulate ventilation.
Methods:
Our objectives were (i) to explore in 1060 women, the influence of the phase of menstrual cycle, oral contraception, and menopause with or without hormonal treatment, on hypoxic ventilatory response at exercise (HVRe) and hypoxic cardiac response at exercise (HCRe) measured during a routine hypoxia exercise test, before an exposure to high altitude; (ii) to determine in 260 women exposed to high altitude, the influence of menopause and oral contraceptive and other drug use, on the prevalence of severe acute mountain sickness (sAMS). Four groups were defined: premenopausal with or without oral contraception and postmenopausal with or without hormonal treatment.
Results:
In premenopausal women without contraception, HVRe was higher in the early luteal/midluteal phase than in the early follicular phase (0.89 ± 0.37 vs. 0.75 ± 0.27 mL/[min · kg], p = 0.03). HVRe was similar in postmenopausal versus premenopausal women. HCRe was lower in postmenopausal women (p < 0.001), due to aging. HVRe decreased from second to fourth decade of age and increased from fourth to eighth decade, while HCRe consistently decreased with aging. Oral contraception or hormonal treatment had no effect on responses to hypoxia. The prevalence of sAMS was similar in all groups. Severe high-altitude illness score was higher and HVRe lower in women with sAMS.
Conclusion:
(i) physiological responses to hypoxic exercise depend on the ovarian cycle phase and menopause status, (ii) oral contraception and hormonal treatment have no influence on the tolerance to high altitude, and (iii) independent of hormonal status, aging modulates physiological responses to hypoxia.
Introduction
Hypoxic ventilatory response at exercise (HVRe) is a determinant factor of tolerance to high altitude (Richalet et al., 2012; Canouï-Poitrine et al., 2014). In women, female hormones are known to modulate ventilation (Behan and Wenninger, 2008). Therefore, tolerance to high altitude might be influenced by female hormonal status. Considering the great changes in hormonal status during the menstrual cycle, we can speculate that HVRe might vary along the phases of the menstrual cycle. However, conflicting results are found in the literature, mainly because of low number of studied subjects and high variability in hormonal changes during the ovarian cycle; moreover, hypoxic ventilatory response (HVR) was mainly measured at rest and not in exercising conditions (Schoene et al., 1981; Takano, 1984; Dombovy et al., 1987; Regensteiner et al., 1990; Muza et al., 2001).
Menopause (in untrained women) has been shown to blunt the age-related increase in HVR observed in males (Lhuissier et al., 2012). Chronic mountain sickness, the pathophysiology of which is mainly determined by hypoventilation and hypoxemia, is mainly observed in men and postmenopausal women (León-Velarde et al., 2001), suggesting a role of hormonal modulation of HVR. Hormonal treatments are frequently used by women, either for contraceptive purposes or to mitigate the effects of menopause. Hormone replacement has been shown to increase HVR in postmenopausal women (Cistulli et al., 1994). However, little is known about the influence of the cycle phase, menopause, or the use of female hormone treatment on HVR and tolerance to high altitude.
Altogether, very few studies were performed about women's physiological responses to acute or chronic hypoxia until the end of the 1990's when there appeared a regain of interest as witnessed by the 1997 Hypoxia Symposium in Lake Louise where “Women at altitude” was the leading theme (Moore, 1997). Thereafter, some publications were dedicated to women's physiology and especially to the influence of the ovarian cycle on the physiological responses to hypoxia (Beidleman et al., 1999; Muza et al., 2001).
The objectives of this study were to explore in a large cohort of women the influence on HVRe and hypoxic cardiac response at exercise (HCRe) responses to hypoxia at exercise of (i) the phase of menstrual cycle, (ii) oral contraception, and (iii) menopause with or without hormonal treatment. Moreover, our study aimed to evaluate the tolerance to high altitude as evaluated by the incidence of severe acute mountain sickness (sAMS), as a function of age, hormonal status, and treatments, taking into account other drugs that are frequently used during trekking and that may interfere with the incidence of AMS.
For this purpose, we took advantage of the large cohort of subjects coming to our high-altitude medical consultation for exercise HVR testing before a stay at high altitude (Richalet et al., 2012; Canouï-Poitrine et al., 2014; Richalet et al., 2015).
Subjects and Methods
Subjects
From 2009 to 2017, 1060 sea level female natives went through a routine hypoxia exercise test at an outpatient mountain medicine consultation before a sojourn at high altitude. Subjects were included when they planned to spend at least 3 days above 4000 m with one night above 3500 m. Before the inclusion in the testing process, each patient was informed and signed consent documents. After clinical assessment, subjects were asked the number of days from the first day of their last menstruation to determine the phase of their cycle on the day of the test. They were also asked if they took oral contraception and if they were postmenopausal. No hormonal measurement was made at the occasion of this particular consultation, although most of the postmenopausal women had a regular evaluation of their hormonal status by their general practitioner or gynecologist.
Four groups of women were then defined: group A (n = 336), premenopausal without oral contraception; group B (n = 169), premenopausal with oral contraception; group C (n = 428), postmenopausal without hormonal treatment; and group D (n = 69), postmenopausal with hormonal treatment. Within group A, four periods were defined following the first day of previous menstruations: 0–4 days, 5–14 days, 15–24 days, and 25–28 days (Fig. 1). No difference was made between the type or dose of oral contraception, neither between the type or dose of hormonal treatment for postmenopausal women. A control group of 226 male subjects was extracted from our cohort of patients coming to the mountain medicine consultation (Canouï-Poitrine et al., 2014), with identical mean age of the present female cohort, to compare physiological variables and clinical outcome at high altitude.
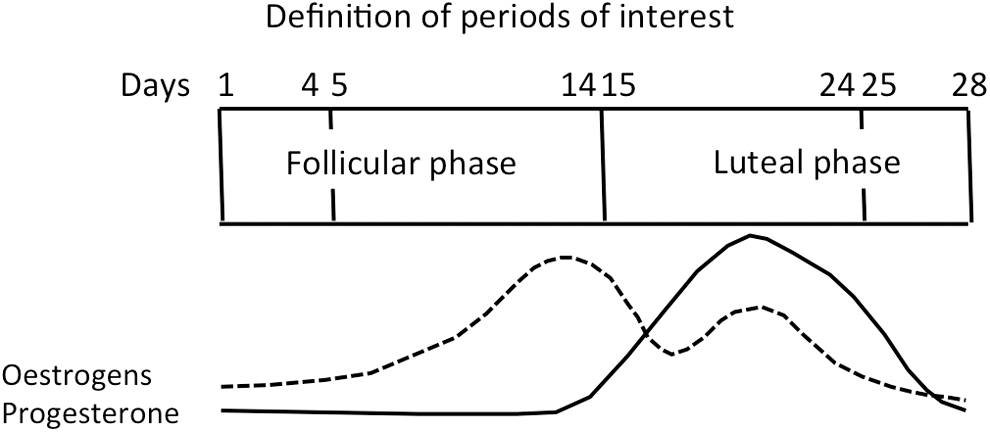
Determination of periods of interest during the follicular and luteal phases. Typical schematic variations of estrogens and progesterone are indicated.
Methods
Laboratory testing
As explained in previous studies (Richalet et al., 2012; Canouï-Poitrine et al., 2014; Richalet et al., 2015), subjects performed an exercise test consisting of five successive phases: 1—rest in normoxia, 2—rest in hypoxia (fraction of inspired oxygen 0.115 equivalent to 4800 m altitude), 3—exercise in hypoxia (EH) at 30% of maximal normoxic power output, 4—exercise in normoxia (EN) with the same power output as in EH, and 5—EN with the same heart rate (HR) achieved during EH (EN+). The power output used during the EH and the EN phases was fixed to ∼30% of maximal aerobic power, which corresponds to 40%–50% of HR reserve based on the value of theoretical maximal HR (220-age). Room air temperature was maintained at 22°C. The exercise was performed on an electrically braked cycloergometer (ER 900; Jaeger, Wuerzburg, Germany).
Minute ventilation (
Clinical evaluation at high altitude
During their sojourn at high altitude, subjects were asked to fill out a daily questionnaire about their medication use (especially acetazolamide [ACZ], aspirin, paracetamol, and ibuprofen), daily level and gain in altitude, sleep altitude, activities, cardiovascular or respiratory complains, symptoms of acute mountain sickness (AMS) based on the Lake Louise Score, high altitude pulmonary edema (HAPE) (clinical signs of respiratory distress [dyspnea, cyanosis, and rales] later confirmed by a thorax X-ray), and high altitude cerebral edema (HACE) (clinical signs of neurological deficit: ataxia and mental confusion). The Lake Louise Score (LLS) is a self-administered questionnaire based on the most frequent symptoms of AMS: headache, gastrointestinal symptoms (anorexia, nausea, or vomiting), weakness and/or fatigue, dizziness/light-headedness, and sleeping difficulty (Lake Louise, 1992). Given that no subject suffered from HAPE and HACE, we restricted the analysis to sAMS to deal with a homogeneous group of patients. Subjects with sAMS as defined by the LLS questionnaire (headache and LLS ≥6) were included in the sAMS+ group. The presence of peripheral edema (two locations) was also self-evaluated and reported in the questionnaire.
A large proportion of subjects (44%) took preventive ACZ during their sojourn since this prescription takes part of our decisional tree in case of high SHAI probability (SHAI score >5) (Canouï-Poitrine et al., 2014; Richalet et al., 2015). However, in this study, no difference was found in the prevalence of sAMS between the groups who did or did not take ACZ (26.8% vs. 26.1%, nonsignificant [ns]) so that groups were pooled for further analysis.
Statistical analysis
We compared physiological variables between A, B, C, and D groups by a two-factor analysis of variance (ANOVA) (premenopause/postmenopause and treatment/no treatment). Similarly, the influence of age category on physiological variables was assessed by a one-way ANOVA, pooling all groups. When appropriate, we compared groups two-by-two, using Student t-tests for quantitative variables and Pearson's χ2 test or Fisher's exact test (when <5 subjects in any condition) for qualitative variables. A multiple regression was performed to assess the respective influence of age, menopause, and treatment on the variables of interest.
The differences were considered statistically significant when p < 0.05 or ns if p > 0.05. Quantitative variables were reported as mean ± standard deviation and qualitative variables as n (%). Statistical analysis was performed by using STATA software version 14 (Stata, Inc., College Station, TX).
Results
Information obtained at sea level during the hypoxia exercise test
Oxygen saturation in hypoxia at exercise (SaO2e) and HVRe as a function of the phase in the menstrual cycle in premenopausal women not taking contraceptives are shown in Figure 2. Both SaO2e and HVRe were maximal during the early luteal/midluteal phase (15–24 days after the first day of menstruations). No difference was found in HCRe with cycle phase (data not shown). Maximal values of SaO2e and HVRe at the early luteal/midluteal phase were similar to the values of the control male group, matched for age. In all female groups pooled, HVRe and HCRe as a function of age categories are shown in Figure 3. There was no overall effect of age on HVRe (ANOVA, p > 0.05). However, taking the 40s (40–49 years) decade as the reference period, HVRe slightly decreased from the 20s to the 40s and then increased from the 40s to the 70s. HCRe progressively declined with aging (ANOVA, p < 0.001), the difference (vs. <20 years) being significant from the sixties. Multiple regression (age/menopause/treatment) analysis showed that menopause had no effect on HVRe and that age was the principal determinant of HCRe decline between postmenopausal and premenopausal women (Table 1).
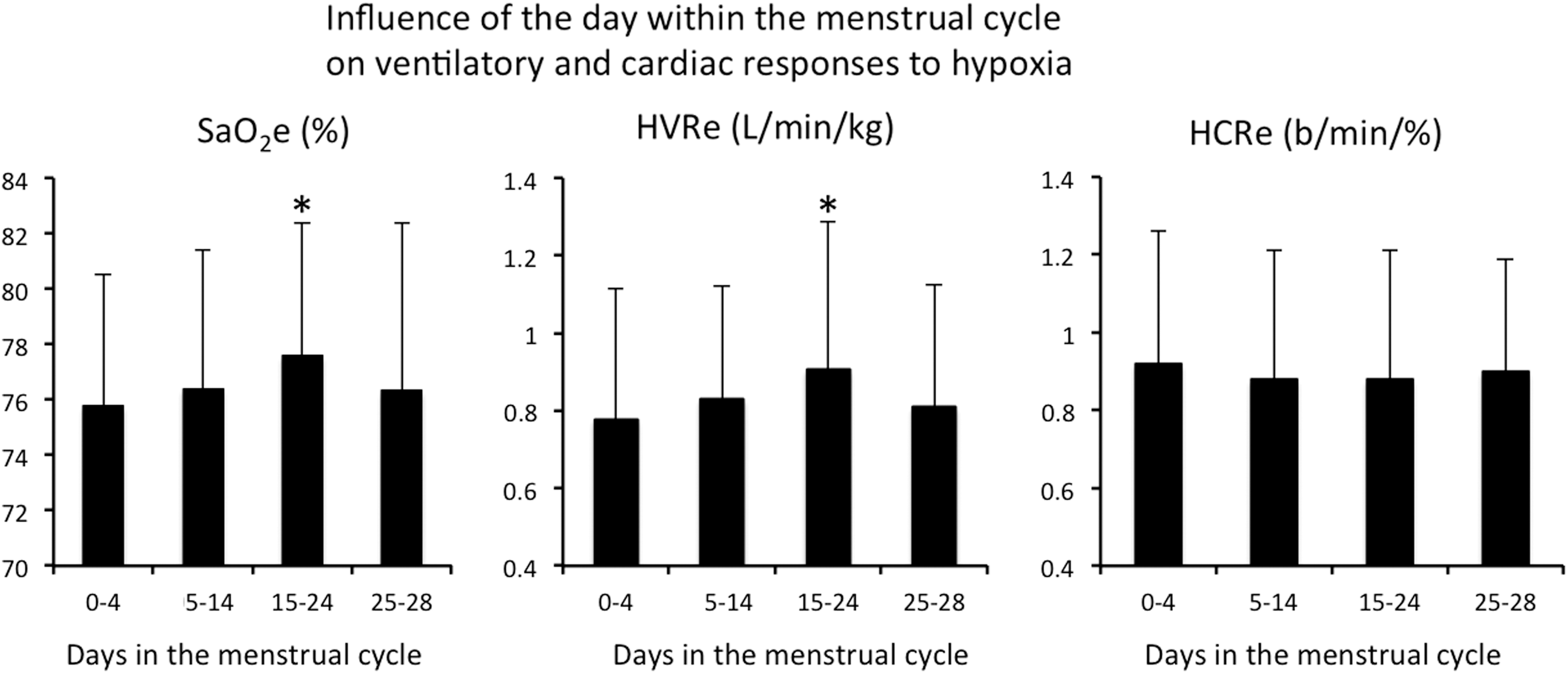
Influence of the day within the menstrual cycle on SaO2, HVRe and HCRe in premenopausal women, taking no contraception (group A). Values for an age-matched male group are given for comparison. *p < 0.05 period 15–24 versus period 0–4. HVRe, hypoxic ventilatory response at exercise; HCRe, hypoxic cardiac response at exercise.
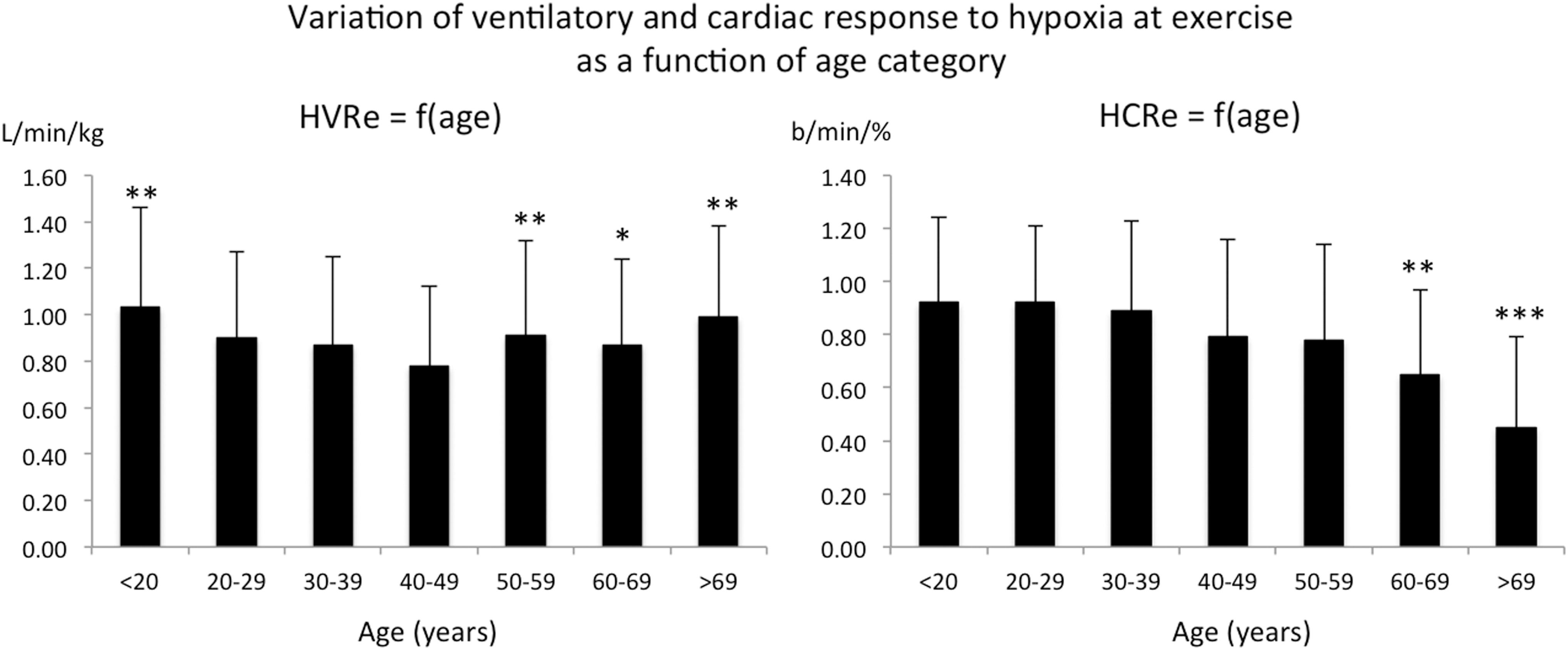
Variation of ventilatory (HVRe) and cardiac (HCRe) responses to hypoxia as a function of age category. All groups A, B, C, and D are pooled. For HVRe: *p < 0.05, **p < 0.01 versus 40–49 years. For HCRe: **p < 0.01, ***p < 0.001 versus <20 years.
Anthropometrics, Ventilatory, and Cardiac Responses to Hypoxia at Exercise as a Function of Menopause and Hormonal Treatment
p < 0.01, **p < 0.001 postmenopausal versus premenopausal.
HVRe, hypoxic ventilatory response at exercise; HCRe, hypoxic cardiac response at exercise; ns, nonsignificant.
Information obtained during the sojourn at high altitude
Data were obtained from 260 women. Table 2 shows in the various female groups and the control male group, the prevalence of sAMS, the maximal altitude reached, and the mean daily altitude gain. Women taking oral contraception were younger than those not taking. Prevalence of sAMS was similar in all female groups, but higher than in the male group. Peripheral edema was reported in 11.5% of all subjects, without any difference between groups, but almost double than in the male control group (6%). Postmenopausal women reached a lower maximal altitude during their sojourn than premenopausal ones, but the ratio altitude reached/altitude planned was similar. The daily altitude gain was similar between groups. Altitude planned and reached were higher in men, but the ratio was similar. Table 3 shows the medications taken during the sojourn at high altitude in the various groups. Women taking oral contraception more frequently took aspirin than the other groups. The use of ACZ, ibuprofen, and paracetamol was similar between groups.
Information Concerning the Sojourn at High Altitude in the Four Groups of Female Subjects and a Male Control Group
p < 0.001 with versus without treatment.
p < 0.05; ++p < 0.01; +++p < 0.001 premenopaused versus postmenopaused.
p < 0.001 total female groups versus male control group (χ2 or Student's t-test).
Information is lacking about phase cycle and contraception in 13 premenopaused women. Percentage altitude reached is the ratio (in %) Max altitude reached/Max altitude planned.
sAMS, severe acute mountain sickness; n.a., data not available.
Information Concerning the Treatments Used at High Altitude in the Four Groups of Subjects
No significant difference between groups, except for aspirin in premenopaused women, taking versus not taking contraceptives (*p < 0.05).
Information is lacking about phase cycle and contraception in 13 premenopaused women.
ACZ, acetazolamide.
Table 4 shows the values of HVRe, HCRe, and SHAI score in subjects who did not take ACZ, but did or did not suffer from sAMS. As expected, HVRe was lower and SHAI score was higher in those who suffered from sAMS.
Results of the Hypoxia Exercise Test Before the Exposure to High Altitude and Tolerance to High Altitude During the Sojourn
p < 0.05; ***p < 0.001 sAMS+ versus sAMS−. All subjects not taking acetazolamide.
SHAI, severe high-altitude illness.
Discussion
This is the first study exploring the ventilatory and cardiac responses to hypoxic exercise in a large cohort of women, with special attention to the influence of the phase of the ovarian cycle, menopause, and hormonal treatments. We confirmed that the oxygenation and the ventilatory adjustments were optimal in the early luteal/midluteal phase, where they were similar to male values. The difference observed between premenopausal and postmenopausal women was largely due to aging. Oral contraception and hormonal treatment had no effect on ventilatory or cardiac adjustments to hypoxia and on tolerance to high altitude.
The influence of the cycle phase on HVR at rest has been explored in a few studies and mostly in a small number of subjects. Ventilatory response to hypoxic exercise has been scarcely explored. HVR at rest and ventilation at exercise were found to be higher in the luteal phase than in the follicular phase in athletes (n = 6) and nonathlete (n = 6) females (Schoene et al., 1981). Similarly, ventilation was found higher in the luteal versus follicular phase in 14 physically active women and values of arterialized blood PCO2 were inversely related to plasma concentrations of progesterone and 17β estradiol during the luteal phase (Slatkovska et al., 2006). However, the last authors failed to find any difference in hyperoxic or hypoxic response to CO2 at rest between follicular and luteal phases.
In nine women performing a maximal exercise test at 3000 m, the ratio
In 22 women ascending to 4300 m, no significant difference was found in HVR at rest between luteal (n = 8) and follicular (n = 14) phases (Muza et al., 2001). Yet, when comparing the same subjects (n = 12) in both phases, a significant increase in ventilation was evidenced in the luteal phase. In a similar context, no difference was found in erythropoiesis (evaluated by erythropoietin concentration, reticulocyte count, and hematocrit) between follicular (n = 11) and luteal (n = 5) phases (Reeves et al., 2001). As the ventilatory response to CO2 interferes with the response to hypoxia at high altitude, it is interesting to note that an increase was found in the sensitivity to CO2 between the follicular and luteal phases in 20 females (Dutton et al., 1989). In women exposed for 12 hours to a simulated altitude of 4880 m, high levels of progesterone-progestin were associated with lower PaCO2 (higher ventilation), but the altitude-induced increase in ventilation was similar in men and women (Loeppky et al., 2001). In a study performed in a limited number of women (n = 10), but where the hormonal status was repeatedly measured, MacNutt et al. (2012) failed to find any difference in HVR at rest or exercise between follicular and luteal phases (although resting ventilation was higher in the midluteal phase), and this was probably linked to the great variability of the observed hormonal concentrations.
As a whole, there is quite a large variability in the literature as to whether or not the ovarian cycle phase might influence ventilatory responses to hypoxia/hypercapnia or exercise performance, probably because of the limited number of subjects included in all studies and the high variability of hormone levels (Schoene et al., 1981; Takano, 1984; Dombovy et al., 1987; Regensteiner et al., 1990; MacNutt et al., 2012).
The mechanism of hormonal influence on ventilatory adjustments is also controversial. Changes in gonadal hormones throughout the ovarian cycle coincide with changes in serotonin in respiratory motor nuclei, suggesting that the influence of the cycle phase on ventilatory adaptations may have a central origin (Behan et al., 2003). Conversely, ovariectomy in cats led to a decrease in carotid body response to hypoxia, but not in hypercapnic ventilatory sensitivity, suggesting that ovarian hormones mainly act on peripheral chemosensitivity (Tatsumi et al., 1997). The overall influence of sex hormones on the control of respiration is certainly complex since receptors for these hormones are found both in the periphery and in the brainstem centers (Behan and Wenninger, 2008).
Observations are scarce regarding the effects of hormonal treatment on HVR. When given medroxyprogesterone acetate, women showed an increase in HVR at exercise in the luteal phase (Regensteiner et al., 1990). In 14 women taking oral contraceptives, compared to male subjects, gender did not affect cortisol, growth hormone, or catecholamines during hypoxia or exercise (Sandoval and Matt, 2002). The use of oral contraceptives has been associated with an increased risk for the development of AMS in 17 women arriving abruptly at 3200 m (Harrison et al., 2013). Oral contraceptives have been shown to increase the risk of venous thrombosis, although the risk greatly depends on the type of contraceptive (Lidegaard et al., 2011). Some case reports have mentioned the association of oral contraceptive and venous thrombosis at high altitude, and high hematocrit has been considered a risk factor. However, no clear association has been established between oral contraceptive use and thrombosis at high altitude (Schreijer et al., 2010; Gupta and Ashraf, 2012; Keyes, 2015). In this study, no adverse effect of oral contraceptives was reported during the stay at high altitude. It is interesting to note that women taking oral contraceptive spontaneously more frequently took aspirin than those without contraceptive, although no control study has confirmed any advantage in counteracting the hypothetical risk of thrombosis.
Very few studies are available about the effect of menopause on sea level native women (Pokorski and Marczak, 2003; Lhuissier et al., 2012). Some studies were done in high-altitude natives. Low oxygen saturation in postmenopausal high-altitude native women was related to a high serum testosterone/estradiol ratio (Gonzales and Villena, 2000). In a study of Spanish-speaking women, those living in countries with higher temperatures and lower altitudes reported more frequent and problematic hot flushes (Hunter et al., 2013). In a study performed in 33 high-altitude women residing at Cerro de Pasco (Peru, 4300 m), there was a clear lower oxygenation and higher hematocrit in postmenopausal versus premenopausal women and arterial oxygen saturation was positively related to the levels of progesterone (León-Velarde et al., 2001). Similarly, the increase in progesterone level during the luteal phase was related to a significant increase in submaximal exercise ventilation in 23 HA native women (Brutsaert et al., 2002).
The slight increase in HVRe and clear decrease in HCRe observed in this study after menopause are entirely due to the effect of aging, as previously shown (Lhuissier et al., 2012; Richalet and Lhuissier, 2015). Both changes contribute to an unchanged SaO2 at exercise. HVRe has been suspected to increase with aging, due to the increasing prevalence of sleep hypopneas or apneas with aging that promote an increase in hypoxic chemosensitivity (Foster et al., 2005). This leads to a clear increase in HVR in men, although in women, this increase would be counteracted by the blunting of ventilation due to the decrease in female hormones, especially in untrained women (Lhuissier et al., 2012; Richalet and Lhuissier, 2015). Interestingly, another group found similar results for moderate exercise, but HVRe was higher in young subjects (20–30 years) than in older ones (60–70 years) at maximal exercise (Puthon et al., 2017). As previously shown at rest (Pokorski and Marczak, 2003), HVR at exercise in this study was similar in the youngest and the oldest women, but minimal in the 40s (Fig. 3). The decrease in HCRe with aging has been previously described (Lhuissier et al., 2012; Richalet and Lhuissier, 2015) and is probably related to the decrease in maximal HR and adrenergic responsiveness with aging (Christou and Seals, 2008).
Female gender has been found in large cohorts to contribute to the susceptibility to AMS (Richalet et al., 2012; Canouï-Poitrine et al., 2014), and this was confirmed in this study. However, severe forms necessitating evacuation have been found more frequent in men (Maggiorini et al., 1990) and higher scores of AMS were found in men compared to women in acute altitude exposure (Beidleman et al., 2013). However, no study is currently available in the scientific literature about the influence of ovarian cycle phase on AMS. It was not possible, in this study, to recover the information about the cycle phase and the period of exposure to high altitude. In fact, the time of the planned sojourn at high altitude was evidently determined independent of the cycle phase and with a probable overlap between follicular and luteal phases. Peripheral edema has been found more frequent in women (14%) than in men (4%) at high altitude (Canouï-Poitrine et al., 2014) and was again confirmed in this study where peripheral edema was twice more frequent in women (11.5%) than in men (6%). However, no study, including this one, has found an influence of menopause, hormonal treatment, or cycle phase on the prevalence of peripheral edema. Finally, this study confirms that the hypoxia exercise test, leading to the computing of the SHAI score, is a useful way to detect subjects susceptible to sAMS.
Some limitations in this study and in previous ones can account for the variable results between studies: the absence of hormonal analysis to confirm the cycle phase, the variety of methods used to evaluate HVR at rest or at exercise, the training status of the subjects that may interfere with the ventilatory and cardiac responses to hypoxia and the type and dosage of treatment that has been used. However, the large number of subjects included in this study may contribute to mitigate these confounding factors.
Recommendations for women going to high altitude are currently based more on basic physiological considerations or basic precautions than on controlled studies (Sandoval et al., 1997; Jean et al., 2005; Keyes, 2015; Jean, 2017). What is clearly shown from this study is that, in large cohort of women going to high altitude, no adverse effect on physiological adjustments to hypoxic exercise or altitude tolerance can be attributed to contraceptives or menopause hormonal treatment. Although it should be confirmed in large controlled epidemiological studies, women may take a small advantage of exercising at high altitude during their luteal phase, all other risk factors of sAMS being equal. The cycle phase is not probably a prominent factor, but it could help, knowing that progressive acclimatization is still the main advice to give to trekkers to avoid severe forms of AMS.
The fact that, in opposition to what others and ourselves have found in previous studies, the incidence of sAMS was not lower in the group taking ACZ is not so surprising. In fact, this study did not include a controlled double-blind study of the effect of ACZ on AMS. People were free to take any medication, especially ACZ, which is widely used as a preventive drug for AMS. Therefore, subjects at higher risk of sAMS (too rapid ascent, history of sAMS, low HVRe, and so on) will take ACZ and avoid sAMS, thus leveling down the incidence of sAMS in the high risk group. Finally, we observe what we would expect, as an MD: with good advice and prevention by ACZ, subjects with a potential higher risk show no major incidence of sAMS than the others, so that the incidence is the same in subjects taking or not taking ACZ.
Conclusions
Ventilatory response to hypoxic exercise depends on the ovarian cycle phase: SaO2e and HVRe are maximal during the early luteal/midluteal phase. Women taking oral contraception more frequently took aspirin than the other groups. Oral contraception, menopause, and hormonal treatment had no influence on responses to hypoxic exercise and tolerance to high altitude. HVRe in women depends on both the aging process and hormonal changes. HCRe decreases with aging, independent of hormonal status. SHAI score is confirmed as a good predictor of sAMS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.