
Abstract
The lactate threshold (LT) defines the exercise intensity at which lactic acid accumulates and rises exponentially in the blood (Wasserman, 1987). The LT limits a constant workload and correlates with exercise capacity (Faude et al., 2009). Exercise performance is reduced in high altitude, in particular before acclimatization (Burtscher et al., 2006). In patients with heart failure, the LT is dramatically reduced compared with healthy individuals and may be reached already at high altitude without any exercise due to pulmonary vasoconstriction and subsequent worsening of concomitant pulmonary hypertension (Bartsch and Gibbs, 2007).4 Interestingly, flying in a commercial airplane resembles exposure to moderate altitude (2000–2500 m) (Muhm et al., 2007) and may already be critical for some patients with heart failure. Whereas the decrease of exercise performance in acute high altitude has been well studied, evidence on LT is sparse (Burtscher et al., 2006). To elucidate the effect of acute moderate altitude or a flying in a commercial airplane on the LT, we determined the impact of acute altitude exposure without an acclimatization period before work performance on LT levels. For this purpose, we measured the LT at moderate altitude compared with conditions at 500 m in healthy individuals in a pilot study.
Fourteen healthy individuals (4 women and 10 men, mean age 35.6 years, range 24–56 years) were included in this study. All participants performed an exercise test on a cycle ergometer using a step protocol with a step change every 3 minutes. The workload was increased 20 W every 3 minutes starting at 40 W (women) or 60 W (men), respectively. Sampling of whole blood to measure lactate concentrations was conducted at the end of each step and before the exercise. Exercise tests were performed at the Environmental Research Station Schneefernhaus (UFS) at the Zugspitze (2650 m) within 1 hour after arrival and in Munich (521 m) to determine baseline conditions.
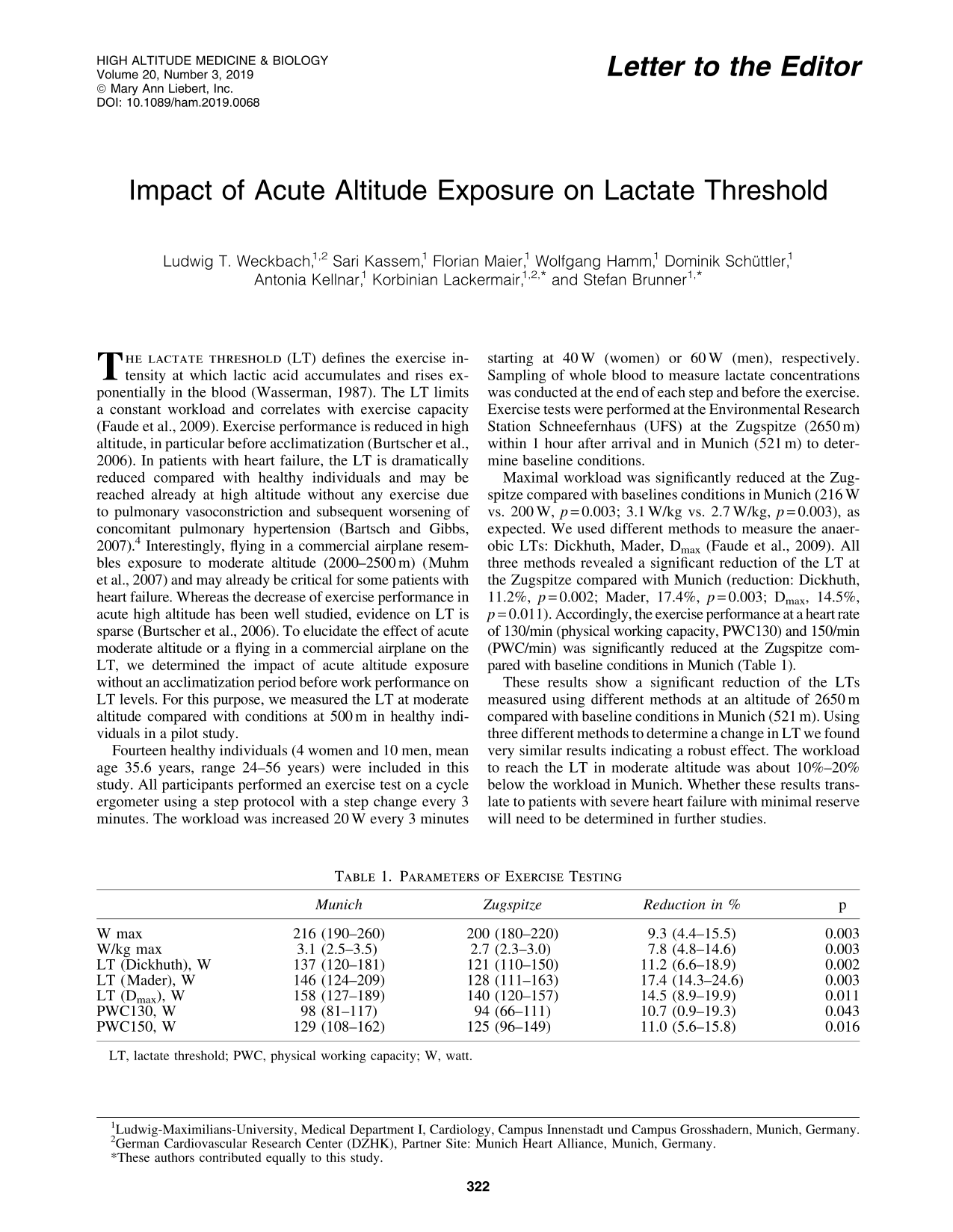
Maximal workload was significantly reduced at the Zugspitze compared with baselines conditions in Munich (216 W vs. 200 W, p = 0.003; 3.1 W/kg vs. 2.7 W/kg, p = 0.003), as expected. We used different methods to measure the anaerobic LTs: Dickhuth, Mader, Dmax (Faude et al., 2009). All three methods revealed a significant reduction of the LT at the Zugspitze compared with Munich (reduction: Dickhuth, 11.2%, p = 0.002; Mader, 17.4%, p = 0.003; Dmax, 14.5%, p = 0.011). Accordingly, the exercise performance at a heart rate of 130/min (physical working capacity, PWC130) and 150/min (PWC/min) was significantly reduced at the Zugspitze compared with baseline conditions in Munich (Table 1).
Parameters of Exercise Testing
LT, lactate threshold; PWC, physical working capacity; W, watt.
These results show a significant reduction of the LTs measured using different methods at an altitude of 2650 m compared with baseline conditions in Munich (521 m). Using three different methods to determine a change in LT we found very similar results indicating a robust effect. The workload to reach the LT in moderate altitude was about 10%–20% below the workload in Munich. Whether these results translate to patients with severe heart failure with minimal reserve will need to be determined in further studies.