
Abstract
Background:
It is well known that oxygen saturation as measured by pulse oximetry (SpO2) decreases as altitude increases. However, how SpO2 changes across childhood, and more specifically during sleep/wake states, at different high altitudes are less well understood. We aimed to perform a systematic review of all studies with direct SpO2 measurement in healthy children living at high altitude (>2500 meters above sea level) to address these questions.
Methods:
MEDLINE, EMBASE, and SciELO databases were searched up to December 2018. Two independent reviewers screened the literature and extracted relevant data.
Results:
Of 194 references, 20 studies met the eligibility criteria. Meta-analysis was not possible due to the use of different oximeters and/or protocols for data acquisition and reporting of different SpO2 central tendency and dispersion measures. The most relevant findings from the data were: (1) SpO2 is lower as altitude increases; (2) at high altitude, SpO2 improves with age through childhood; (3) SpO2 is lower during sleep and feeding in comparison to when awake, this SpO2 gap between wake and sleep states is more evident in the first months of life and narrows later in life; (4) SpO2 dispersion (interindividual variation) is higher at younger ages, and more so during sleep; (5) In 6/20 studies, the SpO2 values were nonnormally distributed with a consistent left skew.
Conclusions:
At high altitude, the mean/median SpO2 increases in children with aging; a significant gap between wake and sleep states is seen in the first months of life, which narrows as the infant gets older; SpO2 dispersion at high altitude is wider at younger ages; at high altitude, SpO2 shows a nonnormal distribution skewed to the left; this bias becomes more evident as altitude increases, at younger ages and during sleep.
Introduction
Since its description in 1975, oxygen saturation as measured by pulse oximetry (SpO2) (Severinghaus, 2007) has become a routine tool in clinical practice, to the point that it has been proposed as a new vital sign (Mower et al., 1997). SpO2 is a cheap, accessible, and portable tool used extensively in acute care, being especially important for acute respiratory infection categorization in infants and children (Lazzerini et al., 2015).
Around 140 million people worldwide live permanently at high altitude (Moore, 2001), where settlements are characterized by hypobaric hypoxia. No prior systematic review has considered normal reference data for resting daytime SpO2 levels across childhood at different high-altitude locations nor considered the impact of sleep and infant feeding on SpO2. Only through understanding normal variation can treatment thresholds be determined for acute infections such as pneumonia and bronchiolitis and chronic illness such as bronchopulmonary dysplasia, cystic fibrosis, and postinfectious bronchiolitis obliterans. Expected SpO2 characteristics during sleep at high altitude are also important to interpret polysomnographic findings (Hill et al., 2016b).
In the decade since Subhi et al. (2009) published a systematic review of normal SpO2 values in high-altitude resident healthy infants and children up to 12 years of age, oximeter technology has progressed. We aimed to extend and update this review to include pulse oximetry studies at high altitude across childhood, including teenagers, and taking in account the differences in wake, sleep, and feeding states, especially in infants.
Methods
We identified published studies from MEDLINE, EMBASE, and SciELO (up to December 2018) databases using the search terms: “(oxygen saturation) AND (high altitude)” restricted to child (birth to 19 years old) without language restriction; high altitude was defined as altitude >2500 meters above sea level (masl) (Moore, 2001). Studies published solely in abstract form were excluded because the methods and results could not be fully analyzed. In addition, we searched other nonbibliographic data sources such as web searching. Only studies of healthy individuals habitually living at high altitude were included. Exclusion criteria included: (1) studies limited to SpO2 measurement uniquely during the first 24 hours of life as SpO2 has important changes during this period (Gonzáles and Salirrosas, 2005); (2) data collected across a range of altitudes greater than ±50 m (e.g., between 3800 and 4200 masl), where it was not possible to identify the number of individuals located at a specific altitude; and (3) studies that included children with acute or chronic cardiorespiratory disorders, chronic ill health, or history of prematurity.
Data extraction and assessment of risk of bias
Titles, abstracts, and citations were independently reviewed by two authors (S.U. and C.M.G.). Based on the full-text versions, all the studies were evaluated, and after obtaining full reports, eligibility was assessed. Disagreements were discussed and resolved by consensus, and, when necessary, advice was sought from the third review author (J.A.C.-R.). The risk of bias was evaluated according to the Newcastle–Ottawa Scale (Wells et al., 2011). For methodological and reporting quality, a prespecified data analysis included year, country, altitude, type of study, number of participants, age range, SpO2 median/mean, and SpO2 dispersion measurements. The pulse oximetry device used and the duration of SpO2 recording were also searched. We also looked at whether hemoglobin (Hb) concentration measurements were reported.
Meta-analysis was not performed due to the variation between studies in oximeter devices, protocols, and the central tendency (e.g., mean/median) and dispersion measures (e.g., standard deviation, interquartile range, 5th/95th percentile) to report SpO2 values.
Using original source data from Rojas-Camayo et al.'s (2018) study, the SpO2 values from the first quartile were compared with those from the second to fourth quartiles grouped using RV 3.6.1 (July 2019 version) software. The comparison was made for three altitude levels (2500, 3600, and 5100 masl) and for two age groups (1–5 and 6–17 years old). Statistical differences were determined using the t-test when the Shapiro–Wilk test showed a p-value <0.05, otherwise the Mann–Whitney test was used.
Results
One hundred ninety-four studies were retrieved from the databases; of which, 20 were eligible for inclusion (Fig. 1). Most of the studies (n = 14) came from the South America Andean region (Peru = 4, Bolivia = 4, Colombia = 3, Ecuador = 2, Argentina = 1); three studies were from China, two from the United States, and one from Nepal. Seventeen studies reported SpO2 data during wakefulness (Lozano et al., 1992; Nicholas et al., 1993; Niermeyer et al., 1993, 1995; Gamponia et al., 1998; Torres et al., 1999; Beall, 2000; Huicho et al., 2001; Ramírez-Cardich et al., 2004; Alduncin et al., 2005; Mattos et al., 2005; Weitz and Garruto, 2007; Schult and Canelo-Aybar, 2011; Shrestha et al., 2012; Duenas-Meza et al., 2015; Hill et al., 2016a, 2016b; Rojas-Camayo et al., 2018). Ten studies reported SpO2 data during sleep (Niermeyer et al., 1993, 1995; Gamponia et al., 1998; Torres et al., 1999; Ramírez-Cardich et al., 2004; Duenas-Meza et al., 2015; Ucrós et al., 2015, 2017; Hill et al., 2016); four studies reported data in infants during feeding (Niermeyer et al., 1995; Gamponia et al., 1998; Torres et al., 1999; Ramírez-Cardich et al., 2004); and one study reported data when infants were crying (Gamponia et al., 1998). One study was published in a Colombian journal not identified by the search but was known by the authors (Torres et al., 1999). All studies were cross-sectional, except one, which had a longitudinal component (Duenas-Meza et al., 2015). The total number of SpO2 records sampled in these 20 studies was 6877 during wakefulness, 923 during sleep, and 528 in infants during feeding. The pulse oximetry device used and the sampling protocols were diverse (Table 1). The quality assessment of most studies was high with a low risk of bias.
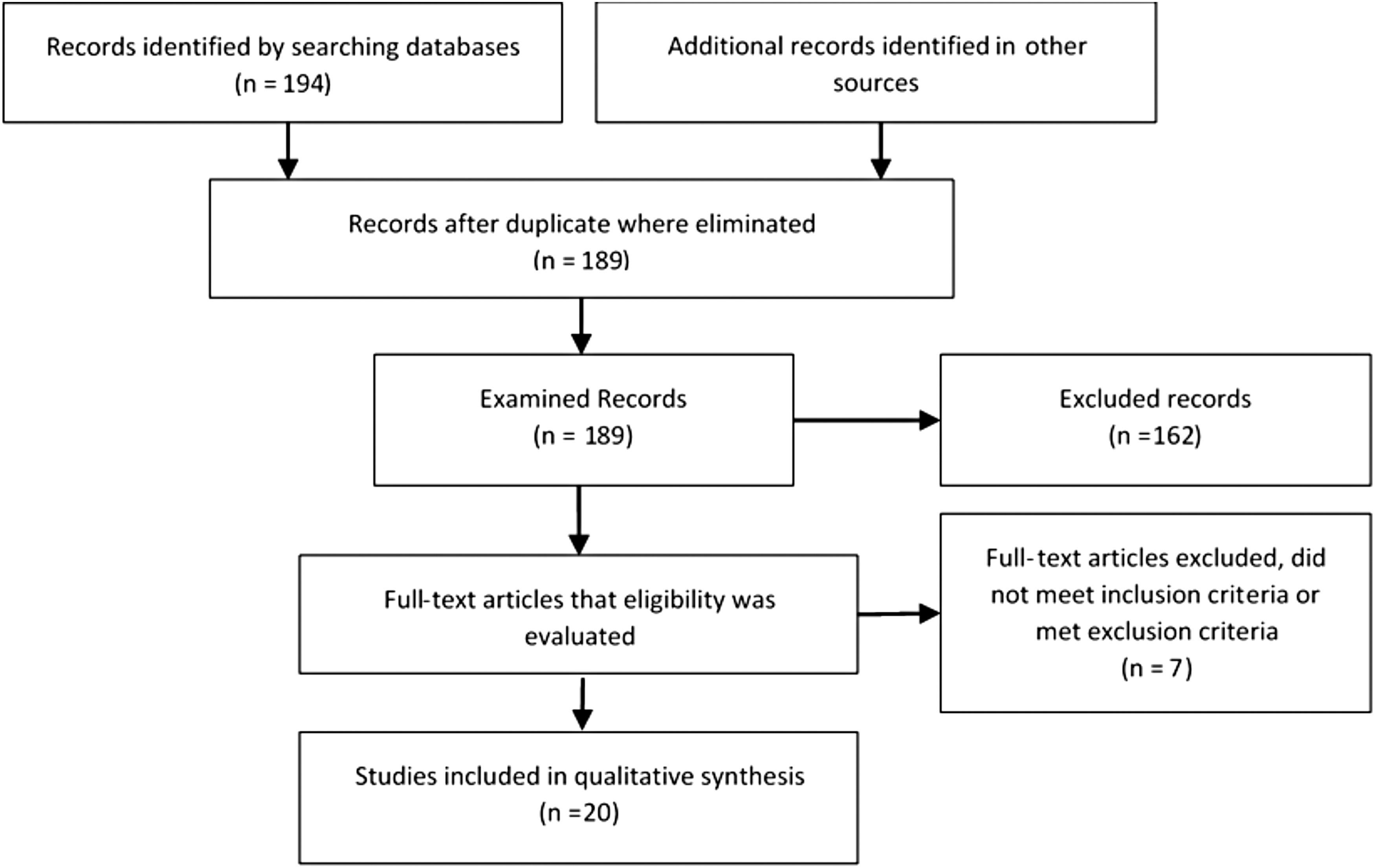
Process of study selection.
Pulse Oximetry Device Used and Duration of SpO2 Measurement
SpO2, oxygen saturation as measured by pulse oximetry.
Studies in the wake and sleep states
The results of studies for SpO2 during the wake state are shown in Tables 2–4 across three different geographic regions. Sleep data are shown in Table 5. The most relevant findings are as follows: diurnal awake SpO2 is lower as altitude increases (for illustrative data, see Fig. 2) and is lower at the same altitude during sleep and infant feeding in comparison to the wake state; in younger children, the range of normal diurnal SpO2 increases with increasing altitude, so, for example, varying by 5% in children aged 1–5 years at 2500 masl, in comparison with 12% in the same age group at 5100 masl, with this phenomenon being more marked during sleep. At high altitude, SpO2 increases with age and a significant gap between wake and sleep states occurs in the first months of life and narrows as the age increases; for example, Hill et al. (2016a) report that at 3700 masl, the median difference in infants aged 6–10 months between the wake versus sleep stage is 6%, compared with 3% between the ages of 13 and 17 years (Fig. 3). SpO2 dispersion at high altitude is wider at younger ages (for illustrative data, see Fig. 4), and SpO2 peak values are attained at older ages as altitude increases.

SpO2 5th percentile at different altitudes in two age groups in Peru. Graphic built with data from Rojas-Camayo et al. (2018) 5th percentile data provided to offer potential thresholds below which children require further clinical evaluation. SpO2, oxygen saturation as measured by pulse oximetry.
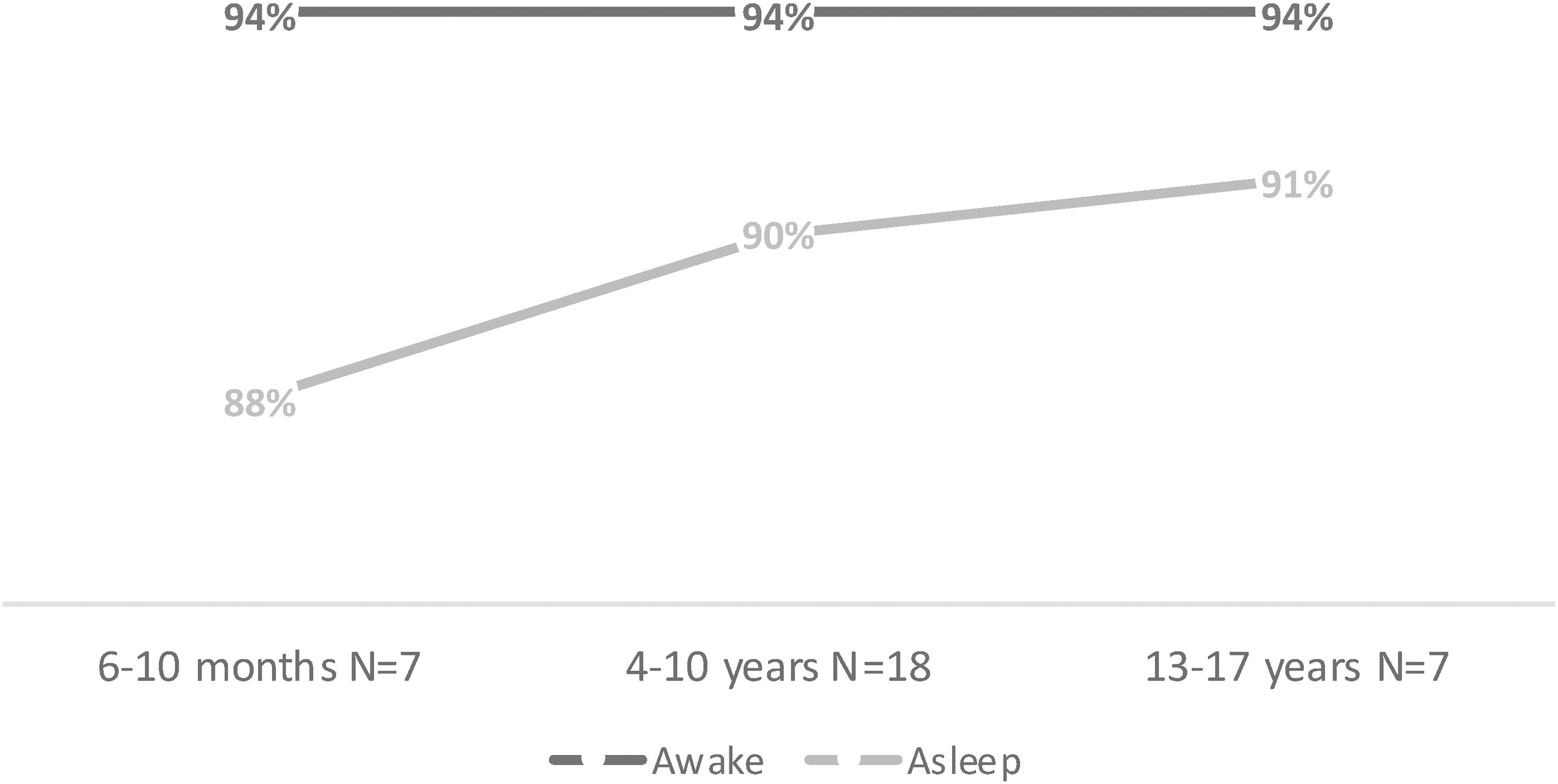
Gap between SpO2 medians in wake and sleep states in children aged from 6 months to 17 years at 3700 masl in Bolivia. At low altitude, SpO2 developmental differences were evident between infants and children in relation to 3% dips and were statistical significant (p = 0.019). These differences were more striking at high altitude (p < 0.001). Graphic built with data from Hill et al. (2016a). masl, meters above sea level.
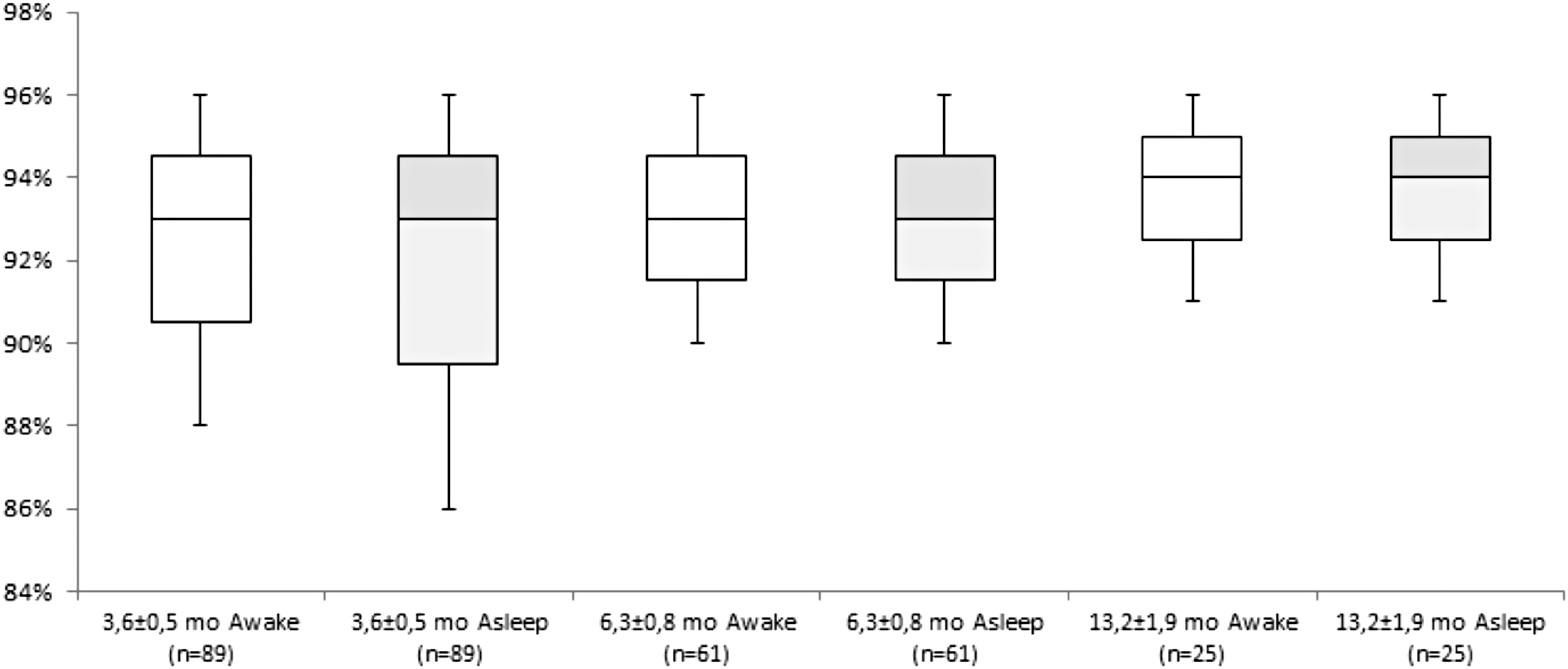
SpO2 at 2640 masl in awake and asleep infants aged from 3 to 15 months in Colombia. In 3.6 ± 0.5-month-old subjects (awake and asleep), SpO2 nadir, time with SpO2 <90%, and oxygen desaturation index were significantly higher in comparison with the two other age groups (p < 00.1). Graphic built with data from Duenas-Meza et al. (2015).
Resting SpO2 in High-Altitude Resident Andean Children During the Wake State by Age Group and Altitude (Ordered from Lower to Higher Altitude)
CI, confidence interval; IQR, interquartile range; masl, meters above sea level; p5th, 5th percentile; p95th, 95th percentile; SD, standard deviation.
Resting SpO2 in High-Altitude Resident Himalayan Children During the Wake State by Age Group and Altitude
Resting SpO2 in High-Altitude Resident Children During the Wake State by Age Group and Altitude in Colorado, USA
SpO2 in Sleeping Children at Different Ages and High Altitudes Across the World
Studies during infant feeding and crying
Five studies analyzed SpO2 during feeding in infants aged up to 5 months at high altitude (Table 6). The data show an SpO2 decrease between 0.2% and 6% when wake and feeding states are compared, with a mean decrease of −2.2%. Only one study reported SpO2 differences in infants when crying compared with quiet wakefulness (Gamponia et al., 1998); this study included 19 infants aged 0–5 months at 4018 masl and noted a 0.8% decrease in median SpO2 in crying infants.
SpO2 in Feeding Infants at Different Ages and High Altitudes Across the World
Studies reporting ethnicity and sex influences
Three studies reported the influence of ethnicity and sex on waking SpO2 variables. One study in Tibet at 3200 masl (Weitz and Garruto, 2007) reported a significant sex-by-ethnicity interaction in 15–19 year-olds, such that Tibetan females had higher SpO2 values than Tibetan males, but among Chinese Han born at this high altitude, males had higher SpO2 values than females (the Han population originate from lowland plains in Eastern China). A study from Peru at 4100 masl found no differences in SpO2 values between males and females, but children from the Nuñoa ethnicity had higher SpO2 levels in comparison with children from Tintayá and Marquirí ethnicities (Huicho et al., 2001), all ethnicities being highlanders. Finally, a study at 3800 masl reported that Tibetan 5–9 year-olds had significantly higher SpO2 values than Han children did at the same age (Niermeyer et al., 1995).
Statistical distribution
In 12/20 studies, a normal distribution was assumed by the authors who reported mean values, but without specification of the statistical test used to reach this conclusion. In 2/20 studies, a nonnormal distribution can be deducted from the data, but the statistical bias is not known; in 6/20 studies, a left-skewed nonnormal distribution was found (Torres et al., 1999; Ucrós et al., 2015, 2017; Hill et al., 2016a, 2016b; Rojas-Camayo et al., 2018). A review of the source data from studies by Hill and Rojas-Camayo confirmed that the data distribution has a negative bias. In Figure 5, the SpO2 left-skewed distribution at different altitudes and ages is shown. In Figure 6, the increase in the difference between 5th percentile and 95th percentile as altitude increases can be seen reflecting how the left bias is more evident as altitude increases.
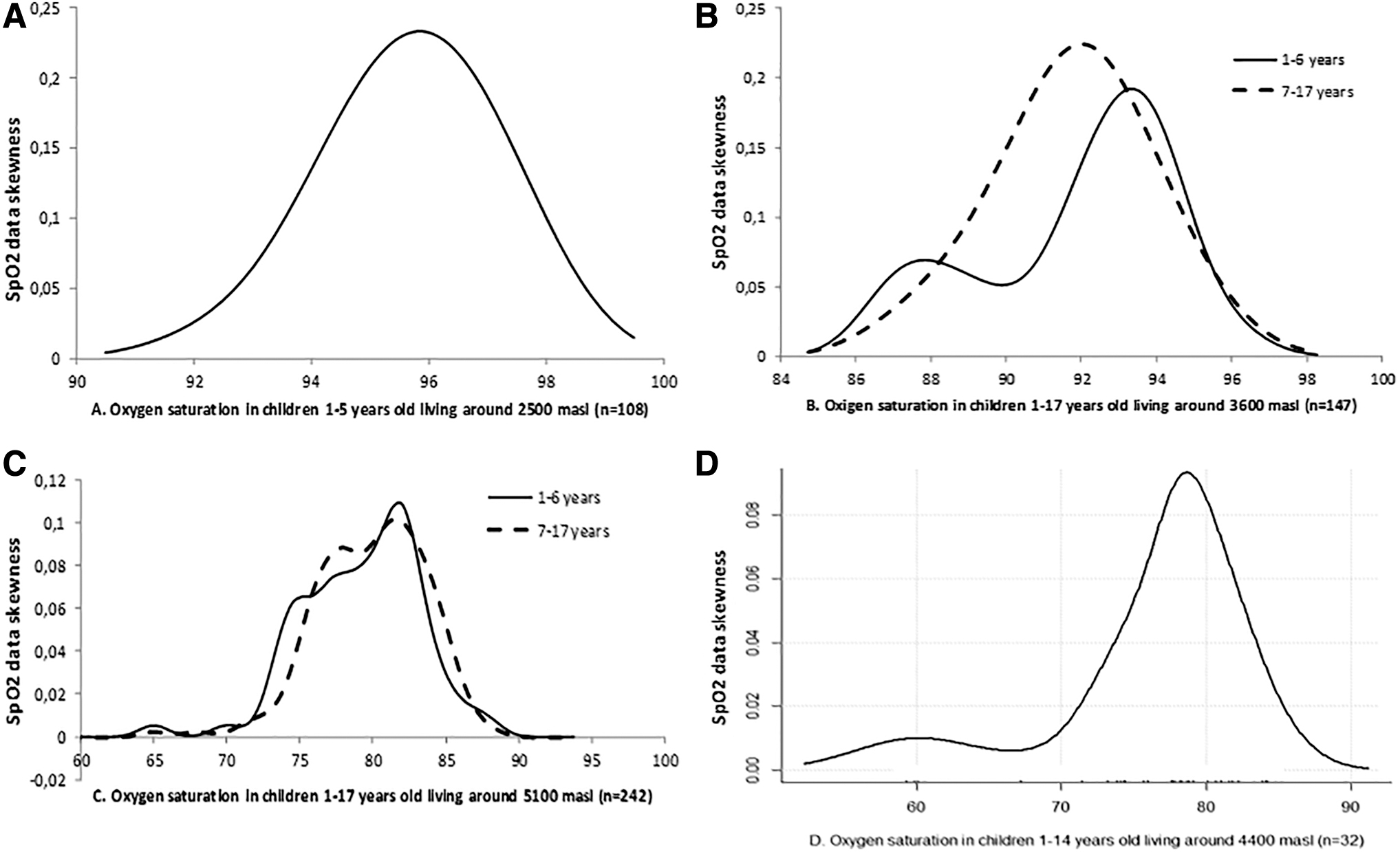
Consistent SpO2 left skew at different altitudes and age groups.
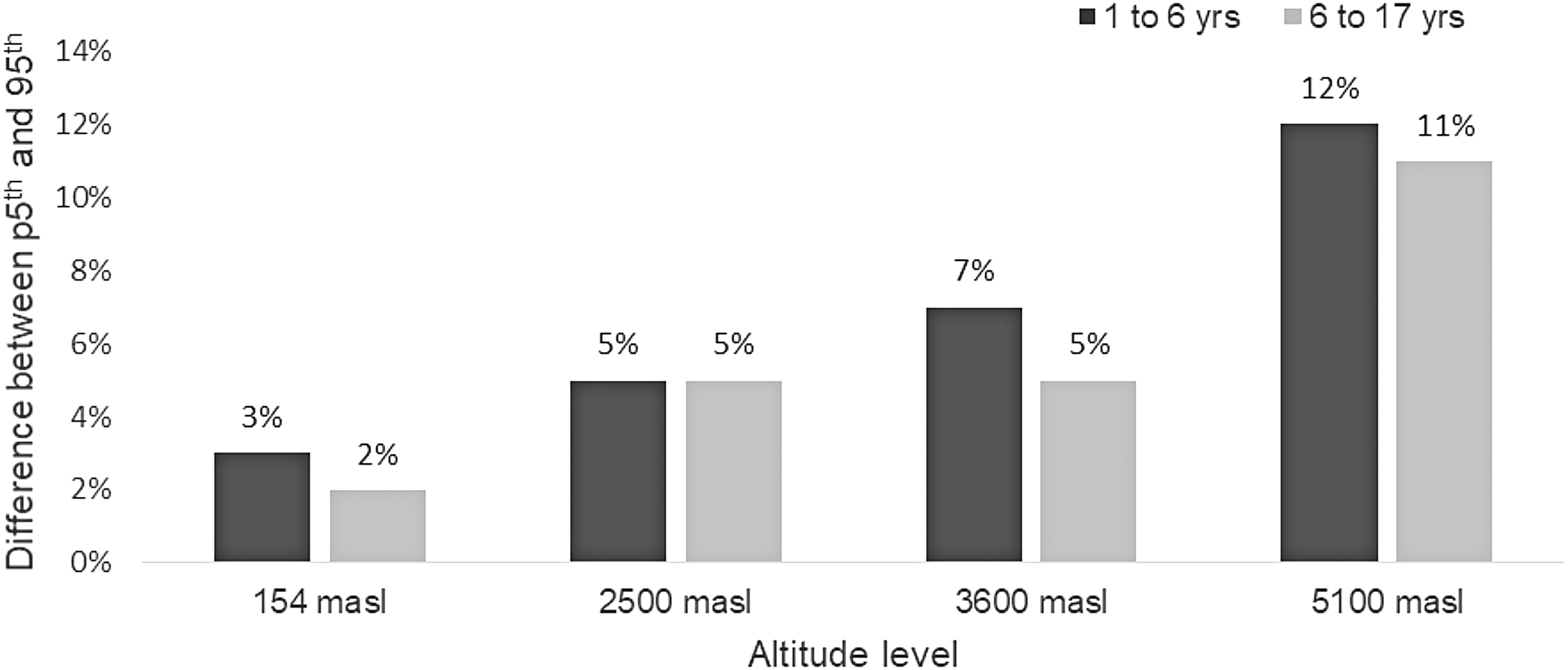
SpO2 difference between 5th percentile and 95th percentile in two age groups at different altitudes. Graphic built with data from Rojas-Camayo et al. (2018).
The comparison of SpO2 values from the first quartile with those from the second to fourth quartiles grouped, using data from Rojas-Camayo et al.'s study, indicated statistically significant differences in all altitude/age groups analyzed (Table 7).
Differences in SpO2 Between Quartiles 1 and Quartiles 2–4 at Several Altitudes and Age Groups
Table built with data from Rojas-Camayo et al. (2018).
Hb concentration measurement
Hb concentration was only measured in two studies (Ramírez-Cardich et al., 2004; Mattos et al., 2005). Oxygen-carrying capacity was not calculated in any of the studies.
Discussion
To the best of our knowledge, this is the first systematic review to examine the influence of high altitude on SpO2 across childhood from 0 to 19 years of age. It builds on data published by Subhi et al. (2009), which was limited to six studies above 2500 masl (rather than the 20 included here), and to pre-adolescent children. Furthermore, we included data on infants when feeding and report key differences between wake and sleep states.
Data provided by this review show that SpO2 at high altitudes increases through childhood; this phenomenon was highlighted by Beall (2000) who reported that at altitudes between 3800 and 4200 masl, SpO2 peak values were attained by 11 years of age and were 7% higher than values in young infants. The SpO2 improvement with age can be viewed as a marker of physiological adaptation or “SpO2 maturation” (Hill et al., 2016a); interestingly, SpO2 maturation is not a phenomenon exclusive to high altitude and is also seen at sea level (Schlüter et al., 2001). In addition, the present review shows that interindividual variability in SpO2 is higher at younger ages (Figs. 3, 4, and 6). This point was also noted by Beall (2000) and has been observed in subsequent studies (Duenas-Meza et al., 2015). This interindividual variation increases with altitude and is more marked during sleep (Figs. 3, 4, and 6) (Duenas-Meza et al., 2015; Ucrós et al., 2015, 2017; Hill et al., 2016a) and during feeding in young infants (Niermeyer et al., 1993, 1995; Torres et al., 1999). In consequence at altitudes >2500 masl, SpO2 treatment thresholds may change depending on sleep–wake or feeding status, especially in young infants.
The lower SpO2 values during sleep are normal in children, even at sea level (MacLean et al., 2015), and could be related with drops in respiratory rate and functional residual capacity, as well as increase in upper airway resistance (Marcus, 2001). What emerges from the present review is that the SpO2 gap between wake and sleep stages is notable at high altitude. The explanation for lower SpO2 values during feeding in infants is less certain; a recent study in infants, aged 2 weeks–3 months with cardiac disease, showed significant desaturation (mean −2.8%) during feeding, but no drop in a healthy age-similar control group (Miranda et al., 2019). The lower baseline SpO2 values in the infants with cardiac disease are similar to those seen in Andean infants at the threshold of high altitude; this suggests that minor perturbations in ventilation associated with infant feeding may become critical when baseline SpO2 is lowered. As it is known, from the O2 dissociation curve, at high altitude, mild changes in PaO2 induce significant SpO2 drops (Chernick and West, 1990).
In relation with lower SpO2 values during sleep in children, it is known at sea level that normal sleep onset prompts a fall in respiratory rate, functional residual capacity, and an increase in upper airway resistance (Marcus, 2001) and that small decrements in oxygen saturation (e.g., 1%–2%) are acceptable (MacLean et al., 2015). Regarding differences by sex, it has been found in adults aged 30–40 years at high altitude, higher SpO2 levels in females than in males (Beall, 2000), but similar findings are not evidenced in the pediatric literature (Huicho et al., 2001).
An interesting question is why SpO2 maturation occurs. It could be hypothesized that since periodic breathing (PB) is much more important at high altitude during the first months of life (Duenas-Meza et al., 2015; Ucrós et al., 2015, 2017), there could be a link between SpO2 increase and decrease in PB with age. We found two studies in infants, which explored this possible association. The first was carried out by Parkins et al. (1998), who exposed 34 healthy infants to a 15% oxygen environment during a mean of 6.3 hours of sleep and measured oxygen saturation, frequency of isolated and periodic apnea, and frequency of desaturation. In the later published by Ucrós et al. (2015), oxygen saturation, PB, and apnea indexes were measured during a mean of 4.1 hours of sleep at 2560 masl in infants aged between 1 and 4 months. Neither study found an association between the mean SpO2 and PB. Similarly, studies carried out in adults have not found this correlation (Salvaggio et al., 1998; Insalaco et al., 2012; Ainslie et al., 2013). A second hypothesis could be related to possible changes in ventilation across childhood at high altitude, nevertheless studies undertaken by Beall on different populations do not support this theoretical mechanism; this research showed that Tibetans were more hypoxic than Aymara, despite a higher resting ventilation and hypoxic ventilatory responses (Beall et al., 1997). A third mechanism, and probably the most plausible hypothesis, is that as pulmonary pressure falls through childhood, the SpO2 gradually increases (Penaloza and Arias-Stella, 2007). The question that would then remain is why pulmonary pressure shows such behavior in children living at high altitude.
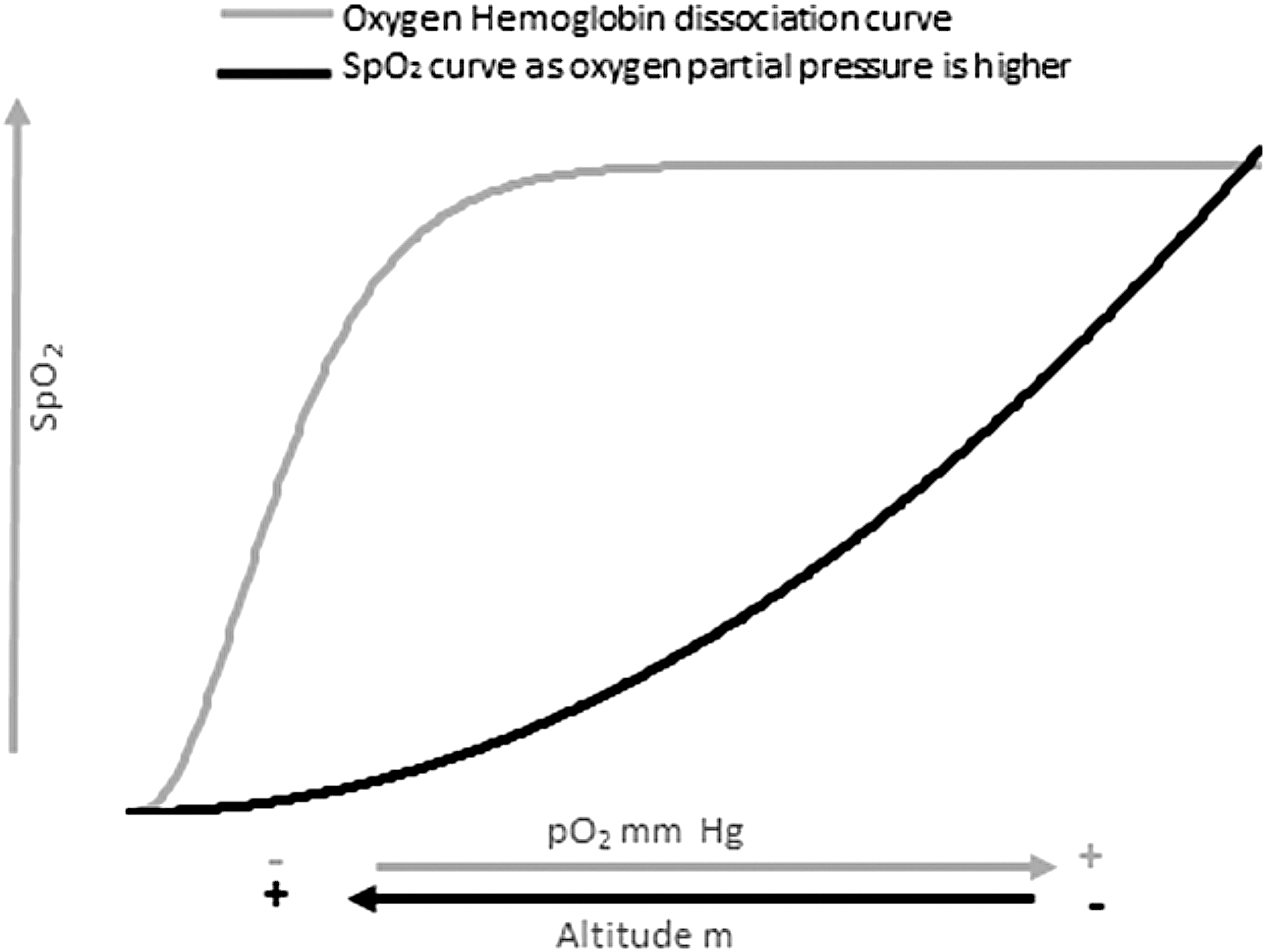
In six studies, data explicitly demonstrated a nonnormal SpO2 left-skewed distribution, meaning significant interindividual differences in SpO2 at a same age and altitude. This phenomena was also noted when data from an early study published in 1963 were reanalyzed; in this research, oxygen saturation was measured in blood of children living around 4400 masl (Sime et al., 1963) (Fig. 5). The striking feature of a left-skewed SpO2 distribution has been found consistently across different altitudes, ages, and sleep versus wake states. At high altitude, the SpO2 nonnormal statistical distribution delivers a parabolic curve, which has to be differentiated from the sinusoidal oxygen dissociation curve related to the capacity of Hb to carry oxygen. This concept is illustrated in Figure 7 (Chernick and West, 1990; Penaloza and Arias-Stella, 2007).
We speculate that children with low steady-state oxygen saturation measures during health may be at increased risk of later life chronic mountain sickness (CMS) in its different forms. These include CMS with altitude polycythemia or Monge's disease (Villafuerte and Corante, 2016); high-altitude heart disease (HAHD) or high-altitude pulmonary hypertension, which occurs without polycythemia (Ge and Helun, 2001; Aldashev et al., 2002; Reeves and Grover, 2005; Kojonazarov et al., 2007; Xu and Jing, 2009); and mixed CMS, which includes both excessive polycythemia and pulmonary hypertension-related HAHD (Ge and Helun, 2001). These different kinds of progressive life-limiting conditions affect 5%–10% of high-altitude residents in the first category (Leon-Velarde et al., 2005), and 5%–18% in the second one (Mirrakhimov and Strohl, 2016). To the best of our knowledge, childhood predictors of CMS have not been reported. The etiology of this condition is likely to be multifactorial, including genetically determined differences in erythropoiesis regulation, as demonstrated by Stobdan et al. (2017) who identified novel genes involved in high-altitude adaptation in the Andes; alterations in ventilatory responses to hypoxia (Villafuerte and Corante, 2016); hypoxia gene expressions related to CMS (Xing et al., 2008; Stobdan et al., 2017); and levels of mediators related to lung vascular reactivity (Aldashev et al., 2002; Kojonazarov et al., 2012). Longitudinal studies of SpO2 across childhood would be of value in this context.
The present study has several limitations. First, different oximeter devices and/or protocols for measuring SpO2 were used across the different studies, and in most studies, we do not have information relating to important equipment settings, such as sampling rate and averaging time (Hill and Evans, 2016). Second, the data available across the publications used different approaches for central tendency measures, with some studies reporting means while others reported medians. Similarly, in relation to dispersion, different measures were used including percentiles, standard deviation, confidence intervals, and interquartile ranges. Third, ethnic background is a key influence on high-altitude adaptation, and data presented here represent populations with different adaptive mechanisms. Fourth, only two studies measured Hb concentration levels. Importantly, SpO2 alone is a limited indicator of oxygen delivery to the tissues, especially in the setting of polycythemia.
However, this review also has notable strengths. In total, 20 studies were analyzed, which included 8347 SpO2 data; furthermore, the quality assessment of most studies was high with a low risk of bias. Importantly, diurnal–nocturnal variation highlighted from sleep data cannot be accounted for by Hb concentration fluctuations, suggesting genuinely compromised adaptation to high altitude in some children that may have implications for later life CMS vulnerability. Finally, the data synthesized in this review offer interesting insights into the concept of SpO2 maturation at high altitude.
The need for international reference data on ranges of SpO2 across childhood at high altitude remains pressing. Future studies should use standardized oximetry protocols (uniform devices and settings) and standardized reporting of data to confidently establish such reference data in healthy children to support clinical decision-making. In the meantime, the data synthesized in this review provide a preliminary guide for clinicians managing children with cardiorespiratory disorders at high altitude.
Conclusions
At high altitude, the mean/median SpO2 improves in infants and children with aging; a significant gap between wake and sleep states is seen in the first months of life, which narrows as the infant gets older; SpO2 dispersion at high altitude is wider at younger ages; at high altitude, SpO2 shows a nonnormal distribution skewed to the left; this bias becomes more evident as altitude increases, at younger ages and during sleep. SpO2 has interindividual differences at a same given age and altitude, being significantly lower in one of four children. Collaborative studies using similar oximeters/protocols for measuring SpO2 at different altitudes in healthy children across high-altitude geographical regions are urgently needed.
Footnotes
Acknowledgments
The authors thank Mr. Gerardo Ardila, Statistician, MSc, of the Research Department of the Fundación Santa Fe de Bogotá, for his valuable help in the construction of graphics and statistical analysis; Dr. Jose Rojas-Camayo of the Instituto de Investigaciones de la Altura, Universidad Peruana Cayetano Heredia, Lima, Peru, for providing raw data from the publication “Reference values for oxygen saturation from sea level to the highest human habitation in the Andes in acclimatised persons” (Rojas-Camayo et al., 2018); and Prof. Romola Bucks of the University of Western Australia for providing raw data from the DeSat study (Hill et al., 2016a, ![]() ).
).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.