
Abstract
Background:
The stress of high altitude alters vascular permeability, which may be related to structural changes in the endothelial glycocalyx. We aimed to study these changes by measuring plasma concentrations of several glycocalyx components upon exposure to high altitude.
Methods:
Plasma collected from 17 subjects at low altitude (423 m) and at three time points (7, 20, and 44 hours) after rapid ascent to high altitude (4559 m) were evaluated for concentrations of three glycocalyx components: syndecan-1, intercellular adhesion molecule-1 (ICAM-1), and heparan sulfate. Vital signs and echocardiographic measurement of systolic pulmonary artery pressure (sPAP) and cardiac output were also obtained at low and high altitudes.
Results:
Mean age of the study population was 35.5 ± 11.2 years with a body mass index of 22.7 ± 2.5 kg/m2. Concentrations of ICAM-1 and heparan sulfate increased from baseline to 7 hours after arrival at high altitude; the ICAM-1 rise persisted at 20 hours. Syndecan-1 concentrations were increased only at 44 hours. Increased ICAM-1 concentrations correlated with sPAP and peripheral edema. Elevations in heparan sulfate appeared to correlate with acute mountain sickness (AMS).
Conclusions:
Levels of circulating glycocalyx components increase after exposure to high altitude and may correlate with AMS. Measuring plasma concentrations of various glycocalyx components could serve as a useful tool for further evaluation of vascular endothelial injury and repair in illness at high altitude.
Introduction
Upon ascent to altitudes above 1600 to 2500 m, numerous changes and stresses occur that alter the systemic and pulmonary vasculature. In the systemic circulation, hypoxia and hypoxemia cause vasodilation directly, but this sometimes can be overridden over time by activation of the sympathetic nervous system and its vasoconstricting effects. In the syndrome of acute mountain sickness (AMS), several nonspecific symptoms and signs, for example, headache, gastrointestinal distress, and development of peripheral edema, might represent alterations in the integrity of the systemic vascular endothelium leading to changes in permeability. Even greater changes in the permeability, respectively, of the lung and brain vasculature occur in high-altitude pulmonary edema (HAPE) and high-altitude cerebral edema. In support of greater peripheral vascular permeability, Hansen et al. (1994) found that the transcapillary escape rate of isotopically labeled albumin was increased in humans after a rapid and passive ascent to 4350 m, but could not confirm this in a subsequent study (Poulsen et al., 1998). Similar to the negative study of Poulsen et al. (1998), Kleger et al. (1996) found that there was no increase in the transcapillary escape rate for labeled albumin in those without illness and those with AMS, but a slight increase in those with HAPE. Neither study correlated their measurements of transvascular escape of albumin with the development of peripheral edema.
While systemic blood pressure may modestly increase in some at high altitude, the magnitude of pulmonary artery pressure (PAP) elevation is significantly greater in absolute and percentage terms (Swenson, 2013). The magnitude of hypoxic pulmonary vasoconstriction (HPV) is determined by the intrinsic hypoxic response of pulmonary smooth muscle cells (Dunham-Snary et al., 2017) and is modified by the vascular endothelium (Scherrer et al., 1996; Swenson et al., 2002; Berger et al., 2005, 2009; Bailey et al., 2010). Exaggerated and regionally inhomogeneous HPV plays a pivotal role in the pathophysiology of HAPE (Bartsch et al., 1991; Hopkins et al., 2005; Dehnert et al., 2006). The resulting hydrostatic stress causes both dynamic changes in the permeability of the alveolar capillary barrier and mechanical damage leading to leakage of fluid, large proteins, and erythrocytes into the alveolar space (West and Mathieu-Costello, 1999; Swenson and Bartsch, 2012).
The inner surface of blood vessels is lined with endothelial cells that are continually exposed to the mechanical shear stress of blood flow. On the luminal surface of these cells lies the glycocalyx, an essential component of the vascular barrier, which has only been recently recognized to play a critical role in determining the permeability characteristics of the vasculature. The vascular endothelial glycocalyx is composed of proteoglycans (e.g., syndecan-1 and heparan sulfate) and glycoproteins (e.g., intercellular adhesion molecule-1 or ICAM-1) and plays an important role in vascular protection, modulation, and hemostasis. The glycocalyx participates in mechanosensing that regulates nitric oxide production in response to both steady and oscillatory shear stress (Florian et al., 2003). Alteration or destruction of the glycocalyx in trauma, sepsis, and ischemia can lead to capillary leak, edema formation, and loss of vascular responsiveness (Becker et al., 2010).
With this prospective study we investigated changes of the endothelial glycocalyx barrier after rapid and active ascent to high altitude (4559 m). We hypothesized that the increased shear stress on the pulmonary and systemic vasculature resulting from acute hypoxic exposure and the exercise of active ascent alters the structure of the glycocalyx and can be detectable by appearance of its components in the circulating blood. Furthermore, we hypothesized that this may occur to a greater extent in those with peripheral edema and in those with AMS, in whom the shedding of glycocalyx may correlate with symptom severity.
Methods
Study approvals
The study was performed in accordance with the Declaration of Helsinki and its current amendments, and was approved by the Ethics Committee Salzburg, Austria, by the Ethics Committee of the University of Torino, Italy, and by the Competent Authority (BASG), Vienna, Austria. Before inclusion in the study all subjects provided written informed consent. The study was part of a trial investigating the effect of inhaled budesonide on AMS, the results of which were published elsewhere (Berger et al., 2017).
Subjects
Seventeen nonsmoking and nonacclimatized native lowlanders were included in the study. They belonged to the placebo control group of a previously published trial (Berger et al., 2017). None of the subjects spent time at altitudes >2000 m within the 4 weeks before study enrollment, and none took any regular medication. As the data sets were incomplete in three participants, the present analysis is based on data from 14 subjects. These subjects included 10 males and four females, with a mean (± standard deviation [SD]) age of 35.5 ± 11.2 years. To assess the physical fitness of the study group, all subjects performed an incremental exercise step test on a bicycle ergometer until exhaustion, starting with 40 W, an increment of 20 W per step, and 1-minute step duration.
Study protocol
Baseline evaluations were performed at an altitude of 423 m (Salzburg, Austria). Between 2 and 4 weeks later, subjects traveled to Alagna (1130 m), Valsesia, Italy, and ascended accompanied by licensed mountain guides to 4559 m (Capanna Regina Margherita, Monte Rosa) within ∼20 hours. The ascent consisted of transport by cable car (from 1100 to 3275 m) and continued with a 90-minute climb to the Capanna Giovanni Gnifetti (altitude, 3611 m), where the subjects spent one night. On the next morning they climbed to 4559 m (∼4 hours), where they spent two nights. Data were collected at 7, 20, and 44 hours after arrival at 4559 m.
Plasma measurements of glycocalyx components
Blood draws were performed on all subjects at low altitude and at several time points (7, 20, and 44 hours) after arrival at high altitude. Aliquoted plasma samples were stored frozen in liquid nitrogen until measurements were performed at the University Hospital Heidelberg, Germany. Commercial enzyme-linked immunosorbant assays were performed to determine the plasma levels of ICAM-1, heparan sulfate, and syndecan-1, as described previously (Rahbar et al., 2015; Papakonstantinou et al., 2016; Robert et al., 2017). Human syndecan-1 was measured using a kit from Abcam (Cambridge, UK) with a detection range of 8–256 ng/mL and an intra-assay precision of 6.2%. Human heparan sulfate was measured using a kit from BIOZOL (Eching, Germany) with a detection range of 15.6–100 pg/mL and an intra-assay precision of <8%. Human ICAM-1 was measured using a kit from BIOZOL with a detection range of 3.1–200 ng/mL and an intra-assay precision of <8%.
Echocardiography
Around each time point of blood sampling, transthoracic echocardiography (Philips CX50; Phillips Medical Systems, Andover, MA) was performed with a 1.0 – 5.0 MHz sector array transducer (Philips S5-1; Phillips Medical Systems) after the participants had rested for 5 minutes in the supine position. All measurements were made by the same experienced echocardiographer, with the subject lying in the left lateral decubitus position. For determination of systolic pulmonary artery pressure (sPAP), continuous wave Doppler was used to measure peak flow velocities of tricuspid valve regurgitation jets in the right ventricular inflow projection, as described previously (Berger et al., 2018). The highest coherent boundary of the spectral wave was used to calculate the right atrial to right ventricular pressure gradient using the modified Bernoulli equation (Rudski et al., 2010). For calculation of sPAP, 5 mmHg was added as an estimate for right atrial pressure (Yock and Popp, 1984). Left ventricular volumes were measured at end diastole (LVEDV) and end systole (LVESV), allowing for calculation of stroke volume (LVEDV–LVESV) and cardiac output (stroke volume × heart rate). All measurements were evaluated offline by two independent echocardiographers who were blinded to clinical and experimental data.
Vital signs and AMS
After 5 minutes of rest in supine position, heart rate and peripheral oxygen saturation (SpO2) were measured by pulse oximetry (Covidien Nellcor, Mansfield, MA) and resting central blood pressure was measured noninvasively by analyzing brachial artery waveforms (Pulsecor®, Auckland, New Zealand) (Lin et al., 2012). Subjects were evaluated, diagnosed, and treated for AMS based on standard diagnostic criteria as detailed elsewhere (Berger et al., 2017). The severity of peripheral edema was rated as: no edema = 0 points, edema at 1 location = 1 point, edema at ≥2 locations = 2 points.
Statistical analyses
Normal distribution of the data was tested using the Kolmogorov–Smirnov test. Effects of altitude were analyzed by one-way repeated measures analysis of variance (ANOVA) or by one-way repeated measures ANOVA on ranks, as appropriate. Pairwise multiple comparison procedures were made using Student–Newman–Keuls test. The relationship between pairs of variables was expressed with the Spearman correlation coefficient (R). Data are expressed as mean values ± SD. A p-value of <0.05 (two-sided) was considered significant. Statistics were performed using the SigmaStat® software package (SPSS, Inc., Chicago, IL).
Results
The study population had a mean height of 177.5 ± 10.7 cm, weight of 71.9 ± 11.8 kg, and body mass index of 22.7 ± 2.5 kg/m2. Maximal power output during the incremental step test was 4.13 ± 0.28 W/kg. Differences in hemodynamic, respiratory, and hematologic parameters between low and high altitude are shown in Table 1. Ascent to high altitude decreased SpO2 and increased heart rate (p < 0.001). The central systolic blood pressure remained unchanged at high altitude, whereas the central diastolic blood pressure increased (p < 0.01). Cardiac output increased on arrival at altitude, and this increase was significant after 20 and 44 hours (p < 0.05). Ascent to high altitude also increased sPAP (p < 0.05). The incidence and severity of AMS among the subjects are summarized in Table 2.
Hemodynamic, Respiratory, and Hematologic Parameters of 14 Subjects at Low Altitude and at 7, 22, and 44 Hours After Reaching High Altitude
All data are shown as mean ± SD.
p < 0.05 when compared against baseline (LA). Values are mean ± SD.
DBP, diastolic blood pressure; HA, high altitude (4559 m above sea level); Hb, hemoglobin; Hct, hematocrit; LA, low altitude (423 m above sea level); ND, not done; SBP, systolic blood pressure; SD, standard deviation; sPAP, systolic pulmonary artery pressure; SpO2, peripheral oxygen saturation.
Incidence and Severity of Acute Mountain Sickness in the 14 Subjects After Arrival at 4559 m
AMS was defined as a LL score ≥5 in combination with an AMS-C score >0.7. The overall incidence of AMS, which reflects all subjects that were classified as AMS-positive at least at one time point, was 53% (9/17). The total number of subjects per group decreased over time due to drop-outs caused by severe AMS and treatment with oxygen and acetazolamide. All data are shown as mean ± SD.
LL, Lake Louise.
The plasma concentrations of various glycocalyx components (ICAM-1, heparan sulfate, and syndecan-1) measured at low and high altitude are shown in Figures 1 and 2. Ascent to high altitude increased the plasma concentrations of all three measured glycocalyx components (all p < 0.05; Fig. 1), but these peaks occurred at different time points. While the plasma concentrations of ICAM-1 and heparan sulfate peaked after 7 hours at high altitude, the increase in syndecan-1 plasma levels occurred after 44 hours. Subjects with AMS had a significantly greater altitude-induced increase in heparan sulfate than those without AMS (p < 0.05; Fig. 2b). In contrast, there were no observed differences in altitude-induced changes in ICAM-1 and syndecan-1 between subjects with and without AMS (p > 0.05; Fig. 2a, c).

Box plots of plasma concentrations of the glycocalyx components in the 14 subjects at LA and at 7, 20, and 44 hours after reaching HA showing median values and 10th, 25th, 75th, and 90th percentile ranges of the data.
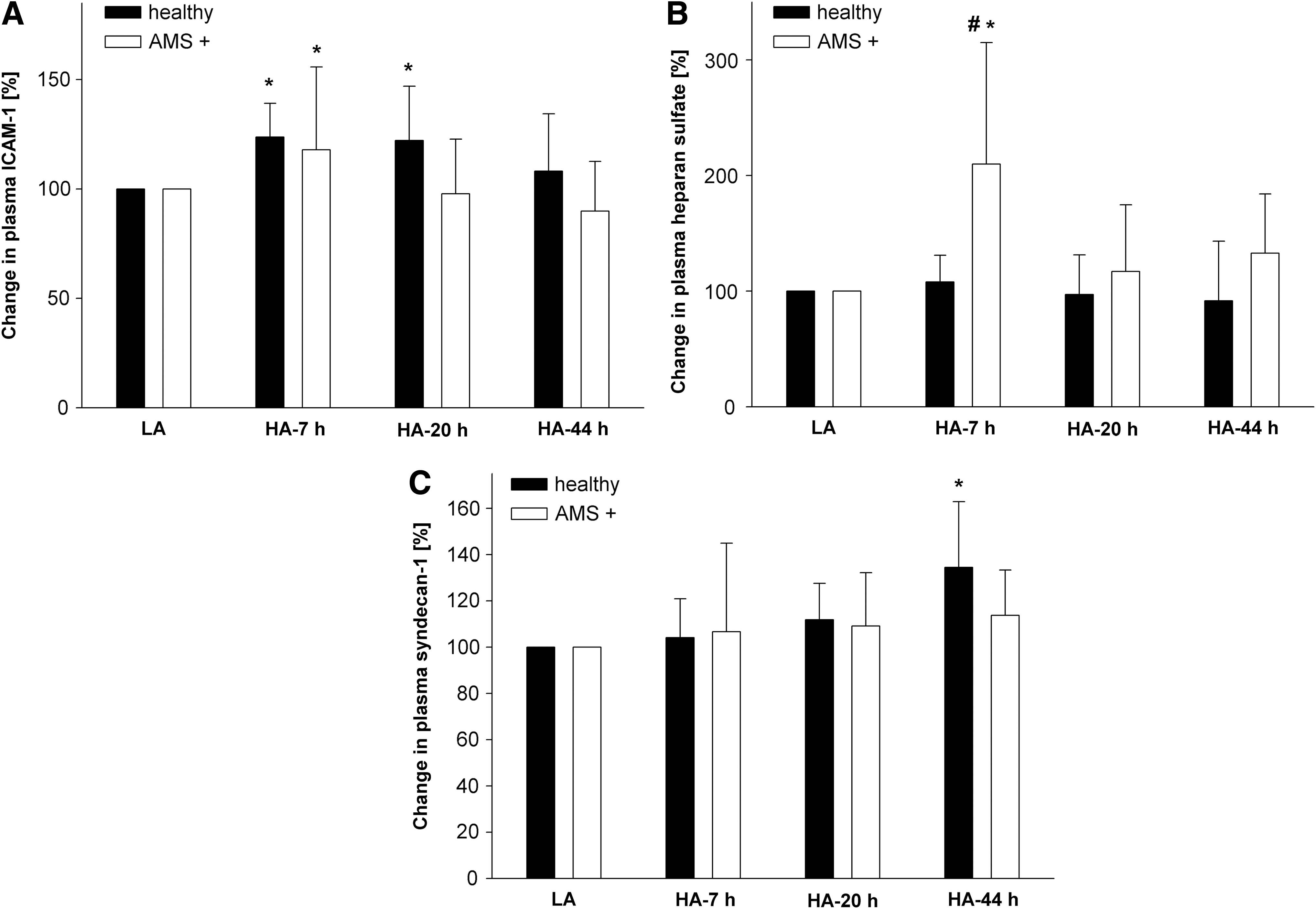
Changes in plasma concentrations of glycocalyx components in the 14 subjects between LA and at 7, 20, and 44 hours after reaching HA in subjects with and without AMS.
Changes in concentrations of measured plasma glycocalyx components were also compared against changes in hemodynamic and respiratory parameters at altitude. A significant correlation was observed between the altitude-induced increase in sPAP and the increase in plasma ICAM-1 concentrations (p < 0.01; Fig. 3); however, a positive correlation with sPAP was not found with plasma concentrations of heparan sulfate or syndecan-1 (p > 0.10; data not shown). A significant correlation was observed between the altitude-induced decrease in SpO2 and the increase in plasma concentrations of heparan sulfate (R = −0.41, p < 0.01; Fig. 4). In contrast, no association was found between the degree of oxygen desaturation and the change in ICAM-1 (p = 0.08) or syndecan-1 (p = 0.56). No significant association was observed between the measured glycocalyx components and resting cardiac output (all p > 0.12; data not shown).
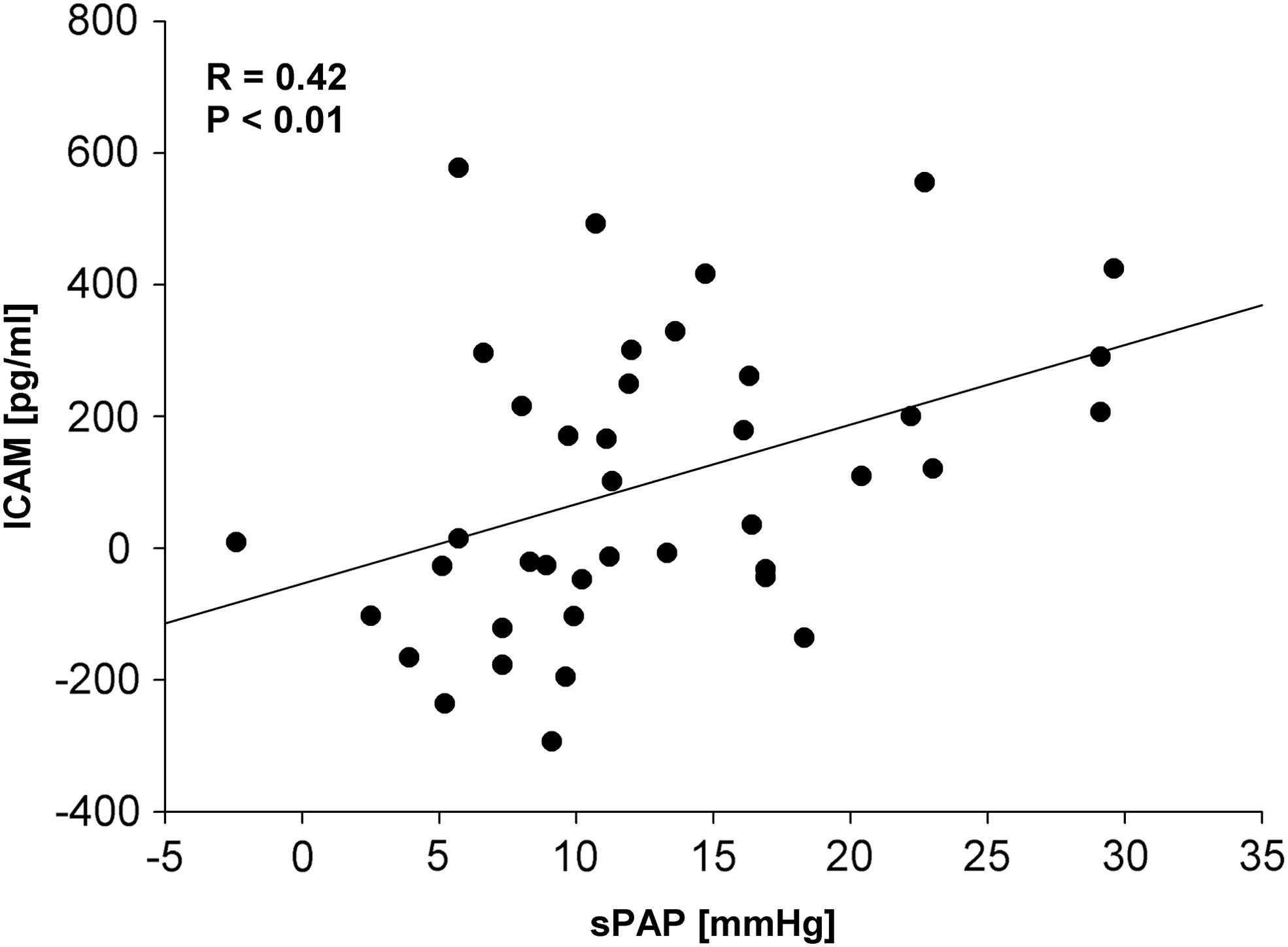
Association between the altitude-induced change in ICAM-1 plasma concentration and sPAP in the 14 subjects assessed after 7, 20, and 44 hours at 4559 m. sPAP, systolic pulmonary artery pressure.
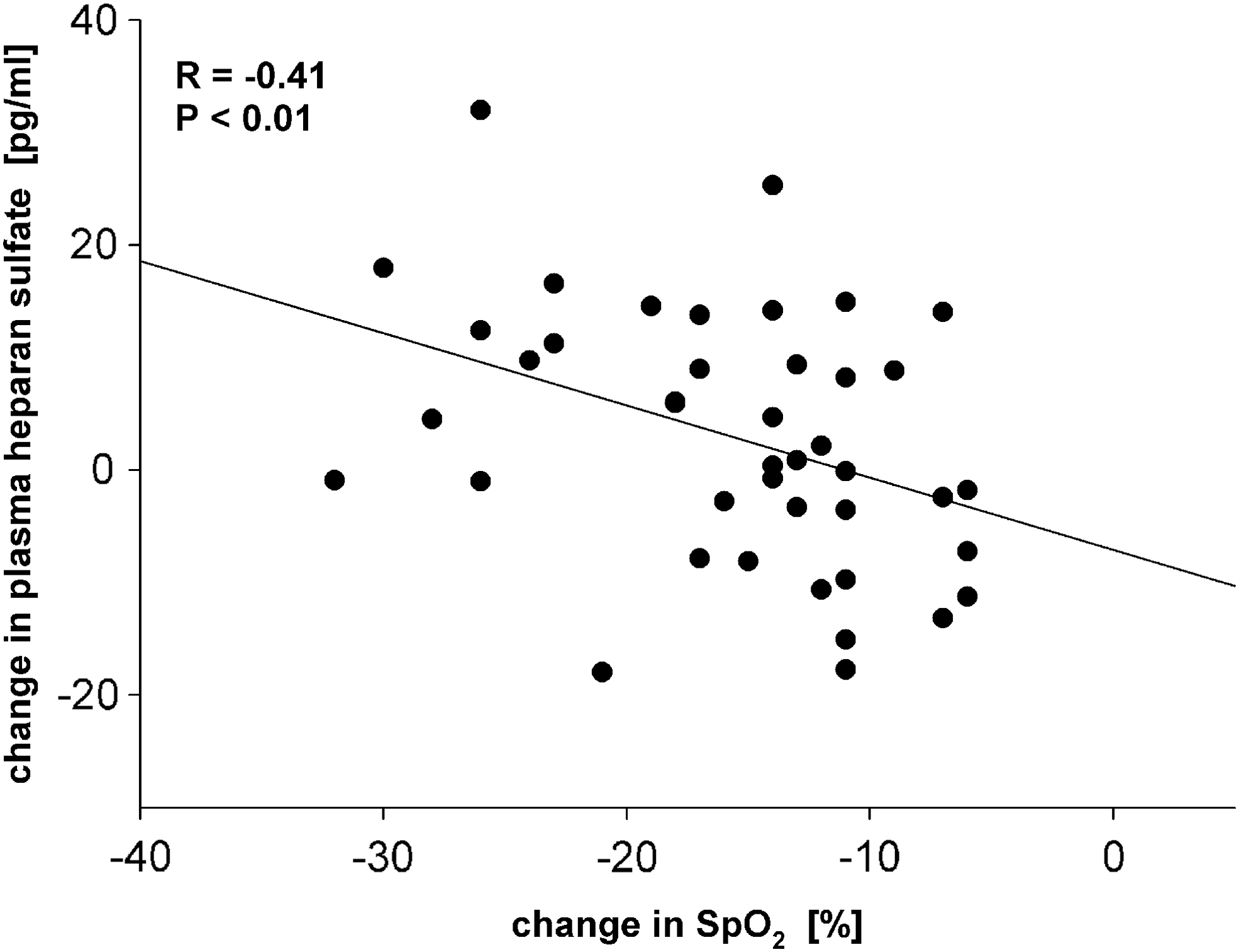
Association between the altitude-induced change in SpO2 and plasma heparan sulfate concentration in the 14 subjects measured after 7, 20, and 44 hours at 4559 m. SpO2, peripheral oxygen saturation.
Plasma ICAM-1 concentrations at high altitude did correlate with the severity of peripheral edema, while plasma heparan sulfate and syndecan-1 concentrations did not (Table 3). The severity of peripheral edema did not correlate with the severity of AMS (R = 0.160, p = 0.312). The correlation analysis between the glycocalyx parameters and edema severity was based on the pooled data of the 14 subjects at 7, 20, and 44 hours after arrival at high altitude. As specified in the methods section, the statistical test for the correlation analysis was the Spearman correlation coefficient.
Correlation Between the Presence of Peripheral Edema and Plasma Glycocalyx Components in the 14 Subjects After Arrival at 4559 m
The severity of peripheral edema was rated as: no edema = 0 points, edema at 1 location = 1 point, edema at ≥2 locations = 2 points.
ICAM-1, intercellular adhesion molecule-1.
Discussion
Increases in circulating glycocalyx components and disruption of the glycocalyx are associated with various stressors to the vascular endothelium, including sepsis (Iba and Levy, 2019), trauma (Tuma et al., 2016), heavy exercise (Lee et al., 2019), ischemia/reperfusion injury (van Golen et al., 2014) and hypoxic exposures (Johansson et al., 2014). Our study is the first to demonstrate that there is increased shedding of glycocalyx components upon the stress of exposure to high altitude. Based on plasma measurements alone, it is not possible to determine the source of these glycocalyx components in our study. However, one could postulate that altitude-induced increases in pulmonary artery shear stress lead to increased shedding of the glycocalyx lining of the pulmonary vascular endothelium. Indeed, our subjects underwent significant pulmonary hemodynamic changes after 7 hours at high altitude (including a 32% increase in resting heart rate and 65% increase in resting sPAP) that would induce an increase in pulmonary vascular shear stress (Table 1). Lending credence to this theory, we note a positive correlation between sPAP and circulating ICAM-1 concentrations (Fig. 3). Furthermore, the correlation of plasma ICAM-1 elevations with the development of peripheral edema (Table 3) also points to a vascular stress in the circulation leading to alterations in systemic capillary permeability in some individuals.
There appears to be a significant heterogeneity in both the composition and time course of these circulating markers of glycocalyx alteration. Our results indicate that while circulating ICAM-1 concentrations and heparan sulfate increase significantly with acute altitude exposure, there is no significant change in syndecan-1 concentrations (Fig. 1): a finding at odds with studies of other disease states (including trauma) as well as a shorter study of hypobaric hypoxia (Johansson et al., 2014). As to the temporal changes at high altitude in ICAM-1 and heparan sulfate concentrations, both were highest at 7 hours and then declined, however, the opposite trend was the case for syndecan-1. Other studies of the timing of these glycocalyx concentration changes in other stresses such as aortic surgeries with periods of no-flow ischemia suggest that syndecan-1 appears earliest (Rehm et al., 2007). This heterogeneity across studies in temporal appearance may be related to the differences with hypoxia versus ischemia and to the total extent of cell injury and stress that both elicit.
Intriguingly, elevations in plasma concentrations of heparan sulfate at altitude appear to correlate only with those subjects who developed AMS and were associated with decreased oxygen saturation (Fig. 2). Furthermore, time since injury appears to be an important variable (Figs. 1 and 2). While heparan sulfate levels quickly returned to baseline, ICAM-1 levels remained elevated at 20 hours and syndecan-1 only was elevated at 44 hours, suggesting heterogeneity in the timing of glycocalyx alteration and repair or clearance kinetics. These findings demonstrate that the stress of high altitude and hypoxia induce complex alterations in the vascular glycocalyx, which are dependent on both the time and degree of injurious exposure and possibly the body's response to altitude, specifically the rise in PAP and magnitude of arterial hypoxemia and systemic hypoxia. Specifically, we did find significant associations with the rise of certain glycocalyx components with increases in sPAP (Fig. 3) and declines in peripheral oxygenation (Fig. 4) in a dose-dependent manner.
It may be questioned whether the increases in these three glycocalyx components are simply the result of the heavy exercise in climbing. Although Lee et al. (2019) found increases in circulating syndecan-1 after 45 minutes of stationary cycling in normoxia, we did not observe a rise at 7 hours after arriving at 4559 m, but only at 44 hours afterward and after no further exercise. Furthermore, two studies by the same group (Majerczak et al., 2016, 2017) found no changes in circulating syndecan-1, heparan sulfate, or ICAM-1 concentrations after a progressive incremental exercise test to exhaustion in young subjects (age 22–23 years old). While our subjects were about a decade older, it is likely that their fitness and physical activity levels would be roughly equal to the subjects in the studies of Majerczak et al. (2016, 2017). Based on these data, we believe the exercise of climbing does not explain the changes in the glycocalyx markers but is a direct result of high-altitude hypoxia. Our syndecan-1 results differ as well from those of Johansson et al. (2014) who found that it rose after 2–4 hours of simulated hypobaric hypoxia of 4500 m, but in our study was only elevated after 44 hours.
To place the changes in syndecan-1, ICAM-1, and heparan sulfate observed by us and others with hypoxia and/or exercise in perspective, these are at most on the order of 30%–50%, while for trauma, sepsis, and ischemia/reperfusion injury in humans, the elevations in these conditions range from 50% to 1000% over baseline circulating blood concentrations (Weigand et al., 2001; Schmidt et al., 2012; van Golen et al., 2014; Rahbar et al., 2015; Andrews et al., 2016; Li and Ma, 2017; Holzmann et al., 2018; Kim et al., 2018; Hippensteel et al., 2019). In a study of a single patient with HAPE, with its much greater stress and injury on the pulmonary vasculature, Droma et al. (1996) found that ICAM-1 concentration in alveolar lavage fluid was doubled over that measured after recovery, but no blood concentrations were measured.
Our study was limited by the low number of subjects studied, making these data hypothesis generating. It would be useful to expand on these findings by studying changes in circulating glycocalyx constituents among more subjects, especially those who develop HAPE. Furthermore, the lack of direct markers of pulmonary vascular endothelial permeability limits our ability to theorize on the source of glycocalyx alteration (pulmonary vs. systemic vasculature); it would be interesting to correlate changes in circulating glycocalyx components with arterial blood gas analysis for quantification of the alveolar/arterial partial pressure of oxygen difference or evaluation of extravascular lung water through various imaging techniques. Measurements in patients with the greater vascular stress of HAPE will be informative as well, particularly as therapies aimed at glycocalyx preservation in sepsis and trauma, such as heparin, are proposed (Li and Ma, 2017).
Conclusion
High altitude induces hemodynamic changes leading to increased shear stress on the vascular endothelium, which may contribute to certain high-altitude disease manifestations. Our study demonstrates that plasma concentrations of glycocalyx components change over time after exposure to high altitude; furthermore, certain patterns of glycocalyx components appearing in the plasma such as an acute rise in heparan sulfate concentrations may correlate with the development of AMS and the rise in ICAM-1 with the increase in PAP and the development of peripheral edema. These data suggest that plasma markers of glycocalyx alteration may be a useful tool to evaluate the role of the vascular endothelium in disease states of high altitude.
Footnotes
Acknowledgments
The authors gratefully thank all the mountaineers who took part in the study and especially the excellent, reliable mountain guides from the Scuola die Alpinismo Corpo Guide Alagna Valsesia. They also thank the hut keepers, the Rifugi Monterosa, and the Sezione Varallo of the Club Alpino Italiano for providing an excellent accommodation and research facility at the Capanna Regina Margherita. They thank Simone Wurm (Department of Anesthesiology, Perioperative and General Critical Care Medicine, Salzburg General Hospital, Paracelsus Medical University, Austria), as well as Sonja Engelhardt and Christiane Herth (Department of Internal Medicine VII, Division of Sports Medicine, University Hospital Heidelberg, Germany) for their excellent technical assistance.
Author Contributions
K.E.S., M.M.B., P.S., L.M.S., H.M., and E.R.S.: Analysis and interpretation of data, drafting of article, and critical revision. M.M.B., M.S., F.M., and H.M.: Study conception and design. M.S. and F.M.: Drafting of article and critical revision. All authors have reviewed and approved of the article before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.