
Abstract
Introduction:
There is evidence that intermittent hypoxic exposure (IHE) may improve high altitude (HA) performance. In this study, the effects of short-term IHE through voluntary apnea training on HA-related symptoms, including acute mountain sickness (AMS), were examined for the first time.
Methods:
Forty healthy adults were randomized to a self-administered apnea training (n = 19) or control (n = 21 no apnea training) group before ascent to an altitude of 5100 m in the Himalayas over 14 days. The apnea training was conducted at sea level (SL) and consisted of five breath holds per day in week 1, seven in week 2, followed by 10 per day from weeks 3 to 6 and until HA exposure. Saturation of arterial oxygen (SpO2), heart rate, sleep quality (Insomnia Severity Index [ISI]), rating of perceived exertion (RPE), blood pressure, and Lake Louise scores were measured at SL (in the United Kingdom) and at HA at 1400, 2700, 3400–3700, 4050–4200, 4800, and 5100–5200 m. Anxiety (Generalized Anxiety Disorder-7 [GAD-7]) scores were examined at SL, 1400, and 5100–5200 m.
Results:
Apnea training led to a significant increase in the mean longest breath-hold times from baseline (80.42 ± 32.49 [median 87.00] seconds) to the end of week 6 (107.02 ± 43.65 [113.00] seconds), respectively (p = 0.009). There was no significant difference in the prevalence of AMS (8/19 = 42.1% vs. 11/21 = 52.4%; RR 0.80; 95% confidence interval 0.41–1.57: p = 0.80) or in GAD-7, ISI and RPE, SpO2, heart rate, or blood pressure among the apnea versus control groups, respectively, at HA.
Conclusions:
Apnea training does not lessen HA-related symptoms in healthy adults traveling up to 5200 m. Larger studies using more challenging apnea protocols and at higher altitudes should be considered.
Introduction
Recent improvements in infrastructure and access have led to significantly increasing numbers of persons traveling to high altitude (HA) compared with only a decade ago. HA-related symptoms, including anxiety, insomnia, and acute mountain sickness (AMS), are some of the commonest obstacles to success. AMS can rapidly worsen and lead to development of HA cerebral edema (HACE) and even death if it is unrecognized and not treated (Bartsch and Swenson, 2013; Boos et al., 2018). HA-related hypoxia can also cause HA pulmonary edema (HAPE), which is a noncardiogenic form of pulmonary edema resulting from excessive hypoxic pulmonary vasoconstriction, which can also be fatal if not recognized and treated promptly (Bartsch and Swenson, 2013). Unfortunately, despite intense research in the field, there are no reliable sea level (SL) predictors to identify individuals who are at a particularly high risk of developing AMS and its complications among a general population of otherwise healthy adults (Bartsch and Swenson, 2013; Lawrence and Reid, 2016; Masuet-Aumatell et al., 2017).
Consequently, there has been an increasing focus not only on methods to try to identify individuals at increased risk of HAPE and AMS but also to pre-emptively mitigate their risk prophylactically. There is emerging, yet inconsistent, evidence to suggest that intermittent hypoxic exposure (IHE) can improve exercise performance and induce a degree of preacclimatization (acclimation) that is associated with a reduction in the risk of AMS development and its severity (Muza, 2007; Wille et al., 2012; Fulco et al., 2013; Dehnert et al., 2014; Lizamore and Hamlin, 2017; Molano Franco et al., 2019). These studies have used either altitude chambers or low FiO2 breathing (hypoxicators) to replicate the hypoxia of genuine terrestrial HA. Both methods are expensive and logistically challenging to perform, thereby limiting their widespread utility. The mechanisms to explain their benefit appear to be multiple and are still poorly understood. Those cited include increased erythropoiesis, angiogenesis, and release of circulating stem cells, reducing oxidative stress and systemic inflammation, improved autonomic and mitochondrial function, chemosensitivity to hypoxia, and aerobic performance (Casas et al., 2000; Povea et al., 2005; Viscor et al., 2018; Gangwar et al., 2019). Its benefits appear to be heavily influenced by the population studied and the mode, frequency, and intensity of the hypoxic stimulus, as well as exercise components (Hamlin et al., 2018; Viscor et al., 2018).
Voluntary breath holding (apnea training) is another method of reproducing short-lived IHE, which has been used successfully for >25 years in free divers to enhance their performance (Bain et al., 2018). It has the obvious advantage over chamber-based IHE, in that there is no financial cost and it can be easily conducted in an individual's own time. There are published data to suggest its positive effects on both aerobic and anaerobic exercise performance (Lemaitre et al., 2010). However, its impact on HA-related symptoms and performance has not been explored. While the hypoxic period is far shorter with apneic training compared with conventional IHE, it has been shown to induce a variety of physiological changes that could be potentially utilized to the benefit of HA acclimation. These include increased splenic volumes and contraction and increased circulating hematocrit and hemoglobin concentrations to potentially improve the arterial oxygen content (Schagatay et al., 2001, 2005). Other published mechanisms include increased chemo-responsiveness, cerebral blood flow, and the bradycardic response to apnea (Bain et al., 2018). Together, these factors may act to improve hypoxic resilience and lessen myocardial oxygen consumption while maintaining cerebral oxygenation, which may be of translational benefit for HA acclimation (Schagatay et al., 2001; Costalat et al., 2014). Additional potential benefits include improved mindfulness and ventilatory control that may improve mood, anxiety, and sleep quality (Lemaitre et al., 2010; Cho et al., 2016). It has been demonstrated that apneic duration and the magnitude of associated bradycardia are linked to a lower risk of AMS, supporting the potential translational impact of apnea training in reducing HA-related illness (Austin and Sleigh, 1995; Holmstrom et al., 2019).
In this study, we aimed to investigate for the first time the effects of apnea training on HA-related symptoms. We hypothesized that apnea training offers a simple method of personal acclimation that leads to improved performance at HA and a reduction in the burden of AMS.
Methods
Population and design
This was a prospective, intention-to-treat observational study of 42 healthy adult male (n = 30) and female (n = 12) British military service volunteers who were due to take part in the RAF 100 Ex Himalayan Venture 18 to the Himalayas in September 2018. They were all low altitude dwellers without previous breath-hold training experience. The population consisted of two trekking teams (TTs) in the Khumbu Valley region of Nepal, undertaking an identical ascent and one Alpine Team (AT). The AT followed a marginally different ascent profile, but along a similar altitude and commencing in the Rolwaling Valley. The subjects were assessed at baseline (SL), 1400 m (day 1), 2700 m (day 2 for TTs and day 3 for AT), 3400–3700 m (day 3 for TTs and day 4 for AT), 4050–4200 m (day 5), and 4800–4900 m (day 7 for AT and day 8 for TTs). Rest days were scheduled where there was an altitude gain of ≥1000 m, hence days 3 and 6 for the TTs and days 6 and 8 for the AT. Thereafter, the sleep altitudes ranged from 4000 to 4996 m on days 9–14 before a further ascent to 5100–5200 m by both groups on day 14. None of the participants had been exposed to simulated or terrestrial HA in the preceding 6 weeks before inclusion.
The primary study outcome measure was development of AMS. Secondary outcome measures of interest were the comparative differences in heart rate, blood pressure, anxiety-related symptoms, sleep quality, peripheral saturation of arterial oxygen (SpO2), and rating of perceived exertion (RPE).
All participants were engaged in regular physical activity and had passed their service-specific fitness tests and were fully fit for military duty. A modified version of the Centre of Aviation Medicine (RAF Henlow) health questionnaire was used for health screening of participants before their inclusion.
Randomization and apnea protocol
The population of research volunteers was randomized to one of two research groups—a control group and an apnea group.
The apnea protocol was conducted at SL and consisted of five breath holds per day in week 1, seven in week 2, followed by 10 per day from weeks 3 to 6 and at least until their departure to HA. This protocol was designed following a previous study at HA (Mellor et al., 2017) and its demonstration of an induction in splenic contraction in a previous SL apnea study (Schagatay et al., 2005). The apnea protocol consisted of 2 minutes of calm and controlled breathing at a rate of 5–6 breaths/minute, followed by a deep, but not maximal, inspiration before each apnea. The apneas were conducted in a static sitting or lying position. The protocol mandated that apnea training be performed for 5 of 7 days each week. Participants in the apneic group were supplied with a breath-hold diary to record their longest breath-hold time and fingertip pulse oximeter to monitor their oxygen desaturation, during apneas, and were instructed to interrupt their breath hold if their SpO2 levels fell to ≤60% as previously described (Engan et al., 2013). They were instructed to document their lowest SpO2 readings for each day of apnea training while at SL. None of the participants in either group had received previous apnea training before this study.
Data collection and measurements
Baseline data were collected at effective SL (44 m) 70 days before departure. Thereafter, data collection was performed at 1400, 2700, 3400–3700, 4050–4200, 4800, and 5100–5200 m.
HA-related symptoms were recorded twice daily using the updated 2018 Lake Louise scoring (LLS) system (Roach et al., 2018). The total LLS score for an individual was calculated as the sum of the scores for four symptoms (headache, nausea/vomiting, fatigue, and dizziness/light-headedness). AMS was defined as a total score of at least three points, which included at least one score for headache at an altitude of ≥2000 m and a recent height gain (Roach et al., 2018). The subjects were advised not to take prophylactic acetazolamide. However, acetazolamide use was permitted under medical guidance (by the expedition doctor) for the treatment of AMS. The use of nonsteroidal anti-inflammatory medication and paracetamol was permitted and documented.
The Borg RPE was recorded at the end of each day (Borg, 1970). This is a 15-point numerical scale numbered from 6 to 20, with values of 6 representing the resting state and 20 representing exhaustive exercise that has been used at HA previously (Mellor et al., 2014). The highest RPE during the day was recorded to reflect the overall effort. The other physiological variables were recorded twice daily, prebreakfast and before the evening meal, and at least 3 hours after arrival at each new altitude. Blood pressure was measured on fully rested and seated subjects using a brachial cuff fitted to the dominant arm using the USCOM BP+ device (Uscom, Sydney, Australia). Resting SpO2 at HA was measured from the finger using a Nonin Onyx Series II pulse oximeter (Plymouth, MN).
Sleep quality was examined daily using the Insomnia Severity Index (ISI) prebreakfast, the night after arriving at each altitude (Bastien et al., 2001). This is a short-form questionnaire that was designed to assess the severity of both nighttime and daytime components of insomnia. The ISI is a seven-item self-report questionnaire assessing the nature, severity, and impact of insomnia. The dimensions evaluated were the severity of sleep onset, sleep maintenance, early morning awakening problems, sleep dissatisfaction, interference of sleep difficulties with daytime functioning, noticeability of sleep problems by others, and distress caused by sleep difficulties. A 5-point Likert scale was used to rate each item (e.g., 0 = no problem; 4 = very severe problem) to yield a total score ranging from 0 to 28. The total score was interpreted as follows: absence of insomnia (0–7); subthreshold insomnia (8–14); moderate insomnia (15–21); and severe insomnia (>21) as previously described (Bastien et al., 2001).
Anxiety levels were quantified using the Generalized Anxiety Disorder-7 (GAD-7) assessment questionnaire (Spitzer et al., 2006) at SL baseline and at 1400 m (day 1) and day 14 above 5000 m. It is a seven-item instrument that is used to measure or assess the severity of generalized anxiety disorder (GAD). Each item asks the individual to rate the severity of his or her symptoms over the past 2 weeks. The GAD-7 score is calculated by assigning scores of 0, 1, 2, and 3 to the response categories of “not at all,” “several days,” “more than half the days,” and “nearly every day,” respectively, and then adding together the scores for the seven questions, with the total score ranging from 0 to 21. Total scores were used to determine the severity of anxiety symptoms, which were graded as mild (score of 5–9), moderate (10–14), and severe (≥15) (Spitzer et al., 2006).
Ethics
The study was approved by the Ministry of Defence Research Ethics Committee and conducted according to the standards of the Declaration of Helsinki. All participants were required to provide written and informed consent before inclusion.
Sample size and power calculation
Our sample size was estimated from previously published work. Schagatay et al. (2005) demonstrated a significant (p < 0.001) and 18% reduction in splenic volume (due to splenic contraction) following three successive apneas among 10 healthy adults. Gangwar et al. (2019) demonstrated a significant reduction in AMS and higher SpO2 at HA among 40 healthy male adults randomized to IHE (n = 20; 12% FIO2 for 4 hours/day for four consecutive days) versus nontreatment (i.e., controls, n = 20). The participants were examined at SL and for seven consecutive days after being airlifted to 3520 m. We estimated that a similar sample size of at least 40 participants exposed to a longer period of self-administered IHE (6 weeks) and to higher altitudes (hence more AMS symptoms) would provide sufficient power to detect notable differences in LLS and AMS prevalence among those randomized to IHE versus no IHE (controls).
Statistical analysis
Data were analyzed using GraphPad Prism, version 6.07 (GraphPad Software, San Diego, CA; www.graphpad.com), and SPSS, version 22 (IBM®). Data inspection and the D'Agostino–Pearson normality test were undertaken to assess normality of all continuous data. Results are presented as mean ± standard deviation (SD). Categorical variables were compared using Fisher's exact and chi-squared tests with 95% confidence intervals (CIs). Independent two-group comparisons of continuous data were analyzed using an unpaired t-test and Mann–Whitney test for parametric and nonparametric data, respectively. Comparisons of continuous data from ≥3 groups of parametric and nonparametric data were performed using a one-way analysis of variance (ANOVA) and Kruskal–Wallis test, respectively. Correlation analyses were performed using Pearson correlation and Spearman's rank correlation with 95% CIs depending on data normality. Only correlations with an r > 0.20 were reported. A split-level factorial ANOVA was performed using SPSS to assess the main effects of apnea training (yes or no), change in altitude, and potential interaction on dependent outcomes. The normality of distribution, homogeneity of covariance matrices, and independence and sphericity assumptions were verified. Mauchly's test was used to check for sphericity. If the sphericity assumption was violated, the Greenhouse–Geisser correction was applied to adjust for the degrees of freedom of the interaction effect between different time points and different sample groups. If the value was <0.75, the Huynh–Feldt correction was used for repeated-measures analysis of variance. Binary logistic regression was performed to identify the baseline factors that were predictive of AMS at HA. A p-value of <0.05 was considered significant for all comparisons.
Results
From the initial inclusion of 42 participants, two people from the control group were excluded: one lost their data collection booklets on the mountain and the other participant failed to complete their data collection. Hence, the final analysis cohort consisted of 40 participants, which consisted of 19 in the apnea group and 21 in the control group. Among the apnea group, eight completed the entire protocol without any missed sessions. Eleven participants missed one or more apnea days as follows: ≤3 apnea days (n = 3), complete cessation after the first 3 weeks (n = 4), missing up to a week in the middle (n = 2), and 3 weeks at the end (n = 2).
The apnea and control groups were very similar in terms of age, sex, ethnicity, and other baseline demographics (Table 1). There was no difference in their baseline SpO2, heart rate, blood pressure, sleep, and GAD-7 scores (Table 1). Apnea training led to a significant improvement in longest breath-hold times from baseline (80.42 ± 32.49 [median 87.00] seconds) to the end of week 6 (107.02 ± 43.65 [median 113.00] seconds; p = 0.009). Their longest breath-hold time (134.94 ± 56.04 seconds) significantly increased compared with their baseline values (p = 0.0002).
Baseline Demographics
p Values refer to comparison of the control versus apnea group at inclusion.
HA exposure led to a significant increase in resting heart rate, systolic and diastolic blood pressure, LLS (Fig. 1), Borg, and GAD-7 scores and a reduction in SpO2 (Fig. 2) (Table 2). Of the 40 subjects, 28 had no significant anxiety symptoms (scores of 0–4) and symptoms were mild in 8 (score 5–9) and at least moderate in 4 (scores of ≥10) at day 14 (5100 m). There was no significant change in ISI scores.
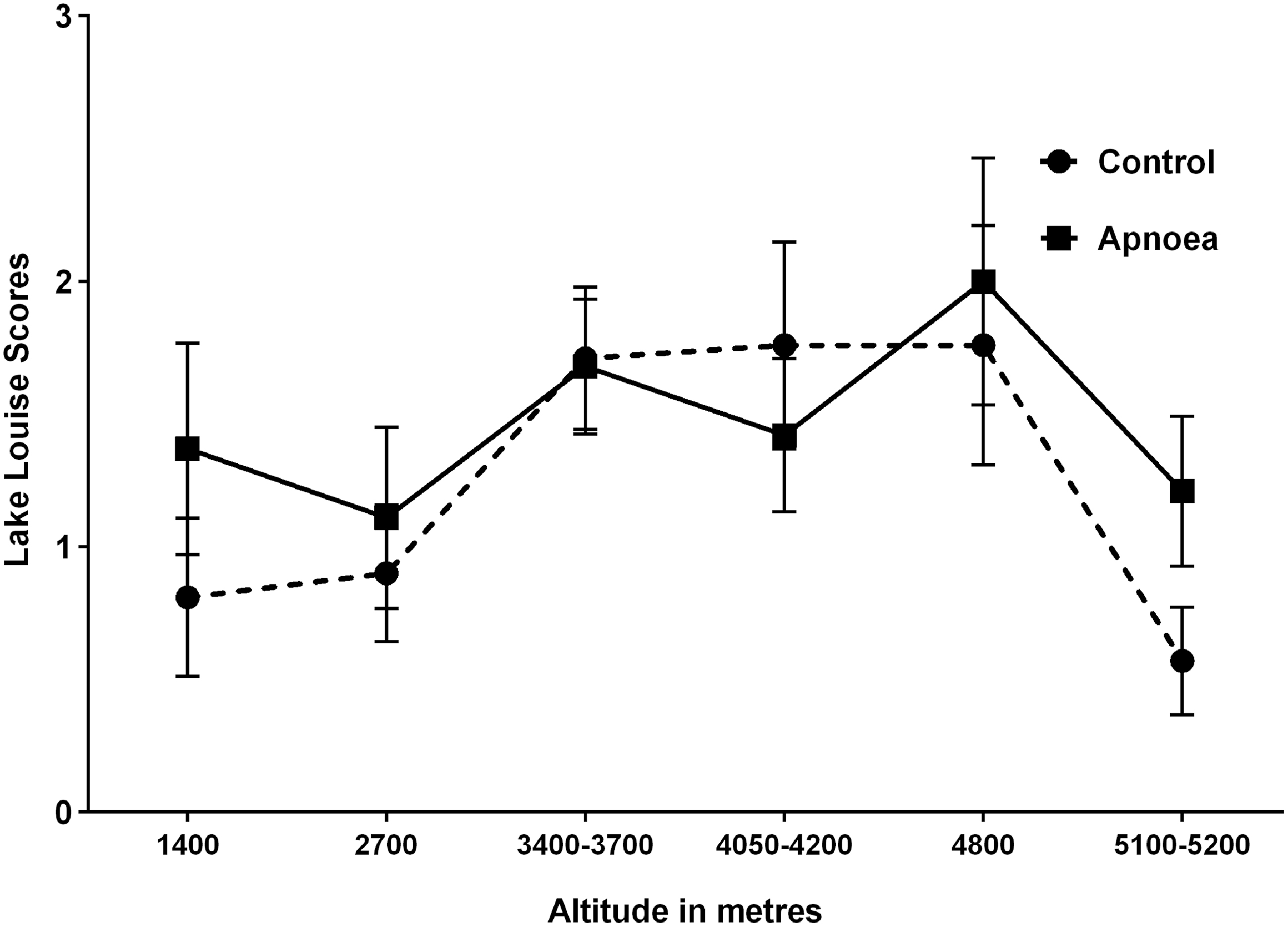
Comparative changes in Lake Louise scores (mean ± standard error of the mean) with increase in high altitude among the control versus apnea groups.

Comparative changes in SpO2 (mean ± standard error of the mean) with increase in high altitude among the control versus apnea groups. SpO2, arterial oxygen saturation.
Comparative Changes in Physiological Indices and Questionnaires with Increasing High Altitude
All measures above relate to those measured on the first morning at each altitude except Borg RPE scores, which were measured on the evening before; p values refer to overall group comparisons of marginal means for the apnea versus control groups.
GAD-7, Generalized Anxiety Disorder-7; RPE, rating of perceived exertion; SL, sea level; SpO2, saturation of arterial oxygen, %.
At HA, SpO2 inversely correlated with the heart rate (r = −0.21; 95% CI −0.30 to −0.12: p < 0.0001) and RPE (r = −0.60; −0.68 to −0.52: p < 0.0001). GAD-7 scores correlated with RPE (r = 0.29; 95% CI 0.06 to 0.48: p = 0.01) and ISI scores (r = 0.39; 0.18 to 0.56: p = 0.0004).
Overall, 19 (47.5%) participants experienced AMS at one or more altitudes ≥2000 m. There was no significant difference in the primary study outcome of AMS prevalence among the apnea group (8/19 = 42.1%) versus controls (11/21 = 52.4%; RR 0.80; 95% CI 0.41 to 1.57: p = 0.80). Eight participants from the apnea group and six from the control group were treated with acetazolamide (p = 0.75). None of the measured SL variables were predictive of AMS at HA. Four participants from the apnea group and four in the control group were treated with nonsteroidal medication and/or paracetamol (p = 1.0).
Apnea training (versus controls) also did not influence the secondary outcomes of GAD-7 scores (or prevalence of anxiety, GAD ≥5), ISI scores, RPE, or other physiological measures, including heart rate and SpO2. Furthermore, there was no evidence of an interaction of apnea training-x-altitude on any of the main outcome variables (Table 3).
Results of Split-Level Analysis of Variance on High Altitude Symptoms and Physiological Measures
All measures above relate to those measured on the first morning at each altitude except Borg scores, which were measured on the evening before.
Restricting our analyses to the eight participants who completed the full apnea training protocol revealed similar demographics to the control group. Among this apnea group of eight participants, the mean (±SD [range]) daily minimal SpO2 readings during apneas were significantly lower over week 6 (88.25% ± 8.85% [61%–98%]) versus week 1 (91.50% ± 6.65% [74%–99%]; p = 0.015). Conversely, their longest breath-hold times also significantly increased from baseline (mean 82.77 ± 34.96 [median 88.40] seconds) to the end of week 6 (109.58 ± 55.12 [107.40] seconds), respectively (overall ANOVA p = 0.009). On the split-level repeated-measures ANOVA, again there were no significant differences between this group (n = 8) versus the control group on any of the main study outcomes or in development of AMS.
Discussion
This is the first prospective randomized study to investigate the effects of apnea training on development of HA-related symptoms and AMS. In this study, apnea training was not associated with a reduction in AMS symptoms or severity. Apnea training did not improve sleep quality, anxiety levels, RPE, resting heart rate, brachial blood pressure, or SpO2.
The premise of this study was based on published evidence over the last 15 years supporting a role for IHE to augment exercise performance across a wide range of sporting disciplines (Czuba et al., 2017). There are also emerging data to suggest that IHE can induce acclimation effects, with the potential to reduce HA-related illness (Muza, 2007; Gangwar et al., 2019). This is an extremely exciting prospect given the enormous clinical burden of AMS, which is known to affect >40% of all persons traveling above 3500 m (Bartsch and Swenson, 2013; Boos et al., 2018). AMS remains the most common medical condition encountered at HA and can rapidly progress to HACE and even death (Bartsch and Swenson, 2013). The underlying concept behind IHE is its utility to induce hypoxic preconditioning and lessen the deleterious effects of hypoxia. Despite its promise, the published data are inconsistent. This may, in part, relate to the marked heterogeneity in IHE protocols used in these studies. They have varied widely in terms of the hypoxic mode used (normobaric versus hypobaric hypoxia versus voluntary apnea), its severity, duration (seconds to hours), and the number of cycles used (Muza, 2007; Hamlin et al., 2018; Gangwar et al., 2019).
In our study, we investigated whether apneic training, using voluntary breath holds, can deliver effective IHE and translate into better acclimatization at HA and lessen HA-related symptoms (including AMS). Apneic training is proven to be effective in terms of improving free diving performance with some data to support its additional role in enhancing normoxic (i.e., SL) athletic performance (Lemaitre et al., 2010; Bain et al., 2018). The cited mechanisms for its performance-enhancing effects include reducing blood acidosis, oxidative stress, basal metabolic and heart rate, increasing erythropoietin concentration and reticulocyte counts, enhanced splenic volume and contraction, lung volumes, and anaerobic glycolysis activity, as well improving cerebral blood flow, autonomic control, and heart rate variability (Joulia et al., 2002; Lemaitre et al., 2010; Christoforidi et al., 2012; Engan et al., 2013; Inoue et al., 2013).
Our desire to investigate the impact of apneic IHE on sleep and anxiety stems from our own previous work and that of others (Dong et al., 2013; Boos et al., 2018). We have recently observed that anxiety symptoms were independent predictors of AMS and its severity among a cohort of 80 healthy adults trekking to 5140 m (Boos et al., 2018). Anxiety-related symptoms are frequently exacerbated at HA and strongly linked to both somatic symptoms and sleep quality (Dong et al., 2013). Indeed, we observed a significant increase in anxiety scores at HA versus SL in this study. There was significant, although modest, correlation between GAD-7 anxiety and ISI scores. Unfortunately, apneic training did not improve either of these scores. We had hypothesized that the controlled breathing, which was integral to the apneic warm up, might have led to a degree of mindfulness and relaxation training that could have improved anxiety and sleep scores. It is worth noting that in this study, the impact of HA on sleep quality was marginal and less than what we might have anticipated, which could reflect the gradual ascent profile used.
There are many plausible reasons to explain the negative results of this study. Compliance with the apnea protocol was poor and this, in itself, could have been sufficient to explain the lack of observed benefits. In our protocol, apnea training was conducted in 5 of 7 days in the week. Hence, the two rest days could have mitigated any acclimation effects. Consequently, we do not know whether a more intense apnea protocol without rest days might have led to different results. Voluntary breath holding is uncomfortable and requires significant motivation. We did not include any encouragement methods to maintain compliance, which is a limitation (van der Zwan et al., 2015). Another consideration is that the apnea intensity was perhaps insufficient to achieve a decent hypoxic stimulus. In a very recently published study, Bouten et al. observed that while 8 weeks of apneic training (five apneas per day and similar to our protocol) led to an increase in splenic volume, it was not sufficient to elicit significant training acclimation (Bouten et al., 2019). The mean daily lowest SpO2 recordings during week 6 of apneic training at SL, in our study, were certainly not insignificant at 88.25%. In fact, this is very similar to the average resting SpO2 recorded at 3400–3700 m, but may still be an insufficient stimulus.
Another factor that needs consideration regarding the modest hypoxia with breath-hold training in this study is the limitations of peripheral pulse oximetry itself. We used finger rather than central (e.g., earlobe) pulse oximetry to record SpO2 during breath holds because of its ease of use, widespread use, and to maintain consistency with SpO2 readings at HA. However, there is a well-recognized time delay between the quantification of central hypoxia and its manifestation on peripheral pulse oximetry SpO2 readings (Lindholm et al., 2007; Pertzov et al., 2019). This can lead to significant differences in simultaneously measured central oximetry readings, which are reported to be ≥6% lower with ear lobe versus finger readings (Lindholm et al., 2007). These differences may be even greater when the onset of hypoxia is rapid such as with breath holding as in this study. Hence, it is possible that we have underappreciated the severity of induced hypoxia with apnea training in this study.
The hypoxic period in the majority of IHE studies (using normobaric or hypobaric hypoxic training) has generally been well in excess of 30 minutes for each training session and far longer than the apneic period of <5 minutes obtained in our study (Lizamore and Hamlin, 2017; Gangwar et al., 2019). Perhaps the potential hypoxic preconditioning effects of apnea training are too short-lived to induce a noticeable, sustained preacclimatization effect (Richardson et al., 2009). Hypoxia is common to apneic training, IHE, and HA exposure. However, with apnea, there is compensatory hypercapneic hypoxia, whereas with IHE and genuine HA, hypocapneic hyperventilation ensues; this leads to a progressive rise in end-tidal O2 and subsequent fall in end-tidal CO2, which is crucial to HA acclimatization (West et al., 2012; Lizamore and Hamlin, 2017). Hence, it is plausible that apnea training may not increase chemoreceptor and carotid body sensitivity noted with traditional IHE, undermining some of its acclimation potential.
This study has a number of strengths that should be acknowledged. This was a prospective and randomized study conducted at both SL and HA. Our sample size was larger than the majority of previously published apneic studies (Richardson et al., 2009; Christoforidi et al., 2012; Engan et al., 2013; Bouten et al., 2019). Our study power was considerably strengthened by the fact that participants were investigated at seven different altitudes across a wide range of physiological and wellness outcomes (GAD-7 [anxiety], ISI [sleep quality], RPE [perceived exertion], and LLS [AMS symptoms]).
Limitations
The poor compliance rate with the apnea protocol is a major limiting factor that needs to be reemphasized, although the absence of benefit among those who completed the full apneic protocol strengthens the validity of our results. While the overall altitudes and time of trekking were similar between the three groups studied, one of the groups (with a similar proportion randomized to apnea and nonapnea subjects) had a slightly different ascent profile and resided at a higher altitude for a longer period. We did not examine comparative hemoglobin and erythropoietin levels to gauge the degree of successful hypoxic preconditioning with breath-hold training. While the longest breath-hold duration significantly increased with apnea training, the average breath-hold duration was relatively short, again suggesting poor compliance with the protocol. Only the lowest SpO2 readings during apnea were recorded. Finally, the ascent rate in this study was modest, particularly between 4800 and 5200 m. This may have contributed to the relatively low incidence of AMS and limited the potential impact of breath-hold training on HA-related symptoms.
Conclusions
In this study, IHE using voluntary breath holds did not reduce the burden and severity of AMS. Breath-hold training also failed to provide any comparative advantages in terms of lessening the impact of HA exposure on sleep quality, anxiety scores, RPE during exercise, heart rate, and blood pressure over traditional non-IHE preparation. A larger study with a more aggressive protocol using compliance encouragement methods should be considered.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.