
Abstract
Background:
Osteogenic responses induced by training under hypoxia remain unclear. We aimed to investigate whether intermittent hypoxic resistance training affects osteogenic responses.
Materials and Methods:
Sixteen male participants underwent resistance training under normoxia (NRT; n = 7) or hypoxia (HRT; O2 = 14.4%, n = 9), twice a week for 8 weeks. The HRT group exercised and rested for 30 minutes under hypoxia, with total hypoxic exposure time in one session of ∼60 minutes. At pre- and postexperiment, bone mineral density (BMD) of the whole body and right proximal femur was measured. At the first and last training sessions, bone alkaline phosphatase (BAP), osteocalcin (OC), cross-linked N-telopeptide of type I collagen (NTx), type I collagen cross-linked C-telopeptide (ICTP), interleukin-6 (IL-6), and blood lactate (La) concentration were analyzed at rest and postexercise.
Results:
BMD did not change with training and hypoxia. Although BAP, OC, and ICTP levels at rest significantly increased with training (p < 0.01, 0.05, and 0.05, respectively), they did not change with hypoxia. NTx and IL-6 did not change. Additionally, changing patterns of bone markers and La induced by a single bout of exercise were similar among groups in both training sessions.
Conclusions:
Short-term resistance training enhanced overall bone metabolism, regardless of the oxygen level. Hypoxia has no effects on osteogenic responses.
Introduction
It is widely known that physical training is very important for bone health and that it significantly increases bone mineral density (BMD) (Guadalupe-Grau et al., 2009). High- or odd-impact exercises, such as volleyball, jump exercise, and soccer, effectively increased BMD or bone strength, whereas low or nonimpact exercises, such as swimming and cycling, had no or less effect on bones (Nikander et al., 2010; Honda et al., 2015). However, it will take several months, probably at least 4 to 6 months, to observe obvious quantitative bone changes by physical training in humans. Therefore, there are only a few studies investigating the effects of short-term physical training on osteogenic responses that are focused on BMD.
Conversely, changes in bone markers are observed in the relatively early stages after training (Fujimura et al., 1997; Woitge et al., 1998; Evans et al., 2008; Lester et al., 2009; Banfi et al., 2010; Maïmoun and Sultan, 2011). In addition, bone markers have been shown to change with a single bout of exercise (Ashizawa et al., 1998; Whipple et al., 2004; Hermann et al., 2007; Banfi et al., 2010; Maïmoun and Sultan, 2011; Rogers et al., 2011; Mezil et al., 2015). However, because many factors, such as exercise type, intensity, time, blood sampling time, age, sex, training status, and so on, were included, results were inconclusive (Banfi et al., 2010; Maïmoun and Sultan, 2011).
As for changes in bone markers with short- to long-term training interventions, Maïmoun and Sultan (2011) reported that anaerobic and resistance training induced an overall acceleration in bone markers or increase in bone formation markers associated with a decrease or no change in bone resorption markers at rest. Meanwhile, in studies investigating the effects of a single bout of exercise on bone markers, results were prominently different depending on exercise types, intensities, and blood sampling points (Ashizawa et al., 1998; Whipple et al., 2004; Hermann et al., 2007; Banfi et al., 2010; Maïmoun and Sultan, 2011; Rogers et al., 2011; Mezil et al., 2015). Although there were wide discrepancies in the changing patterns among studies, the tendency that formation markers decrease and resorption markers increase with a single bout of exercise has been reported (Banfi et al., 2010).
Recently, the effects of intermittent resistance training under hypoxia on strength, muscle size, or physiological responses have been investigated (Kon et al., 2010; Scott et al., 2014; Feriche et al., 2017). However, to our knowledge, there are no studies that focused on osteogenic responses induced by physical training under hypoxic conditions in humans. Hypoxia impairs osteoblast differentiation or bone formation and promotes osteoclast formation or bone resorption ex vivo (Arnett, 2010). Furthermore, acidosis also impedes bone formation and promotes bone resorption (Frick et al., 1997; Arnett, 2010; Kato and Morita, 2013). We have previously reported greater accumulation of blood lactate (La) by resistance training under hypoxia compared with that under normoxia (Kon et al., 2010).
Therefore, we speculated that a greater impact of hypoxia and lactic acidosis would be observed with resistance training under hypoxia compared with normoxic conditions, that is, a decline of bone formation markers or increase of bone resorption markers would be noted. In this study, we hypothesized that intermittent hypoxic resistance training would negatively affect osteogenic responses, especially bone biomarkers. The purpose of this study was to investigate this hypothesis in healthy men who underwent short-term resistance training under hypoxia.
Materials and Methods
Participants
Participants were 16 healthy men living at sea level. They were randomly divided into the following two groups: normoxic resistance training group (NRT, n = 7) and hypoxic resistance training group (HRT, n = 9). Six participants had light to moderate exercise habit; of these, three participants were categorized into the NRT and the remaining participants into the HRT. None of the participants were smokers; were taking medicines and supplements; had injuries, fractures, and other diseases within 6 months; and were exposed to hypoxia within 1 month before the experiment. The experiment was conducted between September and December.
This study was approved by the Ethics Committee of Japan Institute of Sports Sciences. Informed consent was obtained from all participants before their participation.
Measurements of body composition, BMD, and exercise performance
At the pre- and postexercise interventions, one-repetition maximum (1RM) values in leg and bench press were measured. Similarly, percent body fat, lean body weight, and BMD of the whole body and right proximal femur were measured by dual-energy X-ray absorptiometry (DXA, QDR-4500A; Hologic, Bedford, MA). Measurements of BMD and body composition were performed through standard procedures by three professional technicians in our laboratory.
Resistance training program
Participants performed bench and leg press, respectively, 10 times for 5 sets, at 70% 1RM between 90-second intervals, 2 times per week for 8 weeks. A total of 16 training sessions were set, with one training session requiring ∼20 minutes. When the participants completed 10 repetitions for 5 sets without help, 2.5 kg for bench press and 5 kg for leg press were added in the next training session. Additionally, every 2 weeks, each 1RM was rechecked, and load intensity was adjusted.
The participants in the HRT exercised in a normobaric hypoxic training room (O2 = 14.4%, 3000 m). First, they rested for 5 minutes, and the oxygen saturation level (SpO2) in the hypoxic training room was monitored. Then, they started doing the warm-up (stretching or low-intensity main exercise) and main exercises. After the exercise, they stayed and rested in the hypoxic training room for 30 minutes. Thus, participants in the HRT were exposed to hypoxic conditions for ∼60 minutes in each session. NRT performed the same protocol in the normoxic condition without resting after exercise. SpO2 was monitored using a pulse oximeter (oxygen saturation monitor; Pulsox-300i, Konica Minolta Co., Japan).
Bone biomarkers, La, and SpO2
At the first and 16th training sessions, blood samples were obtained from the antecubital vein. The first rest sampling (R1) was taken under normoxic conditions in all participants. Other samplings were taken under the respective training condition. The second rest sampling (R2) was drawn after 15 minutes of entering the hypoxic room for HRT or 15 minutes after R1 for NRT. Blood samplings immediately after exercise (P0) and 30 and 60 minutes later (P30 and P60, respectively) were also conducted. All blood samples were obtained in the morning after an overnight fast. Blood samplings in the 16th training session were conducted at least 2 days after the previous training day. Blood samples at R1 were also used as baseline data at the pre- and postexercise interventions.
Serum bone alkaline phosphatase (BAP) and osteocalcin (OC) levels were measured as bone formation markers, and serum cross-linked N-telopeptide of type I collagen (NTx), type I collagen cross-linked C-telopeptide (ICTP), and plasma interleukin-6 (IL-6) were evaluated as bone resorption markers. BAP and IL-6 were measured by using the chemiluminescent enzyme immunoassay kit (Access Ostase; Beckman Coulter, Inc., CA, and QuantiGlo Elisa Human IL-6 Immunoassay; R&D Systems, Inc., Minneapolis, MN, respectively), OC by immune radio metric assay (BGP IRMA Mitsubishi; Mitsubishi Kagaku Medience, Tokyo, Japan), NTx by enzyme immunoassay (Osteomark NTx Serum; Alere Medical Co., Ltd., Chicago, IL), and ICTP by radio immunoassay (Pyridinoline ICTP; Orion Diagnostica, Espoo, Finland). Analysis of IL-6 was done only at R1. The intra-assay coefficient of variance was <10% in BAP, OC, and IL-6 and <15% in ICTP and NTx. Blood samples were centrifuged for 10 minutes (room temperature, 3000 rpm) and then separated and stored at −80°C until analysis.
Blood sampling from the fingertip was also performed to measure La using a lactate analyzer (Lactate Pro; Arkray, Inc., Kyoto, Japan). To estimate the maximal La level (Lamax), La measurements were added at 3, 5, and 10 minutes after the exercise as well as the usual blood samplings, and the highest value was termed as Lamax. In addition, SpO2 levels were also monitored and checked at the same point during and after exercise.
Statistical analysis
Data are presented as mean ± standard deviation. Repeated two-way (training or time × group) ANOVA was used to examine each main effect and interaction using IBM SPSS Statistics 19.0. If a significant interaction or main effect was found, post hoc analysis was performed using Bonferroni correction. The significance level was set at p < 0.05.
Results
Physical characteristics and exercise performance
The physical characteristics, BMD, and 1RM are shown in Table 1. Body weight and lean body weight were significantly increased (p < 0.05 and p < 0.01, respectively), whereas body fat did not change with training; thus, percent body fat reduced (p < 0.05) at postexperiment. The 1RM value of leg and bench press significantly increased with training (p < 0.01). The BMD of all sites did not change with training, although the BMD of whole body and proximal femur was significantly higher in HRT than in NRT throughout the experimental period (p < 0.05 and p < 0.01, respectively). Conversely, significant interactions were not found in all these parameters, and there were no effects of hypoxia on these changes.
Physical Characteristics, Bone Mineral Density, and One-Repetition Maximum at Pre- and Post-Training
Data are means ± SDs.
p < 0.01.
p < 0.05.
% Fat, percent body fat; 1RM, one-repetition maximum; BMD, bone mineral density; HRT, hypoxic resistance training group (n = 9); LBW, lean body weight; NRT, normoxic resistance training group (n = 7); NS, not significant; SD, standard deviation.
Changes in bone biomarker levels at baseline
The alterations in bone biomarkers at R1 are shown in Table 2. In the last training session, one participant in the HRT had extra high IL-6 values (31.8 pg/mL). According to the result of Smirnov–Grubbs' outlier test, we excluded this participant's IL-6 data in the statistical analysis. There were no significant interactions in all parameters, and hypoxia did not affect bone metabolism. Conversely, significant training main effects were found on BAP, OC, and ICTP (p < 0.01, p < 0.05, and p < 0.05, respectively). These parameters in both groups significantly increased with training. However, NTx and IL-6 did not change with training. A significant group main effect was found in OC and NTx, and these parameters were significantly higher in HRT than in NRT throughout the experimental period (p < 0.05).
Alterations of Bone Biomarkers at Baseline
Data are means ± SDs.
p < 0.01.
p < 0.05.
BAP, bone alkaline phosphatase; HRT, hypoxic resistance training group (n = 9, except for IL-6. n = 8, on IL-6); ICTP, type I collagen cross-linked C-telopeptide; IL-6, interleukin-6; NRT, normoxic resistance training group (n = 7); NTx, cross-linked N-telopeptide of type I collagen; OC, osteocalcin.
Changes in bone biomarkers, La, and SpO2 levels with a single bout of exercise
The changes in bone markers with a single bout of exercise are shown Figure 1. Statistically significant interactions were not found in all bone markers, and hypoxia did not affect the bone marker changes. In BAP, there were significant time main effects in both the 1st and 16th training sessions (respectively, p < 0.01). In both training sessions, BAP significantly increased with exercise (p < 0.01) and returned to the rest levels at 30 minutes after exercise. In addition, BAP was significantly higher at P0 than at R2 (p < 0.01). Regarding OC, significant time main effect (p < 0.01) and group main effect (p < 0.05) were found in the first training session. The OC level significantly decreased at P0 than at R1 and R2 (p < 0.05) and returned to rest levels at P30. In addition, the OC level was significantly higher in HRT than in NRT. Conversely, in the 16th training session, only a significant time main effect (p < 0.05) was found, which was significantly decreased at P0 than at R2. Although there was a tendency of interaction, it was not statistically significant (p = 0.06). As to ICTP, there were significant time main effects in both training sessions (p < 0.01). ICTP at P0 was significantly higher in the 1st (p < 0.01) and 16th training sessions (p < 0.05) than ICTP at R1 and returned to rest levels at P30. Similarly, ICTP was significantly higher at P0 than at R2 in both training sessions (p < 0.01). As for NTx, although there were no significant main effects in the first training session, a significant time main effect was found in the last training session (p < 0.01). NTx levels at R2, P0, and P30 were significantly lower than that at R1 (p < 0.05, p < 0.01, and p < 0.05, respectively) and that at P0 was significantly lower than that at R2 (p < 0.05).

Changes in bone biomarkers with a single bout of exercise. The shaded areas represent exercise time. Data are mean ± SD. There were significant time main effects in BAP, OC, and ICTP in both training sessions and NTx in 16th training session. In the first training session, a significant group main effect was indicated in OC. Significant time × group interactions were not indicated. †p < 0.05 and ††p < 0.01, significant time or group main effect. *p < 0.05 and **p < 0.01 versus R1. #p < 0.05 and ##p < 0.01 versus R2. BAP, bone alkaline phosphatase; HRT, hypoxic resistance training group (n = 9); ICTP, type I collagen cross-linked C-telopeptide; NRT, normoxic resistance training group (n = 7); NTx, cross-linked N-telopeptide of type I collagen; OC, osteocalcin; SD, standard deviation.
The La changes are shown in Figure 2. Because one participant in the HRT had a blood sampling error during the first training session, this participant's data were excluded in the statistical analysis for La. In both sessions, there were significant time main effects (p < 0.01). La significantly increased with exercise (p < 0.01) and remained significantly high until after 60 minutes of exercise (p < 0.01). Lamax at the first training session was 12.3 ± 2.8 mmol/L and 13.4 ± 1.4 mmol/L in NRT and HRT, respectively, and at the 16th training session, it was 13.2 ± 1.8 and 13.5 ± 2.5 mmol/L, respectively. There were no significant interactions and main effects. Hypoxia did not affect the La and Lamax changes. The SpO2 level was significantly lower in HRT than in NRT in both training sessions, except for that at R1. Detailed data were shown in our series study (Kon et al., 2014).
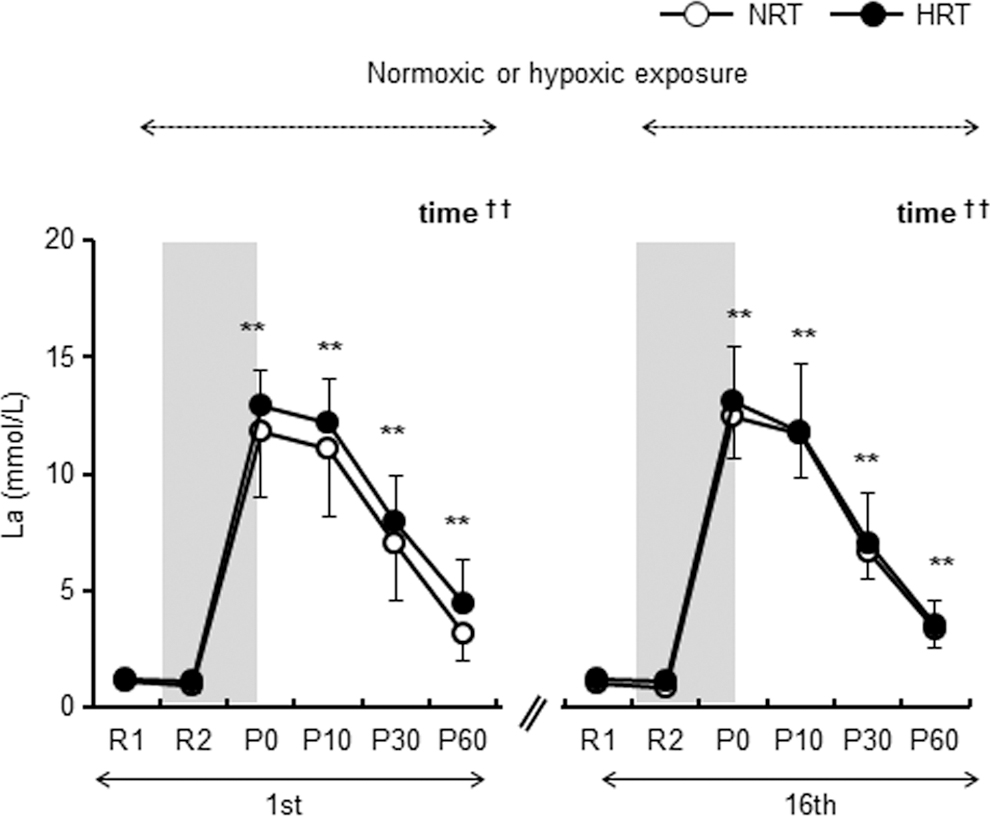
Changes in blood lactate levels with a single bout of exercise. NRT (n = 7) and HRT (n = 8). Data are mean ± SD. The shaded areas represent exercise time. Significant time main effects were indicated in both training sessions. There were no significant group main effects and interactions. ††p < 0.01, significant time main effect. **p < 0.01 versus R1.
Discussion
In this study, we showed that short-term and limited resistance exercise enhanced overall bone metabolism with mainly increases of bone formation markers, regardless of the oxygen level. However, we could not find any effects of hypoxia on bone mass and bone markers, that is, changes in osteogenic responses were similar in both HRT and NRT. Therefore, our hypothesis that intermittent hypoxic resistance training negatively affects bone metabolism in sea level residents was not supported.
Hypoxia and metabolic acidosis had a stimulatory influence on bone resorption and a negative effect on bone formation in ex vivo studies (Frick et al., 1997; Arnett, 2010; Kato and Morita, 2013). Based on our previous study (Kon et al., 2010), we thought that severe lactic acidosis might be observed in HRT than in NRT. Therefore, we hypothesized that the negative effects of bone marker changes during acute exercises or at postexercise interventions might be observed in HRT. However, contrary to our speculation, similar levels and changing patterns of La were observed in both groups. The Lamax value was high and at a similar level (range: 8.0–16.6 mmol/L in NRT and 8.7–16.1 mmol/L in HRT) and, even at P30, the mean La level was maintained at 6.7–8.0 mmol/L in both groups. Although we did not measure the blood pH level, we were convinced of metabolic acidosis during and after exercise, considering the La level. Thus, more severe lactic acidosis induced by hypoxic training compared with normoxia was not shown. In fact, we monitored SpO2 during exercise and checked the hypoxic condition in HRT. The effects of hypoxia on bone markers might be masked by severe acidosis, as observed in NRT as well. The hypothesis that exercise-induced lactic acidosis increases bone resorption markers and reduces formation markers was examined by Hermann et al. (2007). By cycling at the 110% anaerobic threshold for 60 minutes, a significant pH decline due to increase in La (mean value was ∼8–9 mmol/L) was observed. However, significant increases in BAP, OC, and CTx and no changes in tartrate-resistant acid phosphatase (TRAP) were observed. They also could not support their hypothesis. The level of pH (∼7.30–7.35) in their study would not be enough to be considered as acidosis. They suggested that prolonged, severe exercise-induced acidosis was needed to elicit significant changes in bone resorption activity. In this study, although more severe acidosis was induced by our intervention, compared with that of Hermann's study, it did not inhibit bone formation or stimulate bone resorption activity. Therefore, we speculated that the exercise itself would have a great advantage in terms of bone metabolism and removing the negative effects of hypoxia or acidosis.
We could show the time course changes with prolonged or acute exercise in bone markers. Many studies reported that bone metabolism changed with 4 to 8 weeks of physical training (Fujimura et al., 1997; Woitge et al., 1998; Evans et al., 2008; Lester et al., 2009; Banfi et al., 2010; Maïmounet and Sultan, 2011). According to their studies, a short-term exercise intervention had a tendency to increase bone formation markers such as BAP and OC and decrease or maintain bone resorption markers, such as TRAP, CTx, and IL-6. Additionally, it was reported that athletes showed higher values of bone formation markers or overall acceleration in bone markers than their nonexercised counterparts (Maïmoun and Sultan, 2011). Taken together, exercise intervention appears to have a benefit on bone formation, although depending on exercise type, intensity, period, and so on. In our training program, the participants performed only leg and bench press (exercise time was only 20 minutes) twice a week for 8 weeks. Various kinds of contents (squat, bench press, leg extension, abdominal works, and so on), 3 or more times per week, over 30 minutes, and more prolonged intervention periods were generally provided in a resistance training program. To our knowledge, our training program had the lowest training volume. However, our data suggested that this limited and minimal training program also had benefits for stimulating bone formation.
Regarding the effects of a single bout of exercise on bone markers, we observed significant increases in BAP and ICTP and decreases in OC at only immediately after exercise. Some previous studies showed significant changes of bone markers at longer sampling points, for example, after 1 to 48 hours (Whipple et al., 2004; Hermann et al., 2007; Kish et al., 2015; Mezil et al., 2015). In this study, despite negligible changes in bone markers induced by acute exercise, in the long term, these changes led to the enhancement of overall bone metabolism. On the other hand, NTx did not change with training in the first training session, it significantly decreased after the last training session. The reason why secretion of NTx changed after the training intervention was not clear, but we considered that to still be an interesting result. Additionally, regarding OC changes, a significant group main effect was found in the first training session, and this difference disappeared in the 16th training session. In the 16th training session, there was a statistical tendency for time × group interaction (p = 0.06). Therefore, if the experiment period or hypoxic exposure time would be prolonged, the hypoxic effect on bone metabolism might be indicated.
A few studies showed an increase in BMD with physical training of ∼2 months (Lester et al., 2009; Gaffney-Stomberg et al., 2014; Ravnholt et al., 2018). However, the possibility of measurement error by repeated imaging because of significant, but quite small, changes using DXA and peripheral quantitative computed tomography (pQCT) was suggested (Lester et al., 2009). In this study, although we observed enhancement of bone formation markers, the BMD at all sites did not change in both groups. Meanwhile, it will take at least 4 to 6 months to observe obvious bone quantitative changes with physical training, according to the review by Guadalupe-Grau et al. (2009). Therefore, our data were expected results and supported the review by Guadalupe-Grau et al. that observing changes in bone quantities by short-term training is difficult. However, if we could perform a detailed analysis using pQCT, different results might be shown in this study.
Our study had several limitations. First, the time and period of hypoxic exposure would be too short to observe the effects and differences in bone metabolism. A previous study reported significant decreases of BAP and calcitonin and significant increases of parathormone and vitamin D after 4 months of staying at extreme altitudes (Basu et al., 2013). It was suggested that prolonged, extreme hypoxic exposure had negative effects on bone metabolism. However, we do not know the duration or level of hypoxic exposure (altitude) that could have an influence on osteogenic responses with exercise because of the lack of available data and studies in humans. Second, although we chose resistance training as a beneficial training type for bones, other types of training or lower intensity resistance training programs compared with the current program would be suitable for investigating osteogenic responses under hypoxia. Our training program might be too strenuous, taking into consideration the La level. Finally, it was recommended that the bone markers be monitored for at least 24 hours after training (Whipple et al., 2004). If we could measure at another point, such as several hours or days after exercise, different results might be observed. Meanwhile, to the best of our knowledge, we are the first to investigate the effects of hypoxic exposure on osteogenic responses with a single bout of exercise or training intervention in humans. Further investigations improving the abovementioned problems or involving a large sample size are required.
Conclusions
Our results demonstrated that short-term resistance exercise enhanced bone metabolism, especially bone formation, although BMD did not change. However, the changing patterns of bone turnover markers at rest and during exercise were similar in both hypoxic and normoxic conditions. These results indicated that intermittent hypoxic resistance training did not affect the osteogenic responses in sea level residents.
Footnotes
Authors' Contributions
A.H. was involved in study design, data collection, data analysis, and drafting of the manuscript. M.K. and T.M. were involved in study design, data collection, and the experimental work. Y.S. was involved in study concept and design, data interpretation, and manuscript preparation.
All authors agreed to be accountable for this research work and have approved the final version of the manuscript.
Acknowledgments
The authors are grateful to all the participants, members of the hypoxic project, and staff at the Japan Institute of Sports Sciences (JISS). The authors also thank Noriyuki Tawara for operating the DXA scan and for helping in the data analysis of BMD.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.