To study the criterion validity of three indirect maximal oxygen uptake (O2max) assessment equations at altitude.
Methods:
We studied 64 young adults (53% men) at Bogota, Colombia (2600 m altitude). Direct O2max was measured by indirect calorimetry using a maximal incremental treadmill protocol. Indirect O2max was estimated by two exercise field tests (the 20-m shuttle-run test [20-MST] and the 2-km walking test (UKK)) and one nonexercise method (the perceived functional ability–physical activity rating questionnaire [PFA-PAR]). Altitude-adjusted PFA-PAR was estimated as a 13% linear reduction in PFA-PAR. We calculated Lin concordance coefficients (LCC) and standard error of the estimates (SEEs), and we performed Bland-Altman analyses for each indirect method.
Results:
Mean O2max was 41.2 ± 5.8 mL/kg/min in men and 32.2 ± 3.6 mL/kg/min in women. We found the highest agreement with direct O2max for the 20-MST (LCC = 0.79, SEE = 3.91 mL/kg/min), followed in order by the altitude-adjusted PFA-PAR (LCC = 0.71, SEE = 4.12 mL/kg/min), the UKK (LCC = 0.67, SEE = 5.48 mL/kg/min), and the unadjusted PFA-PAR (LCC = 0.57, SEE = 4.75 mL/kg/min). The unadjusted PFA-PAR tended to overestimate O2max, but Bland-Altman analysis showed that this bias disappeared after altitude adjustment.
Conclusion:
Several maximal, submaximal, and nonexercise methods provide estimates of O2max with acceptable validity for use in epidemiological studies of populations living at moderate altitude.
Introduction
Cardiorespiratory fitness (CRF), the measure of an individual's functional ability, has been fully recognized as an independent predictor of all-cause and cardiovascular mortality (Blair et al., 1989, 1996; Kodama et al., 2009), even more powerful than other traditional cardiovascular risk factors (Myers et al., 2002; Katzmarzyk et al., 2005; Blair, 2009). Moreover, CRF has been inversely associated with the risk of developing type 2 diabetes mellitus (Sui et al., 2008; Lee et al., 2009) and dying from cancer (Schmid and Leitzmann, 2015).
Accordingly, the assessment of CRF at both patient (Ross et al., 2016) and population level (Sanders and Duncan, 2006; Kaminsky et al., 2013, 2017; Laukkanen et al., 2016) is increasingly recognized as a part of worldwide efforts to understand, characterize, classify, follow up, and mitigate health risks. Maximal oxygen uptake (O2max) is the accepted criterion measure of CRF (Howley et al., 1995; Bassett and Howley, 1997). Although direct measurement of O2max by respiratory, breath-by-breath, gas exchange analysis is the most accurate method, it is impractical for large-scale epidemiological studies (Matthews et al., 1999; Castro-Pinero et al., 2010; Artero et al., 2014). Therefore, indirect estimations of O2max are frequently used to assess large populations or when access to direct measurement is limited.
A number of studies have validated indirect O2max tests in a variety of populations, most of them living at sea level (Leger et al., 1988; Oja et al., 1991; Sproule et al., 1993; Grant et al., 1995; George et al., 1997; Enright et al., 2003; Stickland et al., 2003; Aandstad et al., 2011; Beatty et al., 2012). However, very few studies have addressed the criterion validity of indirect O2max estimation methods when applied at higher altitudes (Gonzalez Camarena and Carrasco Sosa, 1989; Ahmaidi et al., 1993; Falgairette et al., 1994). Previous research has shown that O2max can be affected by altitude (Fulco et al., 1998; Boning et al., 2001; Schmidt et al., 2002); it is not clear to what extent validations, conducted at sea level, can be extrapolated to populations living at moderate altitude (2000 to 3000 m above sea level) (Bartsch et al., 2008). Most O2max estimation approaches employ a variable related to heart rate (HR) in their calculations, and the chronotropic response to exercise can be markedly affected by altitude (Richalet et al., 1992, 2015; Hernandez Lopez et al., 2000; Mourot, 2018), possibly biasing results to an unknown extent. Moreover, several physiological adaptations to moderate altitude can potentially alter O2max estimation under laboratory or field conditions. Perception of maximal exertion, central and peripheral fatigue, cognitive performance (Ando et al., 2019; Heinrich et al., 2019), effects of altitude-induced pH changes and chronic hypoxia on voluntary muscle contractility (Siegler and Marshall, 2015; Ruggiero et al., 2020), changes in hemoglobin mass, blood rheology, and pulmonary hemodynamics after exposure to moderate altitude (Saunders et al., 2013; Raberin et al., 2019), as well as changes in circulating metabolites and hormones, substrate utilization, and respiratory exchange ratio (RER) during exercise can all influence perceptions of effort in laboratory or field tests (Katayama et al., 2010).
Important issues to consider when choosing a test for CRF estimation include accuracy, simplicity, and applicability in specific populations and environments. The 20-m shuttle-run test (20-MST) (Leger et al., 1988), the 2-km walking test (UKK) (Oja et al., 1991), and the perceived functional ability–physical activity rating questionnaire (PFA-PAR) (George et al., 1997) meet these criteria. However, these methods were developed at sea level/low altitude and for the most part, have not been validated at moderate altitude, with the exception of a study in children at high altitude (3700 m) (Falgairette et al., 1994).
Worldwide, an estimated 130 to 140 million people live at moderate altitude (Cohen and Small, 1998; Peñaloza, 2012). Most of them live in Andean cities such as Bogota (2600 m) and Quito (2850 m), on the Mexican plateau (Mexico City, 2250 m), and in the African and south-central Asian highlands. As these are mostly low-to-middle income nations, young and middle-aged adults account for the largest segment of these populations. Therefore, valid CRF assessment methods are needed for use in this context. The purpose of this study was to assess the criterion validity of three equations for O2max estimation based on two exercise-based methods: The 20-MST (a maximal test) and the UKK (a submaximal test); and one nonexercise method: The PFA-PAR questionnaire, in a group of young healthy adults living at 2600 m.
Materials and Methods
The study population consisted of young, apparently healthy medical students who had resided at 2600 m above sea level altitude for at least 2 years. Volunteers were recruited by posters and fliers installed at Universidad del Rosario's Medical School in Bogotá, Colombia. All procedures were reviewed and approved by the institutional review board (Comité de Ética en Investigación, Universidad del Rosario). After providing written informed consent, subjects were screened for cardiovascular exercise contraindications, completed a brief Physical Activity Readiness Questionnaire (Thomas et al., 1992), and provided information on smoking and physical activity habits. Physical inactivity was defined as reporting less than three 30-minute bouts of moderate intensity physical activity per week. Body weight was measured to the nearest 0.1 kg by using a calibrated physician's beam scale (model 338; Detecto, Inc., Webb City, MO), and height was measured to the nearest 1.0 cm by using a stadiometer (Shorr Productions, Olney, MD). Body-mass index (BMI) was calculated as weight in kilograms divided by height in meters squared and rounded to one decimal place (kg/m2). Percent body fat was estimated by using a six-site skinfold method (Yuhasz, 1974) performed by a trained tester. In addition, fasting blood samples were drawn for complete blood count determination and basic clinical chemistry.
Indirect determination of O2max
Before exercise testing, subjects completed the PFA-PAR questionnaire. The PFA-PAR questions were designed to quantify each subject's perceived ability to sustain exercise of moderate intensity and to estimate the subject's present level of physical activity. Responses to the PFA-PAR are translated into O2max estimations by using a validated equation (George et al., 1997). Since this equation was developed for predicting O2max at low altitudes (360 m), we also adjusted PFA-PAR values by linearly decreasing PFA-PAR-estimated O2max in proportion to the expected change in O2max at 2600 m (Fulco et al., 1998).
We instructed all participants not to smoke for at least 72 hours before the testing, and to ingest a low-fat, high-carbohydrate meal 3 hours before testing, along with proper fluid intake. All exercise tests were performed between 14:00 and 18:00 hours. The two exercise field tests (UKK and 20-MST) were performed by each subject, in that order, on a 400-m synthetic outdoor athletic track, with a 2-hour recovery period in between. For the UKK, participants were asked to “complete five laps in the shortest time possible.” Standardized verbal encouragement was given at the start of each subsequent 400-m lap. Only walking was allowed during the test, and stops were permitted, although discouraged. The time needed to cover the 2-km distance was recorded by using a sports chronometer. HR telemetry monitoring (model Vantage NV; Polar Electro Oy., Kempele, Finland) was performed throughout the test, and the mean HR during the last 30 seconds of the test was used for calculations. We used times in the UKK and other covariates to estimate O2max as previously reported (Oja et al., 1991). For the purpose of the percent peak heart rate (%HRpeak) calculation, we used 220-age as the maximal predicted HR.
For the 20-MST, two sets of rubber cones were placed 20 m apart. The participants had to run back and forth between the cones, at a tempo that was dictated by an audio recording. The frequency of the audio signals was set in a way such that initial speed was 8.5 km/h and increased by 0.5 km/h every 1-minute stage. The test was terminated when the participant was unable to keep pace with the audio signals for two or more consecutive laps or became exhausted despite standard verbal encouragement. The last announced stage was used to estimate O2max by using validated equations (Leger et al., 1988).
Direct determination of O2max
Direct O2max was measured by indirect calorimetry using a calibrated Quinton metabolic cart (model Q-4500; Quinton Cardiology, Inc., Bothell, WA). The metabolic cart sampled expired gases from a mixing chamber every 15 seconds, measuring oxygen consumption, ventilation, and RER. The device was calibrated by using two precision-analyzed gas mixtures chosen to span the range of inspired and expired gas concentrations. Stability of the gas calibration was confirmed on a regular basis by analysis of known gases every 10 minutes. The time delay between the gas concentrations and volume signals was measured by passing a bolus of a known gas mixture through the system with a low-dead-space solenoid valve.
An incremental treadmill protocol was used to elicit O2max. During the protocol, we performed continuous 12-lead electrocardiography and HR monitoring. The exercise protocol began at 4.8 km/h in men and 4 km/h in women, with increments of 1.6 km/h every minute, at a constant inclination of 1%. The test lasted until (1) A plateau of oxygen consumption (change <2.0 mL/kg/min) with increasing external work was observed, (2) An RER ≥1.10 was reached, or (3) The subject reached volitional exhaustion (Howley et al., 1995; Edvardsen et al., 2014).
Statistical analysis
A post hoc sample size calculation showed an achieved power of 99% to detect a true Spearman's rank correlation coefficient of at least r = 0.50 between the direct and indirect methods at a nominal significance level of 5% (two-tailed alpha: 0.05).
For descriptive data, continuous variables were expressed as mean ± 1 standard deviation (SD), and categorical variables were expressed as proportions. For continuous variables, we assessed whether they significantly deviated from a normal distribution by using the Kolmogorov-Smirnov goodness-of-fit test. Since most variables did not follow a normal distribution, we obtained Spearman's coefficients and their associated 95% confidence intervals (CI) to assess the correlation between direct O2max measurement and each of the three indirect methods.
Agreement between direct O2max and each of the indirect methods was evaluated by using the standard error of the estimate (SEE), Bland-Altman plots, and the Lin concordance correlation coefficient. The SEE was used as a measure of precision, and it was calculated as
where r is the Pearson correlation coefficient between the direct and indirect method, and SDy is the standard deviation of the indirect O2max measurement. Bland-Altman plots were used to assess the accuracy (mean bias) of each of the indirect methods, and as a secondary assessment of precision by evaluating the limits of agreement. Mean bias was calculated as the mean of the differences between the direct and indirect O2max measurement for each subject. The 95% limits of agreement were calculated as the mean bias ±2 SD of the paired differences. The Lin concordance coefficients (LCC) and their 95% CI were used as a global measurement of agreement and were calculated as previously described (Lin, 1989; Lawrence and Lin, 1992). Analyses were conducted by using Stata 13 (College Station, TX).
Results
We studied 64 adult participants (30 female, 34 male), aged 20.8 ± 1.7, most of them (78%) being physically inactive and 19% being smokers. Average BMI, percent body fat, hemoglobin, hematocrit, fasting plasma glucose, and plasma lipids were within normal ranges (Table 1). The prevalence of excess body weight (BMI ≥25 kg/m2) was 32% for men and 13% for women. As expected for the altitude, hemoglobin values were relatively high, and more markedly so in men than women. All smokers consumed fewer than 10 cigarettes per day.
Characteristics of Study Participants
Variable
All (n = 64)
Males (n = 34)
Females (n = 30)
Demographics
Age (years)
20.8 ± 1.7
21.5 ± 1.6
20.1 ± 1.6
Physically inactive (%)
78
76
80
Smokers (%)
19
27
10
Body composition
Weight (kg)
64.6 ± 12
72.0 ± 10.1
56.2 ± 7.8
Height (cm)
167 ± 9
173 ± 6
159 ± 5
Body-mass index (kg/m2)
23.1 ± 3
23.9 ± 2.7
22.1 ± 3.1
Body fat (%)
15.5 ± 5.4
11.6 ± 3.2
19.7 ± 4
Laboratory—hematologic
Hemoglobin (g/dL)
16.1 ± 1.7
17.5 ± 1.1
14.7 ± 0.9
% Hematocrit (%)
46.9 ± 4.8
50.8 ± 2.9
43 ± 2.7
Laboratory—metabolic
Blood glucose (mg/dL)
78.3 ± 11
77 ± 14
79.5 ± 7.1
Total cholesterol (mg/dL)
169.4 ± 25.4
164.3 ± 28.9
174.2 ± 20.9
HDL cholesterol (mg/dL)
49.1 ± 12.1
47 ± 12.4
51.1 ± 11.6
LDL cholesterol (mg/dL)
103.9 ± 28
100 ± 29.9
107.6 ± 26.1
Triglycerides (mg/dL)
84.6 ± 52.6
95 ± 67.2
74.7 ± 31.4
Values are mean ± SD unless indicated otherwise.
HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Directly measured O2max was higher in men (41.2 ± 5.8 mL/kg/min) than in women (32.2 ± 3.6 mL/kg/min; p < 0.001). Similar gender differences were seen for the O2max estimates provided by the 20-MST, the UKK, and the PFA-PAR questionnaire (Table 2). The 20-MST elicited the highest average peak heart rate (HRpeak) among the exercise protocols (194.2 ± 8.1 bpm [97.5% of predicted]), followed by the direct VO2 measurement (189.2 ± 8.5 bpm [95% of predicted] and 165.9 ± 18.3 bpm [83.3% of predicted]) for the UKK (Table 2).
Peak Heart Rate, Percent Predicted Peak Heart Rate, and O2max by Assessment Method
We found the highest Spearman correlation coefficient between an indirect test and the direct O2max measurement for the 20-MST (r = 0.80; 95% CI: 0.70–0.90), followed by the PFA-PAR (r = 0.72; 95% CI: 0.60–0.84) and the UKK (r = 0.69; 95% CI: 0.57–0.82) (Table 3). The LCC showed considerable variation, with the highest value among indirect methods for the 20-MST, whereas UKK and PFA-PAR displayed lower coefficients (Table 3). Adjustment by altitude greatly improved the agreement between PFA-PAR and the direct method, from 0.57 to 0.71. The SEEs versus the direct method were similar for the four alternative methods, but lowest for 20-MST (3.91 mL/kg/min for 20-MST, 5.48 mL/kg/min for UKK, 4.75 mL/kg/min for PFA, and 4.12 mL/kg/min for altitude-adjusted PFA-PAR).
Spearman Correlation Coefficient, Lin Concordance Correlation Coefficient, and Standard Error of the Estimate for Each O2max Estimation Method Against the Direct Determination
O2max indirect test
Spearman's r (95% CI)
Lin concordance correlation coefficient (95% CI)
Standard error of the estimate (mL/kg/min)
20-MST (n = 64)
0.80 (0.70–0.90)
0.79 (0.70–0.88)
3.91
UKK (n = 64)
0.69 (0.57–0.82)
0.67 (0.54–0.81)
5.48
PFA-PAR (n = 59)
0.72 (0.60–0.84)
0.57 (0.43–0.71)
4.75
Altitude-adjusted PFA-PAR (n = 59)
0.72 (0.60–0.84)
0.71 (0.58–0.83)
4.12
CI, confidence intervals.
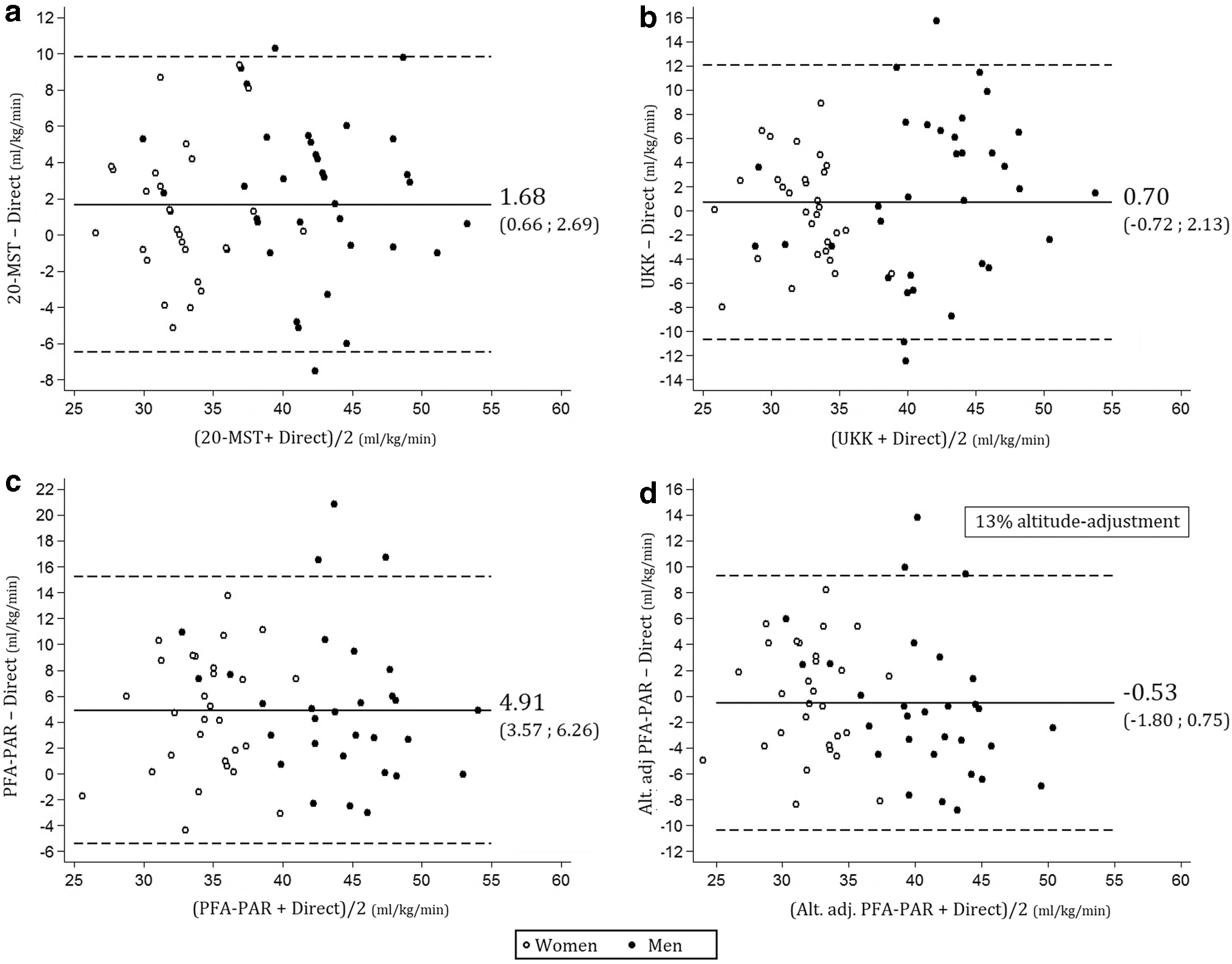
Bland-Altman analyses of agreement showed that the 20-MST tended to over-estimate O2max relative to the direct determination (mean bias 1.68 mL/kg/min; 95% CI: 0.66–2.69). Meanwhile, the UKK showed no significant mean bias (0.70 mL/kg/min; 95% CI: −0.72 to 2.13). The PFA-PAR also over-estimated O2max (mean bias 4.91 mL/kg/min; 95% CI: 3.57–6.26), but this effect disappeared when PFA-PAR values were adjusted by altitude (mean bias −0.53 mL/kg/min; 95% CI: −1.80 to 0.75) (Fig. 1). Bland-Altman limits of agreement were narrowest for the 20-MST (−6.46 to 9.81) and widest for the UKK (−10.68 to 12.09).
Bland-Altman plots of agreement between the direct O2max measurement and the indirect estimation methods. (a) 20-MST, (b) UKK: 2-km walk test, (c) perceived functional ability–physical activity rating questionnaire, (d) altitude-adjusted perceived functional ability–physical activity rating questionnaire. Dashed lines represent the 95% limits of agreement. 20-MST, 20-m shuttle-run test; HR, heart rate; PFA-PAR, perceived functional ability–physical activity rating questionnaire; O2max, maximal oxygen uptake.
Discussion
Our study confirms that O2max can be estimated through maximal (20-MST), submaximal (UKK), and nonexercise (PFA-PAR) methods in young adult populations living at moderate altitude. Several indirect tests for O2max estimation have been extensively validated at low altitude. However, their criterion validity at moderate altitudes is unknown. To the best of our knowledge, this is the first study that has attempted to validate several exercise and nonexercise methods for CRF estimation at moderate altitude. Here, we show that, although previously developed regressions for the 20-MST and the UKK can be applied without modification in our study population, PFA-PAR estimations require an altitude correction factor. These findings will empower researchers at moderate altitude with proven tools to assess and follow up CRF in these populations.
Out of the three indirect methods, the 20-MST showed the highest overall agreement with the criterion measure, an anticipated finding given its maximal nature compared with the other tests. Previous studies of the 20-MST have reported comparable correlation coefficients (Sproule et al., 1993; Grant et al., 1995; McNaughton et al., 1998; Aandstad et al., 2011), SEE values (Leger et al., 1988; Suminski et al., 2004; Ruiz et al., 2009), and Bland-Altman limits of agreement (Aandstad et al., 2011) with the criterion measurement. Some studies have shown no bias between the predicted and measured O2max using the 20-MST in children or adults (Suminski et al., 2004; Aandstad et al., 2011), whereas others have reported significant under-prediction of O2max (Grant et al., 1995; Stickland et al., 2003; Ruiz et al., 2009). A study of circumpubertal boys living at low (300 m) or high altitude (2700 m) assessed O2max by cycle ergometry and the 20-MST (Falgairette et al., 1994), finding significant overestimation by the 20-MST at either altitude. In our study, Bland-Altman analysis also showed an over-estimation of O2max by the 20-MST of 1.68 mL/kg/min at moderate altitude (about half a metabolic equivalent [MET], 1 MET ≈3.5 mL/kg/min), a difference that may bear clinical significance depending on the context of the individual being tested. However, measures of variability (limits of agreement and SEE) were narrowest for the 20-MST when compared with both the UKK and the questionnaire, indicating that the 20-MST was the most precise among the methods assessed.
The UKK walk test has been used to estimate CRF in healthy (Oja et al., 1991; Laukkanen et al., 1992b), overweight (Laukkanen et al., 1992a), and exercise-trained adults (Laukkanen et al., 2000), with an overall good performance (Oja et al., 1991). In our young adult sample, the UKK showed a moderate correlation and agreement with the direct O2max measurement. Given that Bland-Altman analyses indicated no significant bias, a lower agreement could be explained by the lower precision of this test. This is supported by the wider limits of agreement and SEE values. As a submaximal test relying on HRpeak to estimate O2max, the predictive accuracy of the UKK may be lower when compared with a test where physiological mechanisms are driven to a maximal stage. This limitation can be of special concern in healthy young adults when compared with middle-age and older adults, because in the latter group the UKK probably elicits higher relative workloads due to their lower fitness levels and biomechanical limitations (Laukkanen et al., 1992a, 2000). Another factor that may limit the UKK applicability in some settings is the need for accurate HRpeak measurement. HR response to exercise can be impaired by medications, cardiac conduction abnormalities, and, possibly, the effects of altitude. In this regard, prior research has shown that HRpeak can decrease with exposure to extreme altitude (Hernandez Lopez et al., 2000; Mourot, 2018). This effect is believed to be due to increased parasympathetic tone at strenuous exercise. In this study, the chronotropic responses to maximal and submaximal exercise, assessed by HRpeak, were similar to those described for populations at sea level (Oja et al., 1991; Kaminsky et al., 2015). This suggests that the lower validity in the prediction of O2max by the UKK was not related to altitude-impaired chronotropic responses to exercise.
The PFA-PAR questionnaire provides an acceptable estimation of directly measured O2max when a correction factor is applied to the original equation (George et al., 1997) to account for altitude. In our study, Bland-Altman analyses initially demonstrated significant O2max overestimation when the unadjusted-PFA-PAR estimation was compared with the direct measurement. However, a linear adjustment of 13% in the PFA-PAR estimation greatly improved the test's calibration. Analogous adjustments for altitude have also been applied to CRF cutoffs in large epidemiological studies (Ramirez-Velez et al., 2017). Altitude-adjusted PFA-PAR showed an intermediate degree of agreement when compared with the 20-MST and the UKK walk test, a remarkable finding given its nonexercise nature. The correlation of PFA-PAR with the criterion measurement and SEE were within the reported ranges for nonexercised methods (Ross et al., 2016). However, we found a lower correlation compared with the seminal PFA-PAR validation paper (George et al., 1997). In that study, the validity of the questionnaire prediction was limited when subjects were unfamiliar with prolonged exercise, which could affect the subjects' ability to accurately report their subjective exercise capacity. This could have been the case in our sample, which consisted mostly of physically inactive subjects.
The average O2max values for our moderate altitude-acclimatized population were lower than those previously reported for young populations living at low altitude (Kaminsky et al., 2015). According to a study in healthy runners in which altitude was simulated in a hypobaric chamber (Squires and Buskirk, 1982) and a pooled analysis of several studies analyzing changes in O2max with altitude (Fulco et al., 1998), O2max for a 2600 m altitude would be reduced by ∼13%. Our study findings are in agreement with previous reports that show a reduction of about 10%–15% in the peak oxygen consumption in subjects living at 2600 m (oxygen partial pressure ∼65 mm Hg), despite adequate erythropoietic adaptations (Perry et al., 1992; Padilla et al., 1998; Boning et al., 2001, 2004; Schmidt et al., 2002). In fact, hemoglobin and hematocrit values in our sample were comparable to those reported for young untrained populations acclimatized to moderate altitude (Schmidt et al., 2002; Boning et al., 2004), supporting the notion that normal erythropoietic adaptation had already taken place. These findings are consistent with the reported effects of living at altitude, but the effects of lower aerobic power and higher hemoglobin values did not seem to affect the estimation of O2max via indirect field tests. In line with this result, a study in asthmatic adolescents living at moderate altitude (Ahmaidi et al., 1993) found valid O2max estimates using the 20-MST.
It should be noted that, although SEEs and Bland-Altman limits of agreement were within the reported ranges, indirect O2max estimations display a relatively low precision. In our study, the SEEs were equivalent to 1.17 METs for the 20-MST and the altitude-adjusted PFA-PAR questionnaire, and 1.54 METs for the UKK. Given the significant decrease in cardiovascular events and all-cause mortality (13% and 15%, respectively) that has been associated with having a 1-MET higher level of CRF (Kodama et al., 2009; Kaminsky et al., 2013), such a marked variation cannot be accepted at the individual level. On the other hand, the use of indirect methods in epidemiological studies is justified on the basis of their simplicity, lower cost, and the possibility of applying them to a large number of people at the same time (Castro-Pinero et al., 2010). The wide limits of agreement of all indirect methods indicate that none of them can be interchangeably used with the direct method (Bland and Altman, 1986), but for most practical purposes they are intended as a good approximation to O2max, and not as a replacement of the gold standard. Interestingly, it has been demonstrated that exercise (Beatty et al., 2012) and nonexercise O2max indirect methods (Stamatakis et al., 2013; Artero et al., 2014; Nes et al., 2014) are able to predict hard outcomes such as cardiovascular and all-cause mortality on their own, regardless of their relatively lower accuracy versus the direct measurement.
Strengths of our study include the assessment of different aspects of criterion-related validity, not just simple correlation. We employed the Lin concordance correlation coefficient, which performed far better than linear correlation coefficients in assessing overall agreement between the direct and indirect methods. Some studies rely on correlation coefficients to study the validity of an indirect O2max method (Weiglein et al., 2011; Mayorga-Vega et al., 2015), but this approach does not account for the spread of the data or changes in the measurement scale, and it has been extensively discouraged (Bland and Altman, 1986). A significant limitation of our study was the relatively narrow age range of participants (young medical students), which restricts its generalizability to populations with similar demographics. Another relevant limitation could be the nonrandomized order in which we performed the field tests. Still, this is unlikely to have impacted our results because the UKK walk test did not represent a strenuous effort for our young study population, and because the washout period between the two assessments was long enough to allow physiological parameters to return to baseline. Another limitation is the lack of information regarding birthplace of the study participants and their ancestors. It has been shown that adaptations to chronic hypoxia are transmitted between generations (Marconi et al., 2004). However, all subjects had lived at 2600 m for at least 2 years, a period in which acute and chronic adaptations to moderate altitude had already taken place. Further, we acknowledge that our results are applicable only to similar populations of young healthy adults who are not endurance trained and live at moderate altitude. Future studies in which paired estimations can be performed in the same individuals at moderate altitude and at sea level, allowing for an appropriate acclimation time, will confirm and provide greater robustness to our findings.
Conclusion
Adequate estimates of CRF for epidemiological studies can be obtained through maximal, submaximal, and nonexercise methods for populations living at moderate altitude. Among the methods we tested, the highest agreement with the criterion measurement was found for the 20-MST. Given the significant number of young adults living at moderate altitude throughout the world, validation of simple tools for estimating their aerobic power should encourage epidemiological CRF determination in these populations.
Footnotes
Acknowledgments
The authors would like to thank the participating medical students for their cooperation with this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by internal research funding from from the Universidad del Rosario, the Universidad El Bosque, and the Centro de Servicios Biomédicos—Coldeportes Nacional.
References
1.
AandstadA, HolmeI, BerntsenS, and AnderssenSA. (2011). Validity and reliability of the 20 meter shuttle run test in military personnel. Mil Med, 176:513–518.
2.
AhmaidiSB, VarrayAL, Savy-PacauxAM, and PrefautCG. (1993). Cardiorespiratory fitness evaluation by the shuttle test in asthmatic subjects during aerobic training. Chest, 103:1135–1141.
3.
AndoS, KomiyamaT, SudoM, HigakiY, IshidaK, CostelloJT, and KatayamaK. (2019). The interactive effects of acute exercise and hypoxia on cognitive performance: A narrative review. Scand J Med Sci Sports [Epub ahead of print]; DOI: 10.1111/sms.13573.
4.
ArteroEG, JacksonAS, SuiX, LeeD-C, O'ConnorDP, LavieCJ, ChurchTS, and BlairSN. (2014). Longitudinal algorithms to estimate cardiorespiratory fitness: Associations with nonfatal cardiovascular disease and disease-specific mortality. J Am Coll Cardiol, 63:2289–2296.
5.
BartschP, SaltinB, and DvorakJ. (2008). Consensus statement on playing football at different altitude. Scand J Med Sci Sports 18 Suppl, 1:96–99.
6.
BassettDRJ, and HowleyET. (1997). Maximal oxygen uptake: “classical” versus “contemporary” viewpoints. Med Sci Sports Exerc, 29:591–603.
7.
BeattyAL, SchillerNB, and WhooleyMA. (2012). Six-minute walk test as a prognostic tool in stable coronary heart disease: Data from the heart and soul study. Arch Intern Med, 172:1096–1102.
8.
BlairSN. (2009). Physical inactivity: The biggest public health problem of the 21st century. Br J Sports Med, 43:1–2.
9.
BlairSN, KampertJB, KohlHW3rd, BarlowCE, MaceraCA, PaffenbargerRSJ, and GibbonsLW. (1996). Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA, 276:205–210.
10.
BlairSN, KohlHW3rd, PaffenbargerRSJ, ClarkDG, CooperKH, and GibbonsLW. (1989). Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA, 262:2395–2401.
11.
BlandJM, and AltmanDG. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet, 1:307–310.
12.
BoningD, CristanchoE, SerratoM, ReyesO, MoraM, CoyL, and RojasJ. (2004). Hemoglobin mass and peak oxygen uptake in untrained and trained female altitude residents. Int J Sports Med, 25:561–568.
13.
BoningD, RojasJ, SerratoM, UlloaC, CoyL, MoraM, GomezJ, and HutlerM. (2001). Hemoglobin mass and peak oxygen uptake in untrained and trained residents of moderate altitude. Int J Sports Med, 22:572–578.
14.
Castro-PineroJ, ArteroEG, Espana-RomeroV, OrtegaFB, SjostromM, SuniJ, and RuizJR. (2010). Criterion-related validity of field-based fitness tests in youth: A systematic review. Br J Sports Med, 44:934–943.
15.
CohenJE, and SmallC. (1998). Hypsographic demography: The distribution of human population by altitude. Proc Natl Acad Sci U S A, 95:14009–14014.
16.
EdvardsenE, HemE, and AnderssenSA. (2014). End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: A cross-sectional study. PLoS One, 9:e85276.
17.
EnrightPL, McBurnieMA, BittnerV, TracyRP, McNamaraR, ArnoldA, and NewmanAB. (2003). The 6-min walk test: A quick measure of functional status in elderly adults. Chest, 123:387–398.
18.
FalgairetteG, BeduM, FellmannN, SpielvogelH, Van PraaghE, ObertP, and CoudertJ. (1994). Evaluation of physical fitness from field tests at high altitude in circumpubertal boys: Comparison with laboratory data. Eur J Appl Physiol Occup Physiol, 69:36–43.
19.
FulcoCS, RockPB, and CymermanA. (1998). Maximal and submaximal exercise performance at altitude. Aviat Space Environ Med, 69:793–801.
20.
GeorgeJD, StoneWJ, and BurkettLN. (1997). Non-exercise VO2max estimation for physically active college students. Med Sci Sports Exerc, 29:415–423.
21.
Gonzalez CamarenaR, and Carrasco SosaS. (1989). Direct and indirect maximum oxygen consumption in sedentary subjects living at a moderate altitude [in Spanish]. Arch Inst Cardiol Mex, 59:273–278.
22.
GrantS, CorbettK, AmjadAM, WilsonJ, and AitchisonT. (1995). A comparison of methods of predicting maximum oxygen uptake. Br J Sports Med, 29:147–152.
23.
HeinrichEC, DjokicMA, GilbertsonD, DeYoungPN, BosompraN-O, WuL, Anza-RamirezC, OrrJE, PowellFL, MalhotraA, and SimonsonTS. (2019). Cognitive function and mood at high altitude following acclimatization and use of supplemental oxygen and adaptive servoventilation sleep treatments. PLoS One, 14:e0217089.
24.
Hernandez LopezJE, Sierra GalanLM, and Pichel PerezD. (2000). Maximal cardiac rate during treadmill exertion test in 1853 healthy subjects. Its relation with age and under the atmospheric conditions of Mexico City [in Spanish]. Arch Inst Cardiol Mex, 70:261–267.
25.
HowleyET, BassettDRJ, and WelchHG. (1995). Criteria for maximal oxygen uptake: Review and commentary. Med Sci Sports Exerc, 27:1292–1301.
26.
KaminskyLA, ArenaR, BeckieTM, BrubakerPH, ChurchTS, FormanDE, FranklinBA, GulatiM, LavieCJ, MyersJ, PatelMJ, PinaIL, WeintraubWS, and WilliamsMA. (2013). The importance of cardiorespiratory fitness in the United States: The need for a national registry: A policy statement from the American Heart Association. Circulation, 127:652–662.
27.
KaminskyLA, ArenaR, and MyersJ. (2015). Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing: Data from the Fitness Registry and the Importance of Exercise National Database. Mayo Clin Proc, 90:1515–1523.
28.
KaminskyLA, ImbodenMT, ArenaR, and MyersJ. (2017). Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing using cycle ergometry: Data from the Fitness Registry and the Importance of Exercise National Database (FRIEND) Registry. Mayo Clin Proc, 92:228–233.
29.
KatayamaK, GotoK, IshidaK, and OgitaF. (2010). Substrate utilization during exercise and recovery at moderate altitude. Metabolism, 59:959–966.
30.
KatzmarzykPT, ChurchTS, JanssenI, RossR, and BlairSN. (2005). Metabolic syndrome, obesity, and mortality: Impact of cardiorespiratory fitness. Diabetes Care, 28:391–397.
31.
KodamaS, SaitoK, TanakaS, MakiM, YachiY, AsumiM, SugawaraA, TotsukaK, ShimanoH, OhashiY, YamadaN, and SoneH. (2009). Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA, 301:2024–2035.
32.
LaukkanenJA, ZaccardiF, KhanH, KurlS, JaeSY, and RauramaaR. (2016). Long-term change in cardiorespiratory fitness and all-cause mortality: A population-based follow-up study. Mayo Clin Proc, 91:1183–1188.
33.
LaukkanenR, OjaP, PasanenM, and VuoriI (1992a). Validity of a two kilometre walking test for estimating maximal aerobic power in overweight adults. Int J Obes Relat Metab Disord, 16:263–268.
34.
LaukkanenRM, OjaP, OjalaKH, PasanenME, and VuoriIM. (1992b). Feasibility of a 2-km walking test for fitness assessment in a population study. Scand J Soc Med, 20:119–126.
35.
LaukkanenRM, Kukkonen-HarjulaTK, OjaP, PasanenME, and VuoriIM. (2000). Prediction of change in maximal aerobic power by the 2-km walk test after walking training in middle-aged adults. Int J Sports Med, 21:113–116.
36.
LawrenceI, and LinK. (1992). Assay validation using the concordance correlation coefficient. Biometrics, 48:599–604.
37.
LeeD-C, SuiX, ChurchTS, LeeI-M, and BlairSN. (2009). Associations of cardiorespiratory fitness and obesity with risks of impaired fasting glucose and type 2 diabetes in men. Diabetes Care, 32:257–262.
38.
LegerLA, MercierD, GadouryC, and LambertJ. (1988). The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci, 6:93–101.
39.
LinLI. (1989). A concordance correlation coefficient to evaluate reproducibility. Biometrics, 45:255–268.
40.
MarconiC, MarzoratiM, GrassiB, BasnyatB, ColombiniA, KayserB, and CerretelliP. (2004). Second generation Tibetan lowlanders acclimatize to high altitude more quickly than Caucasians. J Physiol, 556:661–671.
41.
MatthewsCE, HeilDP, FreedsonPS, and PastidesH. (1999). Classification of cardiorespiratory fitness without exercise testing. Med Sci Sports Exerc, 31:486–493.
42.
Mayorga-VegaD, Aguilar-SotoP, and VicianaJ. (2015). Criterion-related validity of the 20-M shuttle run test for estimating cardiorespiratory fitness: A meta-analysis. J Sports Sci Med, 14:536–547.
43.
McNaughtonL, HallP, and CooleyD. (1998). Validation of several methods of estimating maximal oxygen uptake in young men. Percept Mot Skills, 87:575–584.
44.
MourotL. (2018). Limitation of maximal heart rate in hypoxia: Mechanisms and clinical importance. Front Physiol, 9:972.
45.
MyersJ, PrakashM, FroelicherV, DoD, PartingtonS, and AtwoodJE. (2002). Exercise capacity and mortality among men referred for exercise testing. N Engl J Med, 346:793–801.
46.
NesBM, VattenLJ, NaumanJ, JanszkyI, and WisloffU. (2014). A simple nonexercise model of cardiorespiratory fitness predicts long-term mortality. Med Sci Sports Exerc, 46:1159–1165.
47.
OjaP, LaukkanenR, PasanenM, TyryT, and VuoriI. (1991). A 2-km walking test for assessing the cardiorespiratory fitness of healthy adults. Int J Sports Med, 12:356–362.
48.
PadillaJ, Eguia LisMC, LiceaJ, and TaylorAW. (1998). Maximal aerobic capacity and sports activity in Mexicans from 13 to 56 [in Spanish]. Arch Inst Cardiol Mex, 68:224–231.
49.
PenalozaD. (2012). Effects of high-altitude exposure on the pulmonary circulation. Rev Esp Cardiol, 65:1075–1078.
50.
PerryME, BrowningRJ, JacksonR, and MeyerJ. (1992). The effect of intermediate altitude on the Army Physical Fitness Test. Mil Med, 157:523–526.
51.
RaberinA, NaderE, AyerbeJL, MucciP, ConnesP, and DurandF. (2019). Evolution of blood rheology and its relationship to pulmonary hemodynamic during the first days of exposure to moderate altitude. Clin Hemorheol Microcirc [Epub ahead of print]; DOI: 10.3233/CH-190671.
52.
Ramirez-VelezR, Palacios-LopezA, Humberto Prieto-BenavidesD, Enrique Correa-BautistaJ, IzquierdoM, Alonso-MartinezA, and LobeloF. (2017). Normative reference values for the 20 m shuttle-run test in a population-based sample of school-aged youth in Bogota, Colombia: The FUPRECOL study. Am J Hum Biol, 29:e22902.
53.
RichaletJP, KacimiR, and AntezanaAM. (1992). The control of cardiac chronotropic function in hypobaric hypoxia. Int J Sports Med, 13;(Suppl 1):S22–S24.
54.
RichaletJP, and LhuissierFJ. (2015). Aging, tolerance to high altitude, and cardiorespiratory response to hypoxia. High Alt Med Biol, 16:117–124.
55.
RossR, BlairSN, ArenaR, ChurchTS, DespresJ-P, FranklinBA, HaskellWL, KaminskyLA, LevineBD, LavieCJ, MyersJ, NiebauerJ, SallisR, SawadaSS, SuiX, and WisloffU. (2016). Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation, 134:e653–e699.
56.
RuggieroL, HoilandRL, HansenAB, AinsliePN, and McNeilCJ. (2020). High-altitude acclimatization improves recovery from muscle fatigue. Med Sci Sports Exerc, 52:161–169.
57.
RuizJR, SilvaG, OliveiraN, RibeiroJC, OliveiraJF, and MotaJ. (2009). Criterion-related validity of the 20-m shuttle run test in youths aged 13–19 years. J Sports Sci, 27:899–906.
58.
SandersLF, and DuncanGE. (2006). Population-based reference standards for cardiovascular fitness among U.S. adults: NHANES 1999–2000 and 2001–2002. Med Sci Sports Exerc, 38:701–707.
59.
SaundersPU, Garvican-LewisLA, SchmidtWF, and GoreCJ. (2013). Relationship between changes in haemoglobin mass and maximal oxygen uptake after hypoxic exposure. Br J Sports Med 47 Suppl, 1:i26–i30.
60.
SchmidD, and LeitzmannMF. (2015). Cardiorespiratory fitness as predictor of cancer mortality: A systematic review and meta-analysis. Ann Oncol, 26:272–278.
61.
SchmidtW, HeinickeK, RojasJ, Manuel GomezJ, SerratoM, MoraM, WolfarthB, SchmidA, and KeulJ. (2002). Blood volume and hemoglobin mass in endurance athletes from moderate altitude. Med Sci Sports Exerc, 34:1934–1940.
62.
SieglerJC, and MarshallP. (2015). The effect of metabolic alkalosis on central and peripheral mechanisms associated with exercise-induced muscle fatigue in humans. Exp Physiol, 100:519–530.
63.
SprouleJ, KunalanC, McNeillM, and WrightH. (1993). Validity of 20-MST for predicting VO2max of adult Singaporean athletes. Br J Sports Med, 27:202–204.
64.
SquiresRW, and BuskirkER. (1982). Aerobic capacity during acute exposure to simulated altitude, 914 to 2286 meters. Med Sci Sports Exerc, 14:36–40.
65.
StamatakisE, HamerM, O'DonovanG, BattyGD, and KivimakiM. (2013). A non-exercise testing method for estimating cardiorespiratory fitness: Associations with all-cause and cardiovascular mortality in a pooled analysis of eight population-based cohorts. Eur Heart J, 34:750–758.
66.
SticklandMK, PetersenSR, and BouffardM. (2003). Prediction of maximal aerobic power from the 20-m multi-stage shuttle run test. Can J Appl Physiol, 28:272–282.
67.
SuiX, HookerSP, LeeI-M, ChurchTS, ColabianchiN, LeeC-D, and BlairSN. (2008). A prospective study of cardiorespiratory fitness and risk of type 2 diabetes in women. Diabetes Care, 31:550–555.
68.
SuminskiRR, RyanND, PostonCS, and JacksonAS. (2004). Measuring aerobic fitness of Hispanic youth 10 to 12 years of age. Int J Sports Med, 25:61–67.
69.
ThomasS, ReadingJ, and ShephardRJ. (1992). Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci, 17:338–345.
70.
YuhaszMS. (1974). Physical Fitness Manual. University of Western Ontario, London, Canada.