
Abstract
Toussaint, Claudia M., Robert W. Kenefick, Frank A. Petrassi, Stephen R. Muza, and Nisha Charkoudian. Altitude, acute mountain sickness, and acetazolamide: recommendations for rapid ascent. High Alt Med Biol. 22:5–13, 2021.
Background:
Sea level natives ascending rapidly to altitudes above 1,500 m often develop acute mountain sickness (AMS), including nausea, headaches, fatigue, and lightheadedness. Acetazolamide (AZ), a carbonic anhydrase inhibitor, is a commonly used medication for the prevention and treatment of AMS. However, there is continued debate about appropriate dosing, particularly when considering rapid and physically demanding ascents to elevations above 3,500 m by emergency medical and military personnel.
Aims:
Our goal in the present analysis was to evaluate and synthesize the current literature regarding the use of AZ to determine the most effective dosing for prophylaxis and treatment of AMS for rapid ascents to elevations >3,500 m. These circumstances are specifically relevant to military and emergency medical personnel who often need to ascend rapidly and perform physically demanding tasks upon arrival at altitude.
Methods:
We conducted a literature search from April 2018 to February 2020 using PubMed, Google Scholar, and Web of Science to identify randomized controlled trials that compared AZ with placebo or other treatment with the primary endpoint of AMS incidence and severity. We included only research articles/studies that focused on evaluation of AZ use during rapid ascent.
Results:
Four doses of AZ (125, 250, 500, and 750 mg daily) were identified as efficacious in decreasing the incidence and/or severity of AMS during rapid ascents, with evidence of enhanced effectiveness with higher doses.
Conclusions:
For military, emergency medical, or other activities involving rapid ascent to altitudes >3,500 m, doses 500–750 mg/day within 24 hours of altitude exposure appear to be the most effective for minimizing symptoms of AMS.
Introduction
Rapid exposure to hypobaric hypoxia, without opportunity for acclimatization, can lead to the development and progression of high-altitude illness, such as acute mountain sickness (AMS). Ascent to altitude for personnel with specialized tasks, such as emergency medical providers, law enforcement, and the military, often involves rapid ascent to high altitudes (>3,500 m) followed quickly by performance of physically demanding tasks (Rodway and Muza, 2011). Therefore, the prevention and treatment of AMS are of critical importance to those having to work at altitude. Recent guidance (Luks et al., 2019) for prevention of AMS recommends acetazolamide (AZ) as the primary prophylaxis. However, most available AZ dosing guidance is focused on slow to modest ascents typical of recreational activities. In this context, our goal in the present discussion is to evaluate a range of dosing strategies for the use of AZ for rapid ascent to altitudes >3,500 m by emergency teams and the military.
Incidence and pathophysiology of AMS
AMS is relatively common in unacclimatized lowlanders (i.e., people who do not live or frequently ascend to altitudes above 1,200 m) who are rapidly exposed to altitudes above 1,500 m (Gallagher and Hackett, 2004; Muza, 2007). Potential incidence rates among this population can range from 20% to 70% (Muza, 2007) as a function of increasing altitude. AMS incidence and severity are primarily related to the individual's altitude acclimatization status (Hansen et al., 1967; Lyons et al., 1995), starting elevation, the altitude reached, the rate of ascent, and the duration of exposure to high altitude (Hackett et al., 1976; Maggiorini et al., 1990; Schneider et al., 2002). Additional factors also include the intensity of physical exertion at altitude (Roach et al., 2000; Beidleman et al., 2013) and individual susceptibility (Robinson et al., 1971). For any given ascent profile and altitude reached, there is a wide range of individual susceptibility to AMS that is likely related to both genetic and environmental variables (Smedley and Grocott, 2013). AMS is most common above 2,500 m but can be seen in highly susceptible individuals at lower elevations (Luks et al., 2017).
Symptoms of AMS commonly appear within 6 to 24 hours of exposure and usually resolve after 2–7 days of altitude exposure if altitude is kept constant (Beidleman et al., 2013; Luks et al., 2017). AMS severity is classified as mild, moderate, and severe both by the worsening of symptoms and by the symptoms impact on performing routine activities (Roach et al., 1993; Bärtsch and Swenson, 2013). Mild-to-moderate AMS is usually temporary and will resolve spontaneously if ascent is stopped and the patient is allowed to rest at the current altitude for 24 hours (Bärtsch and Swenson, 2013; Hofmeyr and De Decker, 2017). Severe AMS may progress into high-altitude cerebral edema, a potentially fatal illness. The definitive treatment is a descent of 300–1,000 m (Luks et al., 2017, 2019).
The exact cause of AMS is not well understood but may be related to hypoxia-induced cerebral vasodilation and subsequent mild edema in the brain. The resulting increased intracranial pressure may trigger the headache, nausea, and fatigue (Hackett and Roach, 2001). However, magnetic resonance imaging (MRI) results are inconsistent with respect to cerebral vasodilation (Fischer et al., 2004). In addition, subsequent research has provided MRI evidence suggesting that cerebral edema formation is not a function of AMS development, but rather a manifestation of acute hypoxia exposure (Mairer et al., 2012). Other reports suggested hypoxia-facilitated release of vascular endothelial growth factor, nitric oxide synthase, and/or bradykinin, which could all act to trigger pain nerve endings in the brain, producing a headache and compromising the blood–brain barrier (Moskowitz, 1990; Mehta et al., 2008).
The three most common pharmacological agents utilized to prevent and/or treat AMS include AZ, ibuprofen, and dexamethasone (DEX) (Gertsch et al., 2010; Luks et al., 2017; Boulet et al., 2018). Historically, ibuprofen has been indicated specifically for relief of headache symptoms of AMS. More recently, ibuprofen was directly compared with AZ for prevention of AMS during high-risk rapid ascents. While ibuprofen provided some efficacy, it demonstrated less effectiveness than AZ and is not recommended for this scenario (Burns et al., 2019). As a corticosteroid, DEX may not be appropriate for use in some individuals with underlying medical conditions such as endocrine disorders, active peptic ulcer disease, upper gastrointestinal (GI) tract bleeding, and certain infections (i.e., amebiasis and strongyloidiasis). Precautions should be taken for those treated with antiseizure medications and concurrent use of alcohol, aspirin, and nonsteroidal anti-inflammatory drugs (Luks and Swenson, 2008). For these reasons, AZ is considered the first-line prophylaxis for AMS (Ellsworth et al., 1991; Luks et al., 2019). Moreover, for multiday missions at high altitude, AZ has the added advantage of promoting ventilatory acclimatization to hypoxia, thus potentially hastening improvements in cognitive and physical performance that typically result from acclimatization (Swenson, 2014). Therefore, we focus in the present study on AZ as the only drug that is specifically approved by the Food and Drug Administration (FDA) for prevention and treatment of AMS (Arky, 1998).
Pharmacology of AZ
AZ works at the level of the kidneys to cause bicarbonate diuresis and metabolic acidosis. This renal effect offsets the respiratory alkalosis caused by altitude-induced hyperventilation and allows increased central chemoreceptor (CCR) sensitivity; the net effect is an augmented ventilatory response in hypoxic environments (Leaf and Goldfarb, 2007). Other evidence suggests that AZ efficacy is due to its augmentation of bicarbonate diuresis, resulting in a decrease in pH of cerebrospinal fluid, which enhances the activity of CCRs, thus stimulating ventilation and augmenting arterial oxygen saturation (SaO2) (Leaf and Goldfarb, 2007). In addition, increased bicarbonate excretion leads to an increase of carbon dioxide in the capillary beds of tissue (including the brain), also further stimulating chemoreceptor activity (Leaf and Goldfarb, 2007; Taylor, 2011).
The goal of the present review was to evaluate the literature to identify the optimal dose of AZ for the prophylaxis and treatment of AMS during rapid ascents to high altitudes (>3,500 m). These situations are likely scenarios for emergency medical and military personnel who must be able to perform complex and/or high-intensity tasks soon after a rapid ascent to high altitudes.
Methods
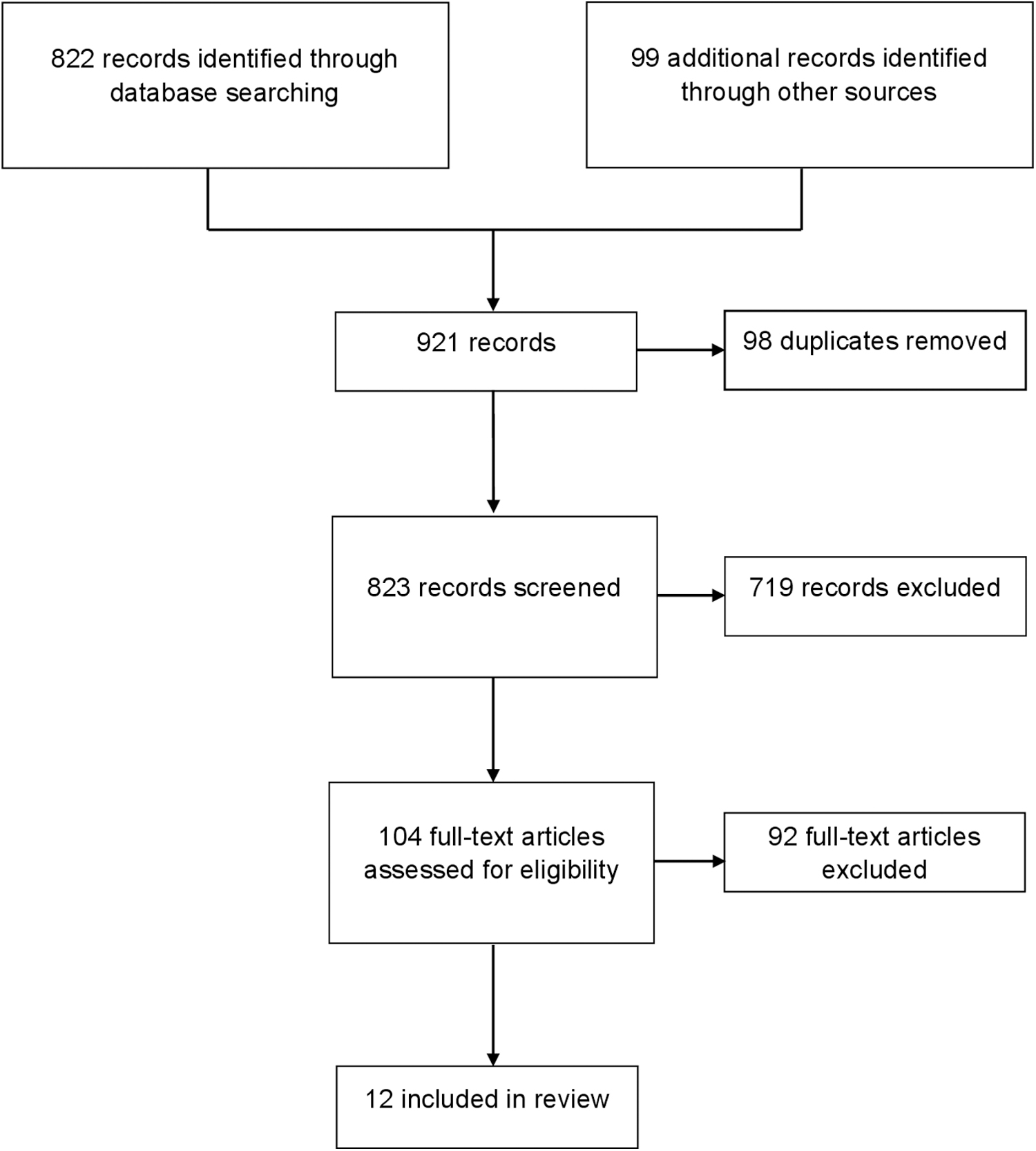
A literature review was conducted during the time frame of April 2018 until February 2020 using PubMed, Google Scholar, and Web of Science. The review occurred over this time period so as to ensure that the most recent articles were captured in the evaluation process. The following free-text terms were searched: acetazolamide, acute mountain sickness, AMS prevention, AMS prophylaxis, pretreatment, dosing, rapid ascent, randomization, and with combinations of these terms using Boolean operators “AND” and “OR,” of which 822 records were identified (Fig. 1). We evaluated 99 additional records through alternative sources such as bibliographies from the retrieved articles, citations, and military technical reports for relevant material. After 98 duplicate materials were removed, we screened 823 records.
Study selection criteria.
Our intent was to identify full-text articles of randomized controlled trials that compared AZ with placebo or other treatment for the prophylaxis and/or treatment of AMS, specific to rapid ascents of >500 m/day.
To be included in the review, articles met the following inclusion criteria: (1) rapid ascent (i.e., ascent to high-elevation destinations within 24 hours at a pace of >500 m/day); (2) mode of ascent (i.e., transport or climbing); (3) AZ utilization as prophylaxis, pretreatment (i.e., at sea level before going to altitude), and/or while at altitude; (4) employed instruments that measured the primary endpoint (AMS incidence and severity); and (5) were conducted at maximum altitudes >3,500 m. Studies were excluded if they: (1) included participants with underlying medical conditions or an advanced stage of altitude illness other than AMS (i.e., high altitude cerebral edema or high altitude pulmonary edema) and (2) combined AZ with another medication as treatment.
Of the 823 articles screened, 719 were assessed against the exclusion criteria and eliminated based on title and/or abstract. A remaining 104 full-text articles, which were published between 1966 and February 2020 were subsequently reviewed. Of the 104 journal articles, 92 did not meet all 5 items of the inclusion criteria, so only 12 research studies were included in this review.
Results
In this section, we review the evidence for efficacy of a range of dosing approaches using AZ to prevent or treat AMS during rapid ascent (Table 1), and the data analyses are summarized in Table 2. The lowest dose evaluated was 125 mg AZ, which was evaluated by Lipman et al. as pretreatment (i.e., ∼9 hours before ascent) and compared with 250 mg daily dose given on the day of ascent (125 mg given at 9:00 AM and at 6:00 PM). These authors found only a minimally higher incidence of AMS (i.e., 9%) with the day of ascent dosing versus the traditional night before approach. However, AMS severity was less (10%) for the “day of ascent” group compared with the “night before ascent” group (22%) (Lipman et al., 2019).
Characteristics of Cited Studies
AMS, acute mountain sickness; AZ, acetazolamide; BL, baseline; SL, sea level.
Data Analyses from Cited Studies
AMS-cerebral score (AMS-C) is derived from ESQ-III and LLS.
ESQ-III, second edition with weighted averages of AMS cerebral and respiratory symptoms (AMS-C and AMS-R).
CI, confidence interval; ESQ-III, Environmental Symptoms Questionnaire-III; GHAQ, General High Altitude Questionnaire; GI, gastrointestinal; HA, headache; LLQ, Lake Louise Questionnaire; LLS, Lake Louise Acute Mountain Sickness Scoring System; PL, placebo; Resp, Respiratory.
Four field studies (Tissot van Patot et al., 2008; Burtscher et al., 2014; Lipman et al., 2018; Burns et al., 2019) used 250 mg daily doses of AZ, as a prophylactic for 3 days, 1 to 9 hours prior, or during ascents to altitudes above ∼3,500 m. Significant decreases in the incidence and severity of AMS were noted in two of the four studies with this dose; however, some AMS remained in the treated groups (43% and 14%), respectively, significantly less in placebo groups (Tissot van Patot et al., 2008; Lipman et al., 2018). Burtscher et al. (2014) found that rapid ascent to 3,480 m (by cable car) caused AMS in five of seven placebo-treated subjects, whereas two of eight subjects treated with 250 mg/day of AZ developed AMS (tended to be statistically significant, p = 0.07). Burns et al. (2019) found that a 250 mg daily dose of AZ was only slightly more effective over ibuprofen for headache prevention during high-risk rapid ascents, with no significant difference in the severity of AMS.
Carlsten et al. (2004) compared two doses (250 and 500 mg/day) given at a baseline altitude (0 hour) and 8 hours into ascent and reported significantly lower AMS scores in the higher dose group. Similarly, Chow et al. (2005) reported that 500 mg/day reduced both the incidence and frequency of AMS (when compared with placebo and Ginkgo biloba treatment). Grissom et al. (1992) studied 12 climbers who went to a clinic with AMS at 4,200 m during an attempted ascent of Mt. McKinley. Over a 24 hour period, in which six climbers were given a total dose of 500 mg and six were given placebo, five of the six climbers taking AZ subsequently experienced a shorter period of AMS as indicated by a lower mean symptom score of <2 and were deemed healthy. All the six climbers who received the placebo still experienced AMS with symptom scores measuring 2 or more.
We noted that studies conducted before 1992 were more likely to evaluate higher doses of AZ. For example, Forwand et al. (1968) evaluated 750 mg/day AZ and reported a significant reduction of severity and frequency of AMS symptoms over placebo. These investigators found improved efficacy within 8 hours into ascent at 3,901 m with a reduction of symptoms during the first 72 hours at altitude. Ellsworth et al. noted greater nausea with 750 mg AZ at baseline altitudes of 1,300–1,600 m but improved sleep in the AZ group at an altitude of 4,392 m. However, in a subgroup analysis, the AZ climbers who presented without side effects reported a prophylactic effect (Ellsworth et al., 1987). In a subsequent study, the investigators compared 750 mg AZ with either DEX or placebo during rapid ascents. They concluded that while DEX was more effective than AZ as a prophylaxis for AMS, it had a propensity for severe adverse reactions and increased risk, so AZ was still regarded as the treatment of choice (Ellsworth et al., 1991).
Larson et al. (1982) studied the effects of 750 mg/day AZ as pretreatment 1 day prior and at altitude, compared with placebo, in preventing AMS and decreasing AMS severity. At 3,000 m, AMS-related symptoms were similar between the groups. However, among those who ascended above 3,000 m, the AZ group had reduced symptom scores for several AMS symptoms, including headache, nausea, dizziness, sleep difficulty, and shortness of breath.
Discussion
The goal of the present review was to focus on dosing of AZ relevant to rapid ascent to high altitude, as relevant to occupations such as emergency medicine and the military. We reviewed the literature in this area published over a 54 year span (1966–2020) and identified 12 of those that met the pre-established inclusion criteria. Based on this review, we recommend dosing of 500–750 mg/day AZ within 24 hours of rapid ascent to altitudes above 3,500 m to minimize symptoms of AMS.
Current clinical practice guidelines for the prevention of AMS using AZ (125 mg every 12 hours) (Luks et al., 2019) are largely based on recreational climbing scenarios using moderate ascent rates to altitudes below 3,500 m (Barry and Pollard, 2003; Gallagher and Hackett, 2004; Netzer et al., 2013; Zafren, 2014; Williamson et al., 2018; Luks et al., 2019). For situations that require rapid ascents to altitudes greater than 3,500 m, the FDA recommends increasing the daily dose up to 1,000 mg (i.e., in divided doses 24–48 hours prior and 48 hours subsequent to ascent) but cautions about the increased risk of adverse reactions from higher dosing (Arky, 1998).
Dumont et al. (2000) conducted a meta-analysis to evaluate the effectiveness of AZ dosing and concluded that AZ dosing guidelines of 250 mg/day are not optimal for rapid ascents to elevations >3,500 m. The authors evaluated AMS incidence in nine studies utilizing AZ and placebo, based solely on the rate of ascent. They concluded that for elevations >4,000 m during a rapid ascent (i.e., >500 m/day), the 750 mg/day AZ, taken prophylactically, was more effective than placebo in preventing AMS, whereas the 500 mg/day was not. However, the interpretation of that study was limited in that (1) the two AZ doses were not compared under equal ascent rates; (2) their review excluded trials that found 500 mg/day to be effective; and (3) their adherence to a strict primary endpoint of “complete prevention of AMS” negated evidence of the prevention of some AMS-related symptoms (Bartsch and Schneider, 2001; Hackett and Roach, 2001).
In a later re-evaluation, Kayser et al. (2012) stratified the relative risk, control event rate (i.e., average incidence of AMS in control subjects of all trials by ascent mode), and number needed to treat by mode of ascent (i.e., climbing, transport and climbing, transport, and hypobaric chamber). The authors concluded that the efficacy of prophylactic AZ was directly proportional to the baseline risk of AMS (i.e., low AZ efficacy linked to low risk of AMS), suggesting that more rapid ascents (with higher risk of development of AMS) would benefit from higher doses (500–750 mg/day).
Sridharan and Sivaramakrishnan (2018) also conducted a meta-analysis of the prophylactic effects of pharmacological interventions for AMS among varying ascent rates. The authors concluded that AZ in daily doses of 250 and 500 mg provided slightly better efficacy with preventing AMS over other interventions (ibuprofen and DEX) (Sridharan and Sivaramakrishnan, 2018).
Adverse reactions to AZ
Although adverse reactions to AZ are not a major focus of the present discussion, we include a brief summary here, particularly since we are recommending higher doses of AZ, and adverse reactions should be taken into account in any risk–benefit analysis before a rapid ascent mission. Common and early occurring dose-dependent adverse reactions to AZ include peripheral paresthesia (notably a tingling sensation in the hands and feet), increased urination (polyuria), loss of appetite, altered taste, particularly of carbonated beverages, and tinnitus (Simancas-Racines et al., 2018; Sridharan and Sivaramakrishnan, 2018). Less common are nausea, headache, and dizziness, which can unfortunately mimic the symptoms of AMS itself (Williamson et al., 2018) as well as GI distress with AZ (Lipman et al., 2019), and possibly occasional drowsiness and confusion (Simancas-Racines et al., 2018). Moderate, but more rare, events include ocular effects such as myopia (Szawarski and Hall-Thompson, 2009). Importantly, for a given dose, adverse reactions to AZ are quite variable across individuals.
Effects on physical performance
One of the concerns for the military and emergency medical personnel is the potential of any medical treatment, which might prevent or alleviate AMS symptoms, to impair physical performance. Posch et al. conducted a literature review to evaluate the effect of AZ with regard to potential impact on exercise performance at both sea level and altitude. Although the authors found that AZ more consistently caused impairments in aerobic exercise performance at sea level, there were more inconsistencies in the literature on the effects of AZ on exercise performance at altitude (Posch et al., 2018). In a more recent placebo-controlled study, investigators found that 500 mg/day AZ did not alter endurance exercise performance in the form of 2 mile run time at 3,500 m altitude (Bradbury et al., 2020). In this context, however, these two recent publications did not attempt to clarify optimal dosing of AZ for rapid ascents to higher altitudes (Posch et al., 2018; Bradbury et al., 2020).
Summary and Conclusions
We have reviewed evidence relative to four doses of AZ (125, 250, 500, and 750 mg daily), with regard to their ability to decrease the incidence and severity of AMS during rapid ascent to altitudes >3,500 m. Although earlier studies used higher doses, it appears that lower doses have become more common in recent decades and that 250 mg/day is sufficient for the majority of people during moderate rates of ascent to lower altitudes (i.e., <3,500 m). However, based on the present review, the military, emergency medical personnel, or others who must ascend rapidly to altitudes above 3,500 m and immediately perform specialized tasks may require dosing of 500 or 750 mg/day.
Authors Contribution
All authors had substantial input in the writing, editing, and revising of this article, and all have reviewed and approved this article before submission.
Footnotes
Acknowledgment
The authors are grateful to Dr. Roy Salgado for his critical review and suggestions for this article.
Author Disclosure Statement
The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as an official United States Department of the Army position, or decision, unless so designated by other official documentation. Approved for public release; distribution unlimited. Citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement or approval of the products or services of these organizations.
Funding Information
Military Operational Medicine Research Program; US Army Medical and Development Command (USAMRDC).