
Abstract
Fornasiero, Alessandro, Aldo Savoldelli, Federico Stella, Alexa Callovini, Lorenzo Bortolan, Andrea Zignoli, David A. Low, Laurent Mourot, Federico Schena, and Barbara Pellegrini. Shortening work-rest durations reduces physiological and perceptual load during uphill walking in simulated cold high-altitude conditions. High Alt Med Biol. 21:249–257, 2020.
Background:
We investigated the effects of two different work-rest durations on the physiological and perceptual responses to a simulated mountain hike in a cold hypoxic environment.
Materials and Methods:
Twelve healthy nonacclimatized active men (age 31.3 ± 5.3 years, body mass index 22.4 ± 1.5 kg/m2) completed a 80-minute work-matched intermittent exercise on a motorized treadmill (25% incline, fixed self-selected speed), in a simulated mountain environment (−25°C, FiO2 = 11%, ≈5000 m a.s.l.), wearing extreme cold weather gear, once with short (20 × 3 minutes walking with 1 minute rest; SHORT) and once with long (10 × 6 minutes walking with 2 minutes rest; LONG) work-rest durations. Heart rate (HR), pulse oxygen saturation (SpO2), rate of perceived exertion (RPE), and thermal sensation (TS) were assessed throughout the exercise protocols. Cardiac autonomic modulation was assessed before (PRE) and after exercise (POST) in supine position, as well as during standing resting periods by means of HR recovery (HRR) assessment.
Results:
SpO2 and TS were similar (p > 0.05) in SHORT and LONG protocols. HR and RPE were increased, and HRR reduced during LONG compared to SHORT (p < 0.05). Parasympathetic activity indices were reduced at POST after both protocols (p < 0.05), but to a lesser extent after SHORT (p < 0.05).
Conclusions:
Reduced work-rest durations are associated with improved perceptual responses and less perturbation of cardiac autonomic balance, compared to longer work-rest durations. Shorter exercise periods from more frequent breaks during hikes at high altitude may represent a valid strategy to limit the impact of exercise under extreme environmental conditions.
Introduction
At high altitude different environmental stressors, such as hypoxia and cold, coexist and affect physiological and perceptual responses to exercise (Castellani and Tipton, 2016; Burtscher et al., 2018). Hypoxia limits exercise tolerance (Wehrlin and Hallén, 2006) and increases exercise-induced perturbation of homeostasis (Mazzeo, 2008), amplifying most of the physiological responses, as well as perceptual strain, for a given absolute submaximal exercise intensity (Mazzeo, 2008; Fornasiero et al., 2019). Furthermore, hypoxic exercise can cause greater Autonomic Nervous System (ANS) disturbance (Hainsworth et al., 2007; Amann and Kayser, 2009; Fisher, 2015; Siebenmann et al., 2019) and delayed postexercise cardiac autonomic recovery (i.e., progressive restoration of normal resting balance between parasympathetic and sympathetic activities) (Al Haddad et al., 2012; Koelwyn et al., 2013; White and Raven, 2014; Michael et al., 2017a; Fornasiero et al., 2018). Similarly, cold stress can exacerbate exercise-induced perturbation of homeostasis (Castellani and Tipton, 2016; Castellani and Young, 2016) and can negatively impact cardiac autonomic recovery (Sanchez-Gonzalez and Figueroa, 2013). Increased physiological stress associated with exercise and inadequate autonomic recovery at high altitude may facilitate the development of maladaptive responses to the environment itself (Sutherland et al., 2017; Boos et al., 2018).
Cardiorespiratory fitness is of paramount importance when dealing with the metabolic requirements of mountain ascents (Bärtsch and Swenson, 2013; Burtscher et al., 2015). Greater cardiorespiratory fitness has been further associated with a decreased rate of perceived exertion (RPE) during trekking at high altitude (≈5000 m above sea level [a.s.l.]) (Rossetti et al., 2017), which has also been related to a lesser impairment of cardiac autonomic balance (Boos et al., 2018) and less acute mountain sickness (AMS) development (Mellor et al., 2014). For the above-mentioned reasons, a moderate exertion during exercise at high altitude has been recommended (Mellor et al., 2014; Boos et al., 2018).
To the best of our knowledge, successful strategies for managing exercise and recovery periods during a mountain hike (i.e., optimal work-to-rest ratio or work-rest duration) have not yet been fully investigated. Intuitively, reducing work-to-rest ratio (i.e., reducing exercise time and/or increasing recovery time) may improve perceptual responses and reduce cardiac autonomic disturbance by means of decreasing the overall mean intensity (Michael et al., 2017a), but this strategy would also increase the time required to complete an ascent. However, the effect of manipulating the work-rest duration during a time-matched exercise (i.e., same time to complete the ascent) seems to be less predictable.
The purpose of this study was to examine the impact of two different work-rest durations on the physiological and perceptual responses to a simulated mountain hike in a cold and hypoxic environment. We hypothesized that reduced work-rest durations during the ascent (i.e., shorter exercise periods and more frequent breaks) would be associated with ameliorated perceptual responses and less impairment of cardiac autonomic balance compared to longer work-rest durations.
Materials and Methods
Participants
Twelve healthy active men (age 31.3 ± 5.3 years, height 176 ± 6 cm, weight 69.3 ± 6.4 kg, body mass index 22.4 ± 1.5 kg/m2) volunteered for this study. None of them had been at altitude above 2000 m for prolonged periods of time (>12 hours) during the previous 3 months before the study. None of the participants involved had clinical evidence of cardiovascular, metabolic, or musculoskeletal diseases. Before data collection, all participants were properly informed about the experimental protocol and gave their written informed consent for the measurements. They were instructed to avoid caffeine, alcohol, and high-intensity exercise during the 24-hour preceding each test session. The experimental protocol was approved by the local ethics committee. The protocol was conducted according to the principles of the Declaration of Helsinki.
Protocol
Each participant visited the laboratory on two different occasions at the same time of the day and completed the experimental protocol within a 2-week period. During each visit, participants randomly performed an intermittent exercise protocol, simulating an 80-minute mountain ascent, on a motorized treadmill (RunRace; Technogym, Gambettola, Italy), either with long (10 × 6 minutes walking with 2 minutes rest; LONG) or short work-rest durations (20 × 3 minutes walking with 1 minute rest, SHORT).
The exercise protocols were conducted in an environmental chamber under controlled laboratory conditions (−25°C, 50% relative humidity). The hypoxic environment was created through the manipulation of the FiO2 by means of an oxygen dilution system based on the Vacuum-Pressure Swing Adsorption principle (B-Cat, Tiel, The Netherlands). FiO2 was set at 11% to simulate an altitude of ≈5000 m a.s.l. To ensure that first short-term physiological responses to the hypoxic environment occurred, participants remained seated quietly in the environmental chamber for 30 minutes before starting the exercise protocols (Duffin, 2007). In the environmental chamber participants wore extreme cold weather clothing (including hat, scarf, and mittens) and high-altitude mountaineering boots, which remained identical for the two protocols, both during exercise and the first 30-minute resting period, during which additional clothes were provided.
Treadmill inclination was kept constant at 25%, whereas speed was gradually adjusted within the first 3 minutes of exercise during the first visit, so as to elicit an individual RPE defined by the participants as “moderate” (25 on the Borg Category Ratio Scale [CR100]) (Borg and Borg, 2002). Previous research suggested that RPE is a valid and appropriate method to record sense of effort and perceptual responses to exercise, as well as to prescribe the target exercise intensity (Eston, 2012). The selected speed was then maintained constant throughout the session and during the second visit, where the same speed adjustment procedure was performed up to the selected speed of the first visit, to match the overall distance covered. Recovery phases were performed in standing position on the treadmill using handrail support.
To investigate the impact of the two exercise protocols on resting cardiac autonomic modulation, heart rate variability (HRV) assessment was conducted before (PRE) and 5 minutes after exercise (POST), with the subject lying in supine position for 10 minutes in a quiet room under normothermic conditions (23°C, 50% relative humidity).
Throughout rest, exercise, and recovery phases, beat-to beat heart rate (HR) was continuously recorded using a Polar RS800CX HR monitor (Polar, Kempele, Finland). Pulse oxygen saturation (SpO2) was continuously recorded during exercise by ear pulse oximetry (Nonin Medical, Minneapolis, MN) at a sampling frequency of 1.0 Hz. The individual RPE was assessed using the CR100 Scale every 6 minutes of accumulated work (Borg and Borg, 2002). Thermal sensation (TS) was assessed using a 9-point scale (from −4 [very cold] to +4 [very hot]) (Arens et al., 2006).
Data analysis
The R-R intervals were uploaded using Polar Precision Performance Software (Polar) and then exported as .txt files. Signal artifacts were filtered out by means of a moderate error correction filter with minimum protection zone of 6 bpm (Al Haddad et al., 2012). All the time series of R-R intervals showed low noise (identified errors <5%). Heart rate recovery (HRR) indices were calculated with a customized script in Matlab (Mathworks, Inc.). HRR60 was calculated from the absolute difference between HRexercise calculated as the mean of the last 30 seconds of exercise and the HR value at 60 seconds of recovery (Buchheit et al., 2007). HRR was also calculated as the relative decline in HR expressed as a percentage of HRexercise (%HRR = HRR/HRexercise × 100), that is, normalized HRR60 (nHRR60). This was done for every 8 minutes of accumulated time (i.e., one cycle for LONG and two cycles for SHORT protocol) to obtain 10 comparable points in terms of accumulated exercise duration.
HRV analysis was performed using Kubios HRV software (version 2.1; Biosignal Analysis and Medical Imaging Group, Kuopio, Finland). HRV indices were calculated considering the last 5 minutes of the 10-minute resting period. The time-domain HRV indices considered were the root mean square of successive differences of R–R intervals (RMSSD), the standard deviation (SD) of normal-to-normal R–R intervals (SDNN), and the percentage of successive R–R intervals differing more than 50 mseconds from the previous R–R interval (Task Force of the European Society of Cardiology, 1996). For frequency-domain HRV indices, low frequency spectral power (LF, 0.04–0.15 Hz), high-frequency spectral power (HF, 0.15–0.4 Hz), and total spectral power (TP, 0–0.4 Hz) were calculated by Fast Fourier Transform (Task Force of the European Society of Cardiology, 1996). Due to the influence of underlying HR on HRV, normalized HRV indices (identified by a “n” in Table 1), according to the methods proposed for time domain and frequency-domain analysis, were also reported (Sacha, 2014; Billman et al., 2015). Mean values of HR and SpO2 were calculated for every 8 minutes of accumulated time, which included for both protocols 6 minutes of exercise and 2 minutes of recovery.
Cardiac Autonomic Modulation Indices PRE and POST SHORT and LONG Protocols
Bold values denote statistical significance at the p < 0.05 level.
Values are mean ± SD. p < 0.05. Normalized HRV data were multiplied by 103 for clarity.
≠ PRE.
≠ SHORT.
HF, high-frequency spectral power; Ln, natural logarithm transformation; LONG, 10 × 6 minutes walking with 2 minutes rest; n, HRV parameter normalized for the mean R–R interval; pnn50, percentage of successive normal interbeat intervals greater than 50 mseconds; RM ANOVA, repeated measures analysis of variance; RMSSD, root mean square of successive differences of R–R intervals; RR, R–R interval; SD, standard deviation; SDNN, standard deviation of normal-to-normal R–R intervals; SHORT, 20 × 3 minutes walking with 1 minute rest; TP, total spectral power.
Statistical analysis
Data are presented as means ± SDs. Data were tested for normal distribution with Shapiro–Wilk test. If data were not normally distributed, natural logarithm transformation (Ln) was applied to obtain a normal distribution and allow parametric statistical comparisons. HRV indices were compared using a two-way analysis of variance (ANOVA) for repeated measures (RM), with “condition” (SHORT and LONG) and “time” (PRE and POST) as factors. HR, SpO2, TS, and RPE values were compared using a two-way ANOVA for RM, with “condition” (SHORT and LONG) and “time” (10 different time points every 6 minutes of accumulated exercise) as factors. When statistical significance was identified, a Sidak post hoc test was used to further delineate differences between condition or time (Cunha et al., 2015). Statistical analysis was completed using a Statistical software (SPSS, Inc., Chicago, IL). The level of statistical significance was set at p < 0.05.
Results
Physiological responses during SHORT and LONG protocol
The average speed in the two protocols was 1.62 ± 0.38 km/h, equal to a mean ascent rate of 404 ± 95 m/h. A significant effect of “condition” (p = 0.028) and “time” (p = 0.001) without “interaction” (p = 0.188) was reported on HR. On average during the whole protocol mean HR was significantly higher in LONG compared to SHORT protocol (136.0 ± 11.9 vs. 131.6 ± 13.9 bpm, respectively). HR gradually increased (p < 0.05) during the first 18 minutes of accumulated work and remained stable throughout the remaining time of the two protocols (Figs. 1 and 2). We reported a significant effect of “condition” (p = 0.003), “time” (p = 0.001), and “interaction” (p = 0.026) on RPE. RPE was significantly higher during LONG compared to SHORT protocol after 36 minutes of accumulated exercise (p < 0.05; points 7, 8, 9, and 10). Differently, we did not find any significant effect of condition (p = 0.491), time (p = 0.461), or interaction (p = 0.336) on TS responses. A significant effect of “time” (p = 0.001) without “condition” (p = 0.394) or “interaction” (p = 0.069) effects was reported on SpO2. SpO2 was significantly decreased after 30 minutes of accumulated exercise compared to the first 6 minutes (p = 0.049) regardless of the protocol. Overall, mean SpO2 was similar (p > 0.05) in SHORT and LONG protocol (62.4% ± 5.6% vs. 63.2% ± 5.4%, respectively).
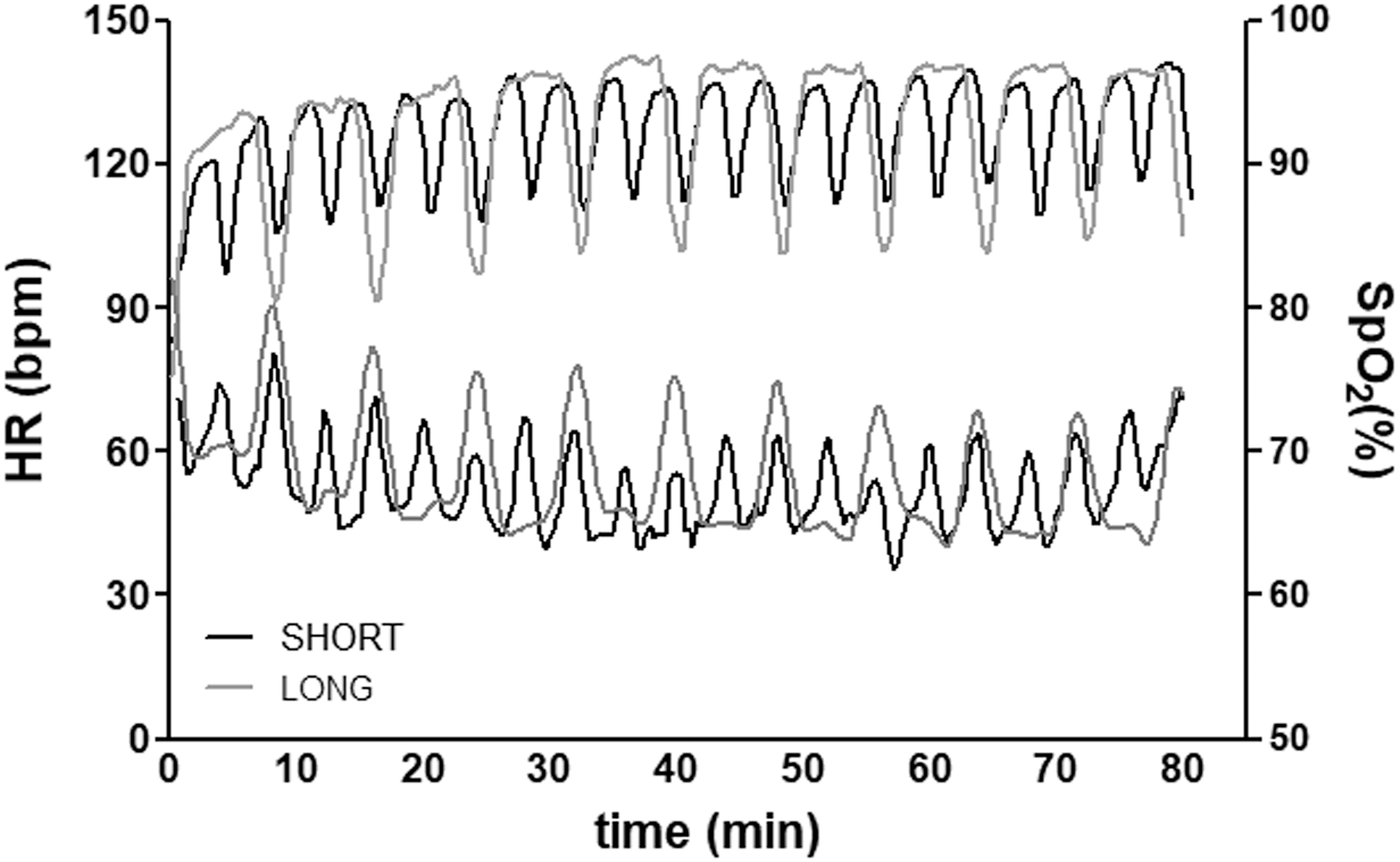
HR (bpm) and SpO2 (%) responses during SHORT and LONG protocols in a representative participant. HR, heart rate; LONG, 10 × 6 minutes walking with 2 minutes rest; SHORT, 20 × 3 minutes walking with 1 minute rest; SpO2, pulse oxygen saturation.

HRR responses during SHORT and LONG protocol
Complete HRR responses during the two protocols are reported in Figure 3. A significant effect of “condition” (p = 0.002) without “time” (p = 0.140) or “interaction” (p = 0.840) effects was found on HRR60. Similarly, only a significant effect of “condition” (p = 0.012) was reported on nHRR60.
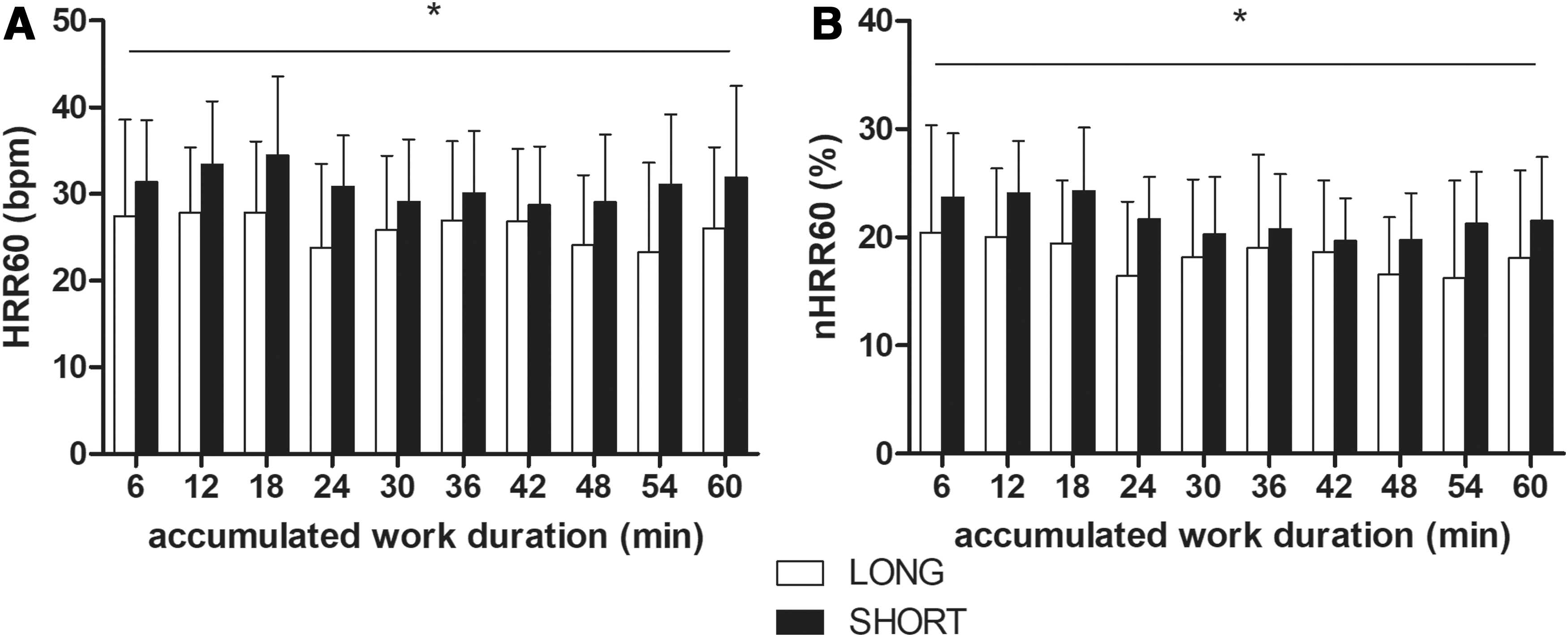
HRR Responses during the two exercise protocols. Black and white bars represent SHORT and LONG exercise protocols, respectively. Error bars represent standard deviation of the mean value; *LONG ≠ SHORT general condition effect; p < 0.05;
Impact of short and long work-rest durations on resting cardiac autonomic modulation
Complete results from two-way RM ANOVA, showing the impact of SHORT and LONG protocols on cardiac autonomic modulation, are reported in Table 1. Mean RR interval was decreased to a greater extent (p = 0.027) at POST after LONG compared to SHORT protocol. Both time- (RMSSD, percentage of successive normal interbeat intervals greater than 50 mseconds [pnn50]) and frequency-domain (HF) HRV indices reflecting parasympathetic activity showed greater reduction at POST in response to LONG protocol (p < 0.05). Similarly, other indices of overall variability (SDNN and TP) showed greater reduction at POST after LONG protocol (p < 0.05).
Discussion
In this study we investigated the impact of two different work-rest durations on the physiological and perceptual responses to a simulated mountain ascent performed under extreme environmental conditions (−25°C, FiO2 = 11%, ≈5000 m a.s.l.) (Fig. 4). The key finding of this study was that shorter work-rest durations were associated with a decreased mean overall physiological strain (i.e., lower mean HR), improved perceptual responses (i.e., reduced RPE), and less perturbation of ANS balance (i.e., lower decrease in vagal-related HRV indices), compared to longer work-rest durations.
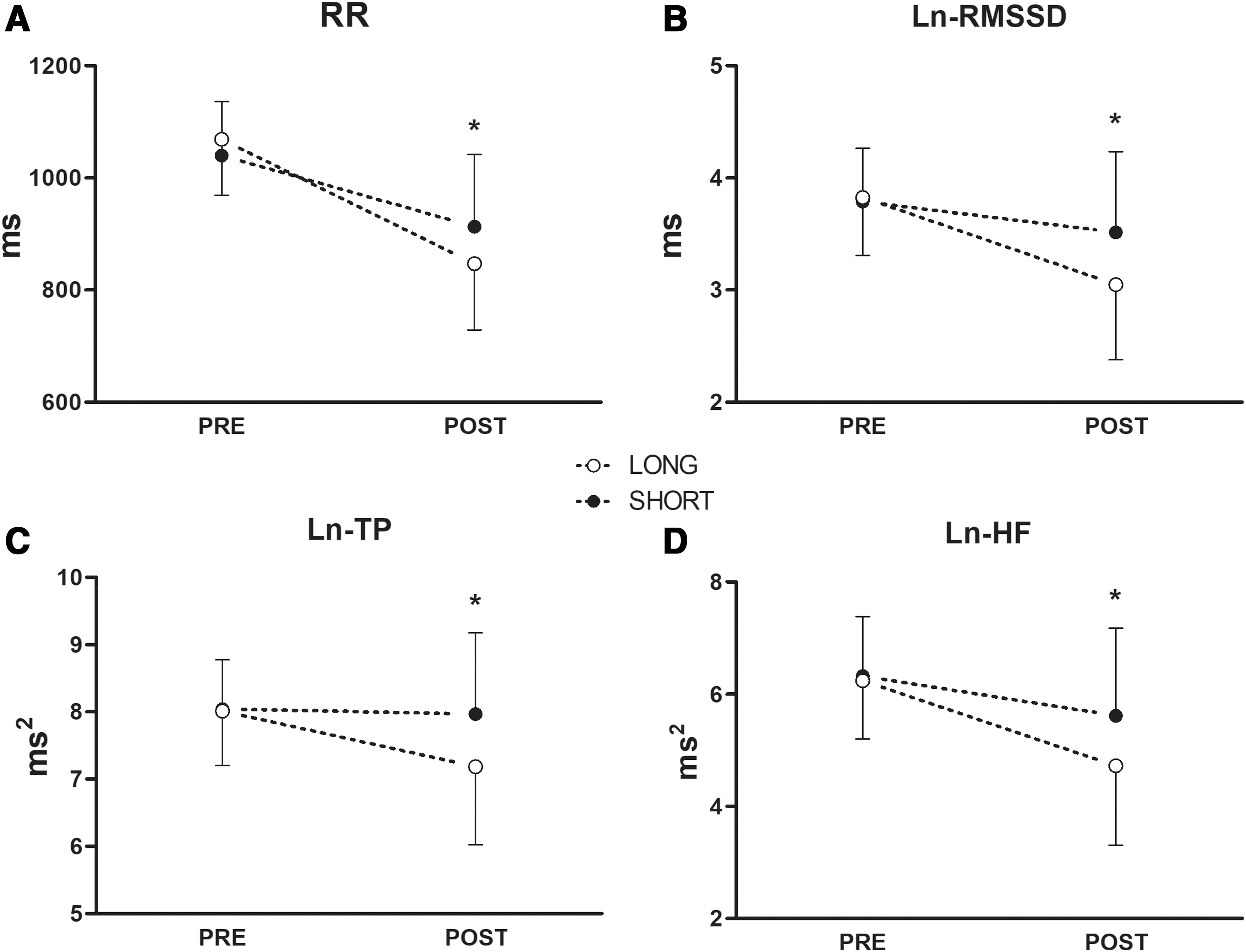
Cardiac autonomic modulation responses before (PRE) and after (POST) the two exercise protocols. Black and white dots represent SHORT and LONG exercise protocols, respectively. Error bars represent standard deviation of the mean value; *LONG ≠ SHORT; p < 0.05;
Physiological responses during SHORT and LONG protocol
Increasing human tolerance to high altitude environments is a key goal for mountaineers, athletes, and anyone who aims to increase the chance of successfully completing ascents at high altitude. Manipulating work-to-rest ratio and work-rest duration significantly alters the physiological and perceptual responses to intermittent/interval exercise (Price and Moss, 2007; Buchheit and Laursen, 2013). At sea level, during work-matched intermittent exercise, longer work-rest durations have been shown to elicit greater physiological and perceptual strain than shorter work-rest durations (Seiler and Sjursen, 2004; Price and Halabi, 2005; Price and Moss, 2007). Similarly, exercise protocols with shorter exercise periods are usually described as more tolerable (Martinez et al., 2015; Farias-Junior et al., 2019). Interestingly, climbing strategies characterized by shorter exercise periods and frequent breaks are spontaneously adopted when facing demanding hikes at extreme altitudes, to decrease the mean overall workload in conditions where exercise tolerance is dramatically reduced (West and Wagner, 1980).
To the best of our knowledge the present study was the first to investigate the impact of manipulating work-rest duration on the physiological (HR and SpO2) and perceptual exercise responses (RPE) to a simulated mountain ascent at high altitude. Using an individual “perceptually-regulated exercise” approach using moderate RPE (Rossetti et al., 2017), participants completed the same external workload (same vertical gain (≈400 m) and total work completed) using two different climbing strategies: SHORT and LONG protocols.
In our study, RPE was significantly increased during LONG compared to SHORT during the second half of the ascent (Fig. 2C). This is in line with existing literature on interval exercise, reporting improved perceptual responses with shorter work-rest durations (Price and Halabi, 2005; Price and Moss, 2007). In addition, despite similar mean SpO2 (Fig. 2B), mean HR was higher in LONG (≈136 bpm) than in SHORT (≈131 bpm; general condition effect) (Fig. 2A). A decreased SpO2 level in hypoxia is a key factor influencing cardiac autonomic modulation due to a direct effect on the carotid chemoreflex (Favret and Richalet, 2007). In this case, other influences may have accounted for the difference in HR between the two protocols. Previous studies have suggested that longer exercise durations directly impact cardiac autonomic responses, resulting in reduced parasympathetic activity (Michael et al., 2017a). A similar influence may be hypothesized for the LONG protocol, where the double duration of exercise bouts may have resulted in higher parasympathetic withdrawal. In line with this observation HRR was reduced during LONG protocol (Fig. 3A, B), underlining a delayed parasympathetic reactivation during transitions from exercise and recovery periods (Michael et al., 2017a; Pecanha et al., 2017).
These divergent responses to SHORT and LONG were not evident in the TS responses to the two protocols (Fig. 2D). TS is governed by core and especially skin temperatures (Filingeri, 2016). Given that the ambient temperature of the environmental chamber and clothing were constant between trials and the amount of work (and therefore heat produced at a fixed efficiency) was matched, core and skin temperatures were likely similar in the two protocols, as well as the thermal stress experienced by the participants.
These findings suggest that shorter exercise bouts and more frequent recovery periods during a simulated ascent at high altitude may result in a decreased mean overall physiological stress (as inferred from mean HR) and in ameliorated perceptual responses, representing a convenient climbing strategy while hiking at high altitude.
Impact of short and long work-rest durations on cardiac autonomic recovery
HRV monitoring is a valid tool to investigate the disturbance induced in ANS balance by an acute bout of exercise (Kiviniemi et al., 2007; Michael et al., 2017a). Particularly, vagal-related HRV indices, such as RMSSD and HF, are the most used indices to investigate postexercise autonomic recovery (Michael et al., 2017a; Pecanha et al., 2017). During exercise, HR increases and HRV decreases, with different contributions from parasympathetic withdrawal and sympathetic activation throughout the exercise intensity spectrum (White and Raven, 2014). After exercise, HR progressively decreases, and HRV indices tend to return to baseline levels (i.e., postexercise parasympathetic reactivation and sympathetic withdrawal) (Michael et al., 2017a; Pecanha et al., 2017; Romero et al., 2017). A clear relationship has been shown between exercise-induced perturbation of homeostasis and postexercise cardiac autonomic recovery (Goldberger et al., 2006; Michael et al., 2017a). Higher exercise intensities (Terziotti et al., 2001; Buchheit et al., 2007; Seiler et al., 2007) and durations (Castrillón et al., 2017; Michael et al., 2017b), as well as the presence of challenging environmental conditions (Al Haddad et al., 2012; Koelwyn et al., 2013; Sanchez-Gonzalez and Figueroa, 2013; Fornasiero et al., 2018), increase exercise-induced homeostatic perturbation and lead to a delayed recovery of HR and HRV indices (Michael et al., 2017a).
In line with existent literature, in this study vagal-related HRV indices (HF and RMSSD) were decreased after both exercise protocols (Fig. 4B, D), indicating incomplete cardiac autonomic recovery 10 minutes after the exercise (Michael et al., 2017a). However, vagal-related HRV indices were decreased to a greater extent in response to the LONG protocol. Similarly, HRV indices of overall variability (SDNN and TP) were significantly decreased at POST only in response to the LONG protocol (Fig. 4C and Table 1). In addition, RR interval, which is a marker of sympathovagal balance (Medeiros et al., 2018), was decreased to a greater extent at POST in response to the LONG protocol (Fig. 4A), which resulted in a higher mean HR and worsened perceptual responses.
This was consistent with previous studies, showing a positive relationship between the increase in exercise-induced perturbation of homeostasis and the delay observed in cardiac autonomic recovery (Michael et al., 2017a; Fornasiero et al., 2018, 2019). The higher impact of LONG protocol on cardiac autonomic recovery was also evident when HRV indices were normalized for the underlying mean RR interval (Sacha, 2014; Billman et al., 2015), which takes into account the influence of HR on HRV measurements (Table 1).
Overall, our results suggest that shorter work-rest durations during the simulated hike were associated with less impairment of cardiac autonomic balance (i.e., smaller reductions in vagal-related HRV indices), compared to longer work-rest durations.
Alterations in ANS activity and particularly in sympathetic/parasympathetic balance associated with exercise stress may play an important role in the development of AMS (Rossetti et al., 2017; Sutherland et al., 2017). Further research is therefore needed to determine the effect of manipulating work-rest duration in real outdoor settings on cardiac autonomic recovery and tolerance to high altitude environments.
Limitations
Some limitations should be considered. As the evaluations were completed at very low ambient temperatures, the assessment of metabolic and ventilatory responses was not possible. Particularly, information regarding respiratory frequency would have helped to explain the higher RPE values reported with a longer work-rest duration, as a close association between respiratory frequency and RPE has been previously suggested (Nicolò et al., 2017). In addition, information regarding exercise-induced metabolite accumulation (e.g., blood lactate concentration [La]b) could have attested a possible sustained metaboreflex and increased sympathetic activation (Romero et al., 2017) in the postexercise period explaining the worsened cardiac autonomic profile after LONG protocol (Peçanha et al., 2016), as well as the increased HR reported during LONG protocol.
Because the duration of the hypoxic exposure was shorter than 6 hours we did not ask participants to complete any AMS questionnaire (Hackett and Roach, 2001). Some subjects (5/12) experienced a temporary headache after exercise, but without any difference between the two protocols.
We are aware that the approach used in the study does not represent the conventional way of being exposed to this kind of altitudes. However, we intentionally chose an altitude that is often reached also without proper acclimatization, being many mountain peaks nowadays partially ascended using cableways.
However, different types of hypoxia, as well as different statuses of acclimatization, have a huge impact on the physiological responses to hypoxic exercise (Netzer et al., 2017; Bhattarai et al., 2018). Accordingly, the results obtained in this study may be limited to the investigated modality of hypoxic exposure/exercise (normobaric hypoxia, 30 minutes of passive exposure +80 minutes intermittent exercise).
Further research, also including acclimatized subjects and a longer postexercise period assessment under hypoxic conditions, is therefore suggested to generalize these preliminary results to real outdoor situations.
Conclusion
Reduced work-rest durations during a simulated mountain ascent at high altitude are associated with a decreased overall physiological strain (i.e., lower mean HR), ameliorated perceptual responses (i.e., lower RPE), and less impairment of cardiac autonomic balance (i.e., smaller reductions in vagal-related HRV indices) compared to longer work-rest durations. Accordingly, shorter exercise periods and more frequent breaks during hiking at high altitude may represent a valid strategy to enhance exercise perceptual responses and limit the impact of exercise on cardiac autonomic recovery under extreme environmental conditions. Further research is needed to generalize these findings to real outdoor settings.
Footnotes
Authors' Contributions
A.F., A.S., L.B., and L.M. participated in study conception and design. A.F., A.S., and F.St. participated in data acquisition. A.F. and F.St. participated in data analysis. A.F. and L.M. were responsible for data interpretation. A.F., A.Z., D.A.L., and L.M. contributed to the draft of the article. A.F., A.S., A.C., A.Z., D.A.L., L.M., ![]() ., and B.P. critically reviewed the article. All authors approved the final version of the article.
., and B.P. critically reviewed the article. All authors approved the final version of the article.
Acknowledgments
The authors are grateful to the participants for their enthusiasm and commitment.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.