
Abstract
Gaur, Priya, Meerim Sartmyrzaeva, Abdirashit Maripov, Kubatbek Muratali Uulu, Supriya Saini, Koushik Ray, Krishna Kishore, Almaz Akunov, Akpay Sarybaev, Bhuvnesh Kumar, Shashi Bala Singh, and Praveen Vats. Cardiac acclimatization at high altitude in two different ethnicity groups. High Alt Med Biol. 22:58–69, 2021.
Introduction:
High altitude (HA) exposure causes substantial increase in pulmonary artery pressure (PAP) and resistance. However, the effects of HA hypoxia exposure on cardiac function remain incompletely understood. Studies evaluating interethnic differences in cardiac functions in response to HA exposure are lacking. We aimed to compare the cardiac performance in Indian versus Kyrgyz healthy lowland subjects over the course of a 3-week HA exposure at 4,111 m.
Methodology:
Ten Indians and 20 Kyrgyz subjects were studied to assess cardiac acclimatization noninvasively by echocardiography in two different ethnic groups for 3 weeks of stay at HA. Pulmonary hemodynamics, right and left ventricular functions were evaluated at basal and on days 3, 7, 14, and 21 of HA exposure and on day 3 of deinduction.
Results:
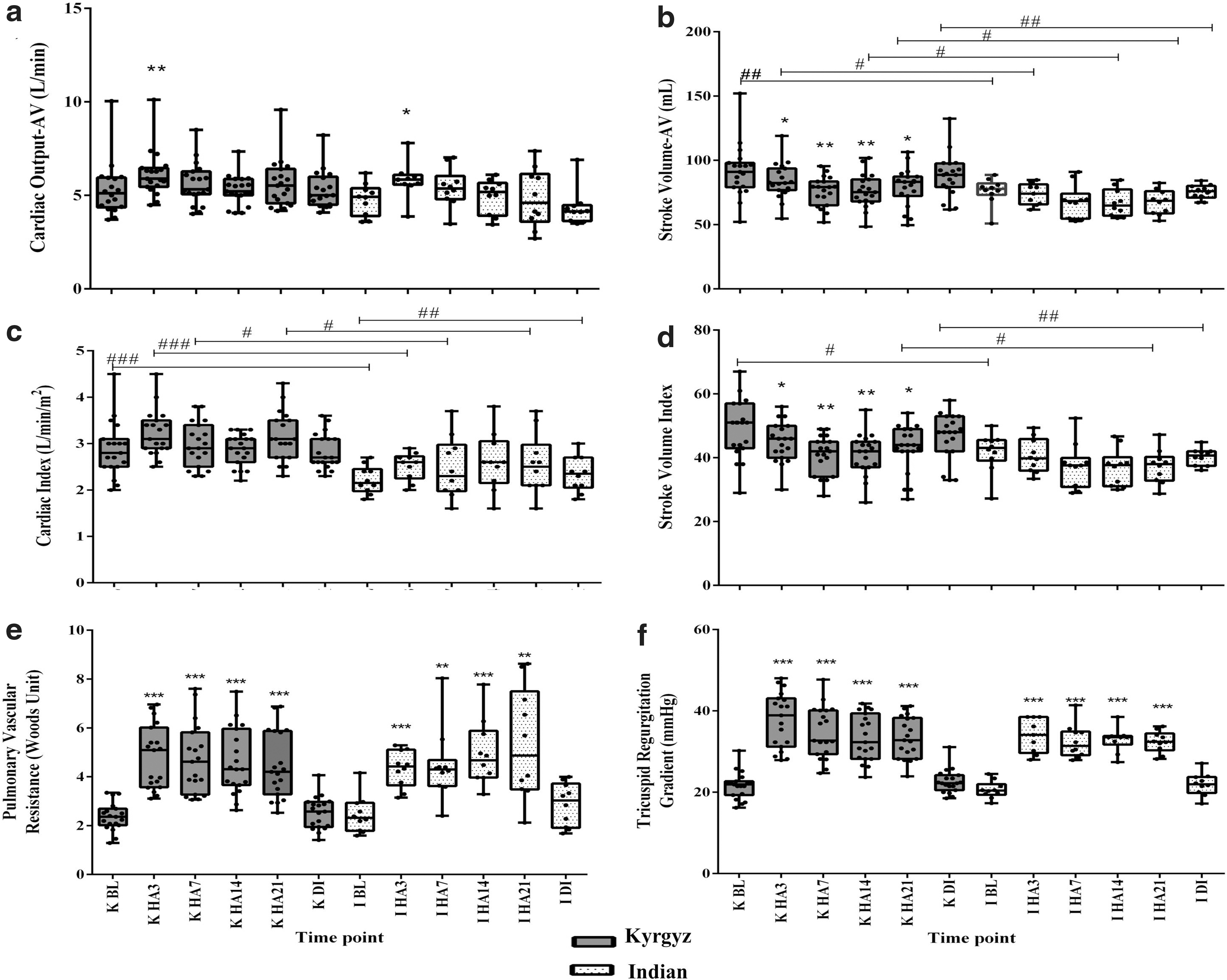
HA exposure significantly increased PAP, pulmonary vascular resistance, cardiac output (CO), and heart rates (HRs) in both groups. Tricuspid regurgitant gradient increased significantly in both the group at day 3 versus basal; 38.9 mmHg (31.8, 42.9) versus 21.9 mmHg (19.5, 22.6) in Kyrgyz; and 34.1 mmHg (30.2, 38.5) versus 20.4 mmHg (19.7, 21.3) in Indians. HR increased significantly in Indians at day 3 and 7, whereas in Kyrgyz throughout exposure. CO increased significantly in both groups at day 3 versus basal with 5.9 L/min (5.5, 6.4) versus 5.1 L/min (4.4, 5.9) in Kyrgyz, and 5.7 L/min (5.56, 5.98) versus 4.9 L/min (4.1, 5.3) in Indians. Both groups exhibited preserved right ventricular diastolic and systolic functions at HAs. HA exposure changed the left ventricular diastolic parameters only in Kyrgyz subjects with impaired mitral inflow E/A, but not in Indian subjects. All cardiac changes induced at HAs have been recovered fully upon deinduction in both, except lateral-septal A′, which remained low in Indians.
Conclusion:
Although pulmonary hemodynamics responses were similar in both groups, there were differences in cardiac functional parameters between the two in response to HA exposure that may be accounted to ethnic variation.
Introduction
High altitude (HA) is defined as an elevation above 2,500 m, and is associated with decreased oxygen saturation in the blood. For maintaining adequate O2 delivery to the tissues, altitude exposure for sports, recreation, and military training, is associated with changes in pulmonary and cardiovascular system. Initial responses to hypoxia exposure are increased heart rate (HR) with increased cardiac output (CO) (Vogel and Harris, 1967; Mason, 2000; Young and Reeves, 2002; Bartsch and Gibbs, 2007). Hypoxic pulmonary vasoconstriction is one of the hallmarks of acute and chronic HA exposure resulting in an increase of pulmonary artery pressure (PAP) and pulmonary vascular resistance (PVR) (Swenson, 2013; Soria et al., 2016).
Chronic HA exposure is also associated with higher PAP in healthy permanent HA residents as compared with lowland residents (Soria et al., 2016) possibly due to pulmonary vascular remodeling (Luks et al., 2017). As previous report has shown that the signs of pulmonary vascular remodeling may be evident after 2 weeks of HA exposure in healthy subjects (Luks et al., 2017). Acute and chronic increase in PVR exert an increased pressure load on the right ventricle, resulting in its structural and functional changes (RV remodeling and dysfunction) as an adaptive response to maintain cardiac function, thus oxygen delivery to the tissues. Hypobaric hypoxia on right ventricular (RV) function in healthy sea-level natives have yielded conflicting results showing preserved (unchanged), increased, or decreased RV function (Huez et al., 2007; de Vries et al., 2010).
Ethnicity studies have been conducted in the past that compared echocardiographic parameters between healthy highlander Tibetans; acclimatized and lowlander natives indicated small left heart and large RV irrespective of ethnic origin (Yang et al., 2018). Sherpa ethnicity highlander versus lowlander were compared after acute HA exposure indicating that despite a higher RV afterload, RV structural enlargement in Sherpa was not evident, probably due to environmental or genetic adaptation (Stembridge et al., 2014). Cardiac adaptation at HA, for RV and left ventricular function, in acclimatized Caucasian lowlanders and Bolivian highlanders was compared pointing qualitative similarity between two (Huez et al., 2009). Echocardiographic reference values for left heart size and left ventricular systolic function according to sex and ethnicity have been established across different ethnicities (The EchoNormal Collaboration, 2015).
Echocardiography remains a reliable method to assess pulmonary hemodynamics noninvasively (Taleb et al., 2013; Greiner et al., 2014). The relation between cardiac function and ethnicities is incompletely understood in lowlander groups of Indian and Kyrgyzstan origin. Moreover, contrast amid different ethnicities is an ever-present concern with HA research. Conduction of echocardiographic studies in different ethnicity lowlanders at HAs might help in delineating the differential responses of the cardiovascular system.
This study prospectively assessed the changed pulmonary hemodynamics, RV and left ventricular functions in Indian and Kyrgyz lowlander healthy subjects during the 21-day HA exposure and upon deinduction. This study will definitely help to understand the cardiac responses at HAs in different ethnic groups and provide as an add-on to the established ethnicity studies. It is essential for establishment of preventive and therapeutic measures for combating the stress environment, improving performance, and healthy stay of soldiers and sojourners at HA.
Methods
Study location and subjects
The study was conducted on 10 Indian (mean age = 23.8 years ±2.1 and mean height 177 cm ±0.04) and 20 Kyrgyz (mean age = 22.6 years ±2.1 and mean height 174 cm ±0.04) healthy male subjects. All subjects were lowlanders with no previous history of HA exposure. They were free from any neurological disorder and cardiac problems. They were not taking any sort of psychotropic, psychoactive, or other drugs during the study.
Indian subjects were flown to Bishkek, Kyrgyzstan, and after 2 days of rest, basal (BL) measurements in Indian and Kyrgyz subjects were carried out at Bishkek (800 m above sea level), Kyrgyzstan. Basal measurements included a health questionnaire history, clinical examination, and echocardiography studies. After baseline examinations, subjects were taken to an altitude of 4,111 m (Syok Pass, Kyrgyzstan) for HA studies, after following the acclimatization protocol (Thakur et al., 2011). After traveling by road in a motor vehicle for 3 hours to the HA research station at 4,111 m, examinations were performed on days 3 (HA3), 7 (HA7), 14 (HA14), and 21 (HA21) of sojourn and after day 3 of deinduction (DI) to Bishkek. Atmospheric temperature was ranging from 28°C to 35°C at Bishkek and −5°C to 9.7°C at Syok Pass; whereas, inside the rooms the temperature was maintained at 22°C ± 2°C. At HA, proper winter clothing was provided to all the subjects. Subjects engaged themselves with morning drill, walking, and other galley duties at HA.
The study protocol was approved by the Executive Board Review Meeting and Ethics Committee of Defense Institute of Physiology and Allied Science (DIPAS), Delhi, and an informed written consent was obtained from all subjects before participation. All the guidelines of Helsinki protocol were followed (World Medical Association, 2013).
Physiological measurements
Individual weight (in kg) was measured using the electronic platform balance (Deca 770; Seca Corporation, USA) at 6:00 to 8:00 A.M. after voiding before breakfast and in minimal clothing. Height was recorded using calibrated height rod (least count 1 mm; Seca Ltd, Medical Scale and Measuring System, Birmingham, United Kingdom). Furthermore, body weight and height were used to derive body mass index (BMI). BMI is defined as the body mass divided by the square of the body height and expressed as units in kg/m2 (Di Angelantonio et al., 2016). Systolic and diastolic blood pressure (BP) along with HR was measured in subjects using mercury-free BP monitoring instrument (OMRON®, USA). They were allowed to take rest for at least 15 minutes before measurements. BP and HR were taken at different time points as per the study protocol. Saturation of peripheral oxygen was measured using finger pulse oximeter (Nonin Medical, Inc., USA). It specifically measures percentage of oxygenated hemoglobin compared with total hemoglobin in blood giving an estimate of arterial oxygen saturation.
Lake Louise acute mountain sickness score recording
Acute mountain sickness (AMS) assessment is a self-questionnaire, which is very direct and based on a common grading system (Roach et al., 2018). Each symptom was scored on a scale between 0 and 3 by volunteers (0 = none; 1 = mild; 2 = moderate; 3 = severe). AMS recording was performed on initial 7 days of HA exposure. Before initial recording, subjects were introduced with the terminologies and meaning of each symptom and they were taught how to identify signs of AMS.
Echocardiography
On days of echocardiographic examination, participants were asked to avoid drinking tea, coffee, and strenuous exercise to limit the effects of sympathetic nervous system activation on cardiac parameters. Echocardiographic images were obtained from parasternal short axis, parasternal long axis, and apical four-chamber views using M-mode, two-dimensional and Doppler echocardiography on fully rested subjects in both supine and left lateral position with a portable ultrasound system (CX50 CompactXtreme; Philips Medical Systems, Amsterdam, the Netherlands) and S5-1 sector array transducer. All reported values represent the average of three or more consecutive cardiac cycles. All measured parameters were taken according to the recommendations of the American Society of Echocardiography (Lang et al., 2005, 2006; Rudski et al., 2010). All images were digitally stored for offline analysis.
After tricuspid regurgitation, flow location by color Doppler imaging, tricuspid regurgitation peak velocity (TRV) was measured using continuous-wave Doppler in the apical four-chamber view. Tricuspid regurgitant gradient (TRG) was used as a surrogate of the estimated systolic pulmonary artery pressure (sPAP), which was automatically calculated from the TRV using simplified Bernoulli equation in the echocardiographic machine.
CO was determined by measuring left ventricular outflow tract diameter (LVOTd) and the time/velocity integral of the LVOT Doppler blood flow (LVOT VTI) (Quinones et al., 2002) using the following formula: CO = π × (LVOTd/2)2 × LVOT VTI × HR.
The mitral and tricuspid inflows were obtained with the pulsed wave (PW) Doppler sample volume positioned at the tips of the mitral and tricuspid valve leaflets in the apical four-chamber view to measure early (E) and late (A) diastolic peak flow velocities.
The PW tissue Doppler imaging (TDI)-derived myocardial peak systolic (mitral S′), peak early (E′), and peak late (A′) diastolic velocities of the mitral annulus at the lateral and septal borders of the mitral annulus were measured in the apical four-chamber view. For the analysis, the average of lateral and septal values were used.
Left ventricular filling pressure index (E/E′) and left atrial pressure (LAP) were derived from the ratio of the Doppler mitral E peak flow velocity to the TDI mitral annulus early diastolic velocity E′ (LAP = 1.9 + 1.24 × E/E′) (Nagueh et al., 1997). PVR was calculated as (sPAP − LAP)/CO (Argiento et al., 2012).
Similarly, PW TDI-derived myocardial velocities of the lateral tricuspid annulus were obtained at the junction of the tricuspid annulus and the RV free wall. The peak systolic (S′) velocity, peak early (E′), and peak late (A′) diastolic tricuspid annular velocities were measured. Echocardiographic measurements were taken by experienced cardiac sonographers (M.S., A.M., K.M.U.), who had no knowledge of the clinical data and days of measurements of the subjects. Recordings were analyzed offline in random order and in a blinded fashion.
Statistical analyses
Continuous variables are presented as median (25th, 75th percentile). Normal distribution of the data was tested using the Kolmogorov–Smirnov test (Supplementary Table S1a–e). Two-way analysis of variance (ANOVA) with adjustments for multiple comparisons was performed with Bonferroni correction. Factors entered into the two-way ANOVA model were ethnicity and time point. All data and calculation were performed with GraphPad prism v6.0 software. Statistical power calculation was performed before experimentation using SigmaStat software v4.0. All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant and are presented with exact values in all the tables and graphs.
Results
Subjects' clinical characteristics
The sequential physiological parameters in the Kyrgyz and Indian subjects are shown in Table 1 and Supplementary Table S2a. Upon ascent to HA, body weight of Kyrgyz individuals decreased significantly during later time points (HA7, HA14 and HA21). The significant loss in body weight was observed at HA14 (p < 0.05). In Indians, the weight loss was not significant. Similarly, BMI decreased significantly (p < 0.05) during altitude stay as compared with basal in Kyrgyz individuals as the body weight decreases. Indians have no change in BMI during altitude stay. However, during all time points, BMI is within normal ranges according to WHO guidelines (WHO, 2004) in both the groups.
Physiological Parameters at Basal and High Altitude: HA3, HA7, HA14, HA21, and After Descent Along with p-Values
Data are presented as median (interquartile range). Groups: KYR and IND.
p < 0.05, **p < 0.01, ***p < 0.001 in Indians and Kyrgyz as compared with their respective BL.
nonsignificant p-value in Kyrgyz as compared with Indians at each time point.
p < 0.01, ##p < 0.05 significant p-value in Kyrgyz as compared with Indians at each time point.
AMS, acute mountain sickness; BL, basal; BMI, body mass index; BP-dia, blood pressure-diastolic; BP-sys, blood pressure-systolic; DI, deinduction; HA, high altitude; HR, heart rate; IND, Indian; KYR, Kyrgyz; SpO2, arterial oxygen saturation.
Systolic and diastolic BP did not change significantly between the two groups upon altitude exposure. Significant increase was seen in systolic BP at HA3 (p < 0.001) and HA7 (p < 0.005) in Kyrgyz, whereas in Indians, the increase was not significant as compared with basal. Diastolic BP was highest at HA3 in Kyrgyz and Indian as compared with basal with a significant increase of p < 0.001 and p < 0.0035, respectively, as compared with their respective BL. Thereafter, the value remained significantly high in Kyrgyz at HA7 (p < 0.0028), HA14 (p < 0.001), and HA21 (p < 0.0373) as compared with its basal. After returning from HA, the BP values returned to almost basal level in Kyrgyz and Indians. In our study, no symptoms of AMS appeared in both the groups as the Lake Louise AMS Score Recording was found to be less than 3 (Table 2).
Acute Mountain Sickness Score in Indian and Kyrgyz Individuals at High Altitude: HA1, HA2, HA3, HA4, HA5, HA6, and HA7 Along with p-Values
Data are presented as median (interquartile range). Groups: KYR and IND.
p < 0.05 in Indians and Kyrgyz as compared with their respective HA1.
nonsignificant p-value in Kyrgyz as compared with Indians at each time point.
p < 0.01 significant p-value in Kyrgyz as compared with Indians at each time point.
Echocardiographic characteristic of subjects
Cardiovascular hemodynamic variables are represented in Figure 1a–f. Kyrgyz subjects display increased HRs at all time points of HA. While, in Indians, HRs increased significantly at earlier stages (on days 3 and 7) of HA, further gradually decreasing to baseline values. Upon deinduction, HRs decreased in both groups (Table 1). Kyrgyz subjects displayed decreased stroke volume at all HA time points. In Indian subjects, stroke volume was unchanged upon HA induction; although the values were nonsignificantly lower at HAs compared with baseline. In addition, in Indian subjects, stroke volume was significantly lower compared with Kyrgyz subjects at both sea level and HA time points. CO increases significantly at HA day 3 in both groups. Later, the values decreased at rest HA time points and returned to baseline values upon deinduction. There is no significant increase in cardiac index upon induction to altitude in both the groups when compared with their baseline values. Intercomparison for cardiac index was significantly higher in Kyrgyz as compared with Indians at BL, HA3, HA7, HA21, and DI. At baseline, both groups displayed similar TRG and PVR values. In both groups, TRG and PVR values significantly increased upon HA exposure and remained elevated over the entire period of HA stay. However, TRG values were nonsignificantly higher in Kyrgyz subjects compared with Indians on day 3 of HA. Upon deinduction, in both groups, TRG and PVR decreased to baseline values.
Both groups displayed similar left ventricular ejection fraction, and were unchanged during the entire period of the study (Table 3 and Supplementary Table S2b). Similarly, lateral mitral S′ wave velocity also showed no change during the entire period of the study. At baseline and upon deinduction, none of the measured parameters of the left ventricle was significantly different between the two groups (Table 3). In Indian subjects, mitral inflow E wave did not change at HA. However, in Kyrgyz subjects, mitral inflow E wave values were decreased at HAs (Fig. 2a). Both groups displayed no change in mitral inflow A wave during the entire period of study. In Kyrgyz subjects, HA exposure significantly decreased mitral inflow E/A ratio at first week of HA stay (Fig. 2b). While Indians displayed nonsignificant gradually decreased mitral inflow E/A ratio over the period of HA stay. In addition, in both groups, mitral annular peak A′, S′ wave velocities, lateral-septal E′/A′ ratio, E/E′ ratio, and LAP remained unchanged at HA acclimatization (Table 3). In Kyrgyz subjects, lateral-septal E′ significantly decreased on days 7 and 14 and further returning to baseline values on days 21 of HA and DI. While, in Indians, lateral-septal E′ wave velocity remained unchanged upon HA exposure (Fig. 2c).

(
Changes in Left Ventricular Functional Variables Assessed at Basal and High Altitude: HA3, HA7, HA14, HA21, and After Descent Along with p-Values
Data are presented as median (interquartile range). Groups: KYR and IND. *p < 0.05 in Indian and Kyrgyz as compared with their respective BL.
nonsignificant p-value in Kyrgyz as compared with Indians at each time point.
Significant p-value in Kyrgyz as compared with Indians at each time point.
A, mitral inflow late diastolic velocity; A′, mitral annulus velocity by TDI during late diastole; E/E′, ratio between the early diastolic mitral inflow velocity E and early diastolic mitral annular velocity E′; E′/A′, tissue Doppler early and late diastolic mitral velocity ratio; LAP, left atrial pressure; LVEF, left ventricular ejection fraction; S′, peak systolic velocity with TDI at the lateral mitral annulus; TDI, tissue Doppler imaging.
Changes in RV functional variables are mentioned in Figure 3a–e, Table 4, and Supplementary Table S2c. In Kyrgyz subjects, tricuspid E wave decreased on day 14 at HA compared with baseline values. While in Indians, HA exposure did not change tricuspid E wave. However, at deinduction, Kyrgyz subjects displayed significantly higher tricuspid E wave compared with Indians. Tricuspid A wave did not change in both groups at HA exposure. HA exposure nonsignificantly decreased tricuspid inflow E/A ratio in Indians at day 3, which was significantly lower compared with Kyrgyz subjects at the corresponding day. In addition, Indian subjects displayed significantly lower values of tricuspid inflow E/A ratio at HA day 14.

(
Changes in Right Ventricular Functional Variables Assessed at Basal and High Altitude: HA3, HA7, HA14, HA21, and After Descent Along with p-Values
Data are presented as median (interquartile range). Groups: KYR and IND. *p < 0.05, **p < 0.01 in Indians and Kyrgyz as compared with their respective BL.
nonsignificant p-value in Kyrgyz as compared with Indians at each time point.
p < 0.01, ##p < 0.05 significant p-value in Kyrgyz as compared with Indians at each time point.
A, tricuspid inflow late diastolic velocity; A′, tricuspid annulus velocity by TDI during late diastole; E′/A′, tissue Doppler early and late diastolic tricuspid velocity ratio; E/E′, ratio between the early diastolic tricuspid inflow velocity E and early diastolic tricuspid annular velocity E′; RVD1, right ventricular basal, RVD2, right ventricular mid cavity; RVD3, RV minor dimensions and the RV longitudinal dimension; tTei, also called myocardial performance index.
In Kyrgyz subjects, tricuspid annular E′ velocity significantly decreased at HAs starting from one week after induction. However, Indians displayed decreased annular E′ velocity only on day 21 of HA stay. However, at deinduction in Indians, tricuspid E′ velocity remained decreased, which was significantly lower compared with Kyrgyz subjects. In Kyrgyz subjects, tricuspid annular E′/A′ ratio was unchanged during the entire period of HA exposure. While, in Indians, tricuspid E′/A′ ratio nonsignificantly decreased after two weeks' stay at HA, which were significantly lower compared with that of Kyrgyz subjects at the corresponding time points. In both groups, estimated RV filling pressure E/E′ ratio did not change during the entire period of investigation. In both groups, tricuspid S′ velocity did not change upon induction to HA; although, its values were significantly lower in Indian subjects compared with Kyrgyz subjects at baseline and on day 3 at HA. Tricuspid annular plane systolic excursion (TAPSE) decreased on day 14 in Kyrgyz subjects, whereas, in Indians, on day 21 at HA. In addition, upon deinduction, in Kyrgyz subjects, TAPSE fully recovered to baseline values, whereas in Indians, its values remained significantly lower compared with that of Kyrgyz subjects.
Discussion
The current study investigated cardiac responses of healthy lowland subjects with different ethnic backgrounds to 3-week HA acclimatization at 4,111 m. To our knowledge, this is the first comparative study carried out on groups of selected lowland subjects, in identical environmental conditions, using the same protocols and experimental setup.
Longitudinal investigation of HR and cardiovascular hemodynamic variables response in both groups upon altitude exposure
Although all subjects displayed increase in HRs during HA exposure, in the present study, a marked difference between two groups was observed with initial increased HR in Indians and throughout Kyrgyz. These findings corroborated with our previous observation of different patterns of HR changes on HA exposure in the two groups (Vats et al., 2013). CO increased during the initial days at HAs (Klausen, 1966; Vogel and Harris, 1967) and is largely explained by the increased HR (Vogel and Harris, 1967). After 1 to 3 weeks of acclimatization, CO normalized due to decreased stroke volume (Vogel et al., 1967). Similarly, in our study, both Kyrgyz and Indian subjects displayed a transient increased CO at HAs, like Sherpas and Tibetans who are known to have the ability to increase CO at an altitude (Gilbert Kawai et al., 2014). In Kyrgyz subjects, stroke volume decreased while in Indians stroke volume was unchanged at HAs. Thus, in line with previous findings, in both groups, CO values were higher due to chronotropic stimulation but not due to increased stroke volume. Over the course of the study, cardiac index values were significantly lower in Indian subjects compared with those of Kyrgyz subjects. However, this may also be explained by the significantly reduced body weights observed in Kyrgyz subjects compared with Indians over the course of HA stay.
Acute exposure to HAs increased PAP due to hypoxia-induced increased PVR. Previous studies indicated that PAP was higher in Sherpa (adapted to HA >3,000 m) and lowlanders exposed to an altitude of 5,050 m in comparison to PAP values of lowlanders at sea level (Stembridge et al., 2014). In another study, human subjects exposed to an altitude of 3,454 m indicate increased PAP during 4 weeks sojourn as compared with sea level and was fully reversible within one week after returning to sea level (Hilty et al., 2016). Similarly, our study of longitudinal investigation over 3 weeks at 4,111 m on pulmonary hemodynamics showed that hypoxic exposure led to increased PAP in both groups. Also, both groups exhibited elevated values of PVR during the entire period of HA stay. Although a previous report has shown that signs of pulmonary vascular remodeling can be noted after 4 weeks stay at HAs (Luks et al., 2017), in our study, in both groups, both PAP and PVR fully recovered upon deinduction.
Preserved RV function after HA exposure in both groups
Increased PVR led to RV pressure overload and susceptible individuals might develop acute RV failure after ascent to HA (Huez et al., 2007). Echocardiographic assessment of RV function in healthy subjects breathing hypoxic gas mixtures revealed that short-term hypoxic exposure is associated with a preserved systolic function and changes in diastolic filling patterns of the right ventricle (Huez et al., 2005; Dedobbeleer et al., 2013).
We did not observe any changes in RV systolic functional variables using tricuspid annular systolic velocity and Tei index in either group contrast to Sherpa ethnicity, which have reduction in RV systolic function followed by chronic altitude exposure (Stembridge et al., 2014). Caucasian lowlanders display higher RV Tei index but maintained RV systolic function (Huez et al; 2009). However, Indians displayed lower tricuspid annular systolic velocity values compared with Kyrgyz subjects at basal and HA3. Nevertheless, both Kyrgyz and Indian subjects displayed decreased TAPSE after 2 and 3 weeks of stay at HA, respectively. These findings were in line with a previous study indicating decreased TAPSE in healthy subjects at 4,200 m after 2 weeks of acclimatization (de Vries et al., 2010). However, some studies showed that TAPSE decreased even at an earlier stage of HA acclimatization at 4,350 m (de Vries et al., 2010).
Taken together, based on tricuspid annular systolic velocity, our data are in line with the results of other studies showing that acute and prolonged hypoxia did not change systolic RV function (Boos et al., 2013; Dedobbeleer et al., 2013). Several studies reported that RV function decreased based on increased Tei index values in healthy lowland subjects upon acute HA exposure (Reichenberger et al., 2007; Huez et al., 2009; Hilty et al., 2016). In contrast, Tei index values have not changed in both groups during the exposure to HA. Measuring RV diastolic function using Doppler (A and E waves, E/A ratio) and tissue Doppler (E′, A′, and E′/A′) echocardiography revealed nonconsistent changes in these parameters with regard to both within- and interethnic comparisons. However, previous studies have shown that E/A ratio is decreased due to increased right ventricular contraction (Maufrais et al., 2017). Thus, more studies with larger sample size are required to know how RV diastolic function changes upon acute exposure to HAs in these two ethnic groups.
Substantial differential response in left ventricular dynamics in Indian and Kyrgyz lowlanders following ascent to 4,111 m
Hypoxia may directly impair myocardial relaxation (Tucker et al., 1976; Gibbs, 2007). The current study reveals that both groups exhibit preserved RV diastolic filling, as shown by maintained tricuspid inflow E/A in both groups at HAs. Similarly, tricuspid annular E′/A′ also remained unchanged at HAs in both groups. However, interventricular interaction between the right and left ventricles may impair left ventricular filling as a consequence of RV pressure overload (Gibbs, 2007).
Our study revealed, only Kyrgyz subjects display impaired mitral inflow E/A with no changes in Indians. Reduced mitral inflow E/A ratio in Kyrgyz subjects resulted from decreased early filling but not from increased left atrial contraction as seen in some of previous reports (Allemann et al., 2004; Rao et al., 2015). The reduced early filling velocity seen in Kyrgyz subjects in this study and also reported previously (Maufrais et al., 2019) may be caused by reduced plasma volume that has been observed in lowlanders upon acute HA exposure in previous studies (Jung et al., 1971; Sawka et al., 1996; Westerterp et al., 1996). However, other groups reported unchanged left ventricular diastolic function in healthy subjects under hypoxic conditions and HA exposure (Bernheim et al., 2007) as seen in Indian subjects in the current study. In one of the recent study, active and rapid ascent of healthy individuals to 4,559 m is associated with an increased contractile performance of the right atrial that compensates for the increased workload of the RV (Sareban et al., 2019). Normalization of left ventricular mechanics in Indians may account for structural and functional adaptation to HAs and are less likely to have symptoms of pulmonary hypertension (Lumens et al., 2010) as compared with Kyrgyz individuals. This likely preserved LV filling is also observed by the controlled HR and sustained diastolic BP in Indians. Nevertheless, these changes are considered as too small to induce pulmonary hypertension, and the clinical significance of this left ventricular diastolic dysfunction is not clear.
In addition, in our study, both left ventricular filling pressure index (E/E′) and estimated LAP remained unchanged during HA stay in both groups, which are in line with previous studies (Maufrais et al., 2019; Sareban et al., 2019). Although, exposure to 4,559 m altitude has been shown to alter left atrial (LA) mechanics, the LA pressure does not change substantially in healthy subjects (Sareban et al., 2019).
Conclusion
In summary, HA exposure led to a significant increase in PAP, PVR, CO, and HRs in healthy subjects. Increased PAP was associated with preserved left ventricular and RV systolic functional parameters; although with modified diastolic indices. The PAP remained elevated over the course of acclimatization in both groups. Deinduction was associated with reversal of HA-induced changes.
The present study indicated significantly altered left ventricular diastolic parameters in Kyrgyz but not in Indian subjects during cardiovascular acclimatization to HAs. Nevertheless, in both groups, all cardiac changes induced at a HA have been recovered fully upon deinduction to low altitude, except lateral-septal A′, which remained low in Indians. Slight differences in the pattern of the changes of diastolic functional parameters were also detected. As a marked genetic diversity exists between Indian and Kyrgyz population (Kivisild et al., 1999; Quintana-Murci et al., 2004; Heyer et al., 2009), these differences in cardiovascular changes observed between Indian and Kyrgyz volunteers during HA acclimatization might be due to ethnic or genetic variation of these two ethnicity groups.
Limitations and future directions
The present study with ethnic specificities of Indian versus Kyrgyz hypoxia-induced echocardiographic changes has some limitations. We acknowledge limitation associated with the sample size, which was kept small and unequal. Due to logistical difficulties and expense associated with work of this nature, large longitudinal studies are less feasible. Future research should attempt to investigate the combined effect of chronic altitude exposure with large sample sizes in Indian and Kyrgyz ethnicity groups. We have applied Bonferroni post hoc analysis in the results obtained from two-way ANOVA model, which decreases statistical power as it overcompensates type 1 error, thus increasing type II error. Conduction of echocardiography studies using similar design, but at higher altitudes, might help delineate the differential responses of the cardiovascular system to HAs in these two population groups.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.