
Abstract
Zhao, Lijun, Xi Wang, Tingli Wang, Wenxin Fan, Honghong Ren, Rui Zhang, Yutong Zou, Huan Xu, Jie Zhang, Yunhong Wu, and Fang Liu. Associations between high-altitude residence and end-stage kidney disease in Chinese patients with type 2 diabetes. High Alt Med Biol. 21:396–405, 2020.
Background:
This study investigated whether living at high altitude was associated with progression to end-stage kidney disease (ESKD) in Chinese patients with diabetic nephropathy (DN).
Materials and Methods:
This retrospective study included 369 patients with type 2 diabetes mellitus (T2DM) and biopsy-confirmed DN. Cox proportional hazards models were used to estimate hazard ratios (HRs) for the influence of living at high altitude on ESKD.
Results:
Patients living at ≥2,000 m above sea level were more likely to be Tibetan, and they had higher mean body mass indexes, glycosylated hemoglobin, hemoglobin concentrations, and baseline estimated glomerular filtration rates than those living at lower altitudes. During a median follow-up period of 20 months, 141 (38%) patients progressed to ESKD. In multivariable Cox analysis adjusted for age, sex, ethnicity, and clinical and pathological parameters, living at high altitude was independently associated with progression to ESKD in Chinese DN patients [HR 2.83, 95% confidence interval (CI) 1.05–7.58]. Compared with Han Chinese, Tibetans were at a lower risk of progression to ESKD (HR 0.15, 95% CI 0.04–0.59).
Conclusions:
Living at high altitude was independently associated with renal outcome in Han Chinese patients with T2DM and DN, but not native Tibetans.
Introduction
Diabetic nephropathy (DN) is one of the most common microvascular complications associated with diabetes mellitus. Paralleling the dramatic global rise in the prevalence of diabetes mellitus, DN has become the leading cause of end-stage kidney disease (ESKD) worldwide (Wang et al., 2017). High altitude is characterized by low oxygen pressure and low oxygen content. In recent studies, populations living at high altitudes were reportedly at risk of high-altitude renal syndrome, a condition characterized by erythrocytosis, microalbuminuria, hypertension, and hyperuricemia (Arestegui et al., 2011). The kidneys are highly metabolic organs, and at rest they are the second-highest consumers of molecular oxygen in the body (Pagliarini et al., 2008). In hyperglycemic patients, the diabetic kidney is under increased intrarenal oxidative stress (Jha et al., 2016), causing increased kidney oxygen consumption and rendering the kidney hypoxic (Friederich-Persson et al., 2013).
Hypoxia arising from high altitude is a challenge with regard to kidney function. Hansen et al. (1994) reported that acute altitude hypoxia increased urinary protein excretion approximately threefold, constituting direct evidence for hypoxia-associated kidney injury. People of mixed European-Andean heritage living at high altitude (3,640 m) in La Paz in Bolivia who were considered healthy had worse kidney function and a higher prevalence of proteinuria than those living at ∼154 m above sea level in Lima in Peru (Hurtado-Arestegui et al., 2018). In healthy native highlanders, however, living at high altitude resulted in multiple compensatory responses, including adaptive genetic changes. Some native Tibetan, Andean, and Ethiopian populations that have lived at altitudes ranging from 3,000 to 4,000 m above sea level for thousands of years have putatively adaptive versions of two hypoxia-inducible factor (HIF) pathway genes, EPAS1 and EGLN1 (Simonson et al., 2015). Thus, kidney reactions to long-term exposure to high altitude may be associated with pre-existing kidney disease, pre-existing risk factors, race, and geographic location.
In China, there is reportedly a higher prevalence of DN in plateau areas than in plains areas (Zhang et al., 2019). The risk factors associated with renal outcomes remain unclear, however, as do the relevant clinical and pathological characteristics in patients who live at high altitude or at low altitude. In the current longitudinal retrospective study, associations between living at high altitude and renal outcomes were investigated in Chinese patients with type 2 diabetes mellitus (T2DM) and biopsy-proven DN.
Methods
Patient selection and study design
This longitudinal observational study included patients with T2DM and DN who had undergone percutaneous renal biopsy between May 2003 and January 2019 at the West China Hospital of Sichuan University. The indications for renal biopsy were T2DM with renal damage, lack of preclusive contraindications, lack of diabetic retinopathy but presence of obvious glomerular hematuria, short duration of diabetes, and sudden-onset overt proteinuria (Li et al., 2017). T2DM was diagnosed in accordance with the American Diabetes Association criteria (Pinsker et al., 2015). DN was defined in accordance with the criteria described in An et al. (2015), and it was diagnosed by at least two renal pathologists and/or nephrologists by using Tervaert's classification system (Tervaert et al., 2010).
Adults with T2DM and biopsy-confirmed DN were eligible for inclusion in the study. The exclusion criteria were the presence of coexisting non-diabetic kidney diseases such as immunoglobulin A nephropathy, systemic conditions including antineutrophil cytoplasmic antibodies (which are associated with vasculitis), antiglomerular basement membrane disease, lupus nephritis, non-T2DM, and progression to ESKD before renal biopsy (Supplementary Fig. S1). A total of 369 patients with DN were ultimately enrolled in the study. All patients provided written informed consent, and the study was approved by the institutional review board of the West China Hospital of Sichuan University.
Definition of low altitude and high altitude
In accordance with previous studies (Betz et al., 2011; Yuwen et al., 2018) patients living <2,000 m above sea level were assigned to a low-altitude group (n = 317), and patients living ≥2,000 m above sea level were assigned to a high-altitude group (n = 52).
Clinical and laboratory data
Baseline demographic and clinical data, including age, sex, body mass index (BMI), smoking status, presence of diabetic retinopathy, 24-hour urinary protein excretion, and use of renin-angiotensin aldosterone system blockade, hypoglycemic agents, or statins, were obtained from electronic medical records at the time of renal biopsy. Estimated glomerular filtration rates (eGFRs) were calculated by using the creatinine-based Chronic Kidney Disease (CKD) Epidemiology Collaboration equation (Mise et al., 2017). Hematuria was defined as >5 erythrocytes per high-power microscopy field in at least 2 of 3 consecutive urine tests in the absence of urinary infection, urinary tract malignancy, and kidney stone (Zhao et al., 2020). Treatment was defined as the use of renin-angiotensin aldosterone system blockade, hypoglycemic agents, and/or statins for more than half of the follow-up period. The patients attended follow-up appointments two to four times annually, depending on their clinical condition.
Histopathological findings
Renal biopsy samples were prepared for light microscopy, immunofluorescence, and electron microscopy by using West China Hospital's standard procedures. For light microscopy examination, renal specimens were stained with hematoxylin and eosin, periodic acid-Schiff, Masson's trichrome, and periodic acid-Schiff silver methenamine. The original immunofluorescence microscopy and electron microscopy results were used to confirm the diagnosis of DN. All light microscopy pathological findings were defined and classified in accordance with the renal pathology society DN classification system (Tervaert et al., 2010). All renal specimens were examined by two nephropathologists who were blind to the clinical data and renal outcomes.
Immunohistochemical staining
Sections (3-μm thickness) cut from 10% formalin-fixed, paraffin-embedded kidney samples were used for immunostaining for HIF-1α (NB100–131; Novus Biologicals, USA) as previously detailed (Zhao et al., 2018). Briefly, heat-induced antigen retrieval (pH 9.0) and peroxide block were performed in preparation for incubation with anti-HIF-1α mouse monoclonal antibody, and they were incubated with a horseradish peroxidase (HRP)-conjugated goat anti-mouse antibody (8125; CST, USA) at 37°C for 1 hour. Antibody binding was detected by incubating with a fresh mixture of diaminobenzidine (8059S; CST) according to the manufacturer's instructions. Images were captured with a Nikon DXM 1200/NIS-Elements mounted on a light microscope (Nikon Eclipse E600, Shanghai, China) and analyzed by using ImageJ software. HIF-1α staining quantification was determined as the ratio of staining-positive area/cortex area.
Renal outcome
The primary renal outcome was progression to ESKD, defined by an eGFR <15 ml/min/1.73 m2, or the commencement of renal replacement therapy (An et al., 2015; Zhao et al., 2020). All patients were followed up in our outpatient department. The last follow-up timepoint was November 2019.
Statistical analysis
Continuous variables are expressed as means and standard deviations if normally distributed, or as medians and interquartile ranges (IQRs) if non-normally distributed. Categorical variables are expressed as counts and percentages. Differences between continuous variables were analyzed by using Student's t-test or the Wilcoxon test, and categorical variables were analyzed by using the chi-square test or Fisher's exact test.
Survival curves were generated via Kaplan–Meier methods with a log-rank test. Univariate and multivariable Cox proportional hazards models were used to estimate hazard ratios (HRs) for ESKD (Gray, 1999). Baseline 24-hour proteinuria data were missing for 22 patients, and hemoglobin data were missing for 1. Differences in clinical parameters between patients with and without missing values were assessed first, to check whether the distribution of missing values was random. Multiple imputation methods were then used to derive multivariable models (Mise et al., 2014). The proportional hazards assumption in Cox models was tested to check whether the datasets satisfied the inherent assumptions of Cox analysis. The Cox proportional hazards model was used to calculate HRs and 95% confidence intervals (CIs) for ESKD. In “multivariable model a” the HRs were adjusted for age, sex, eGFR, 24-hour proteinuria, serum hemoglobin, albumin, and fasting plasma glucose at the time of renal biopsy as continuous variables, renin-angiotensin aldosterone system inhibitor usage and renal pathological parameters as categorical variables. In “multivariable model b” the HRs were adjusted for the aforementioned factors plus ethnicity. The clinical covariates were selected as potential confounders because of their significance in univariate analysis or on the basis of biological plausibility. Age and sex were chosen on the basis of biological plausibility. Baseline serum hemoglobin, albumin, 24-hour proteinuria, and eGFR were significant in the univariate model. Parameters with p < 0.05 in model b were considered to be significant prognostic indicators. Linear regression analysis was used to determine correlations between clinical parameters and demographic parameters.
Statistical analyses were performed by using Stata version 14.0 (StataCorp LLC, College Station, TX) or SAS version 9.4 (SAS Institute Inc., Cary, NC). p < 0.05 was deemed to indicate statistical significance.
Results
Clinical and pathological characteristics
The baseline clinical characteristics of all patients are shown in Table 1. Of the 369 patients enrolled in the study, 257 (70%) were male. At the time of biopsy the median baseline eGFR was 58.2 ml/min/1.73 m2 (IQR 42.6–92.3) and the median baseline 24-hour proteinuria was 4.19 g/day (IQR 1.99–7.75). The median altitudes of residence were 500 m in the low-altitude group and 3,650 m in the high-altitude group. The median baseline eGFRs were 57.6 ml/min/1.73 m2 (IQR 42.0–89.2) in the low-altitude group and 85.5 ml/min/1.73 m2 (IQR 48.7–102.6) in the high-altitude group (p = 0.03). Compared with the low-altitude group, the high-altitude group had higher baseline BMI, eGFR, glycosylated hemoglobin (HbA1c), and hemoglobin concentrations, but lower baseline triglyceride concentration. The high-altitude group had a higher prevalence of males than the low-altitude group, and a significantly higher prevalence of Tibetans (78% vs. 2%). There were no significant differences in duration of diabetes, systolic or diastolic blood pressure, albumin concentration, or 24-hour proteinuria between the two groups. Patients in the high-altitude group used oral hypoglycemic agents more frequently than those in the low-altitude group. There were no significant differences in the use of other medications between the two groups.
Baseline Demographic and Clinical Characteristics of Patients with Biopsy-Proven Diabetic Nephropathy
Data are presented as the mean (standard) for continuous variables with symmetric distribution, median (25th-75th percentiles) for continuous variables with asymmetric distribution, or percentages for categorical variables.
CKD stage 1: eGFR ≥90 ml/min/1.73 m2; stage 2: eGFR 60–89 ml/min/1.73 m2; stage 3: eGFR 30–59 ml/min/1.73 m2; stage 4: eGFR 15–29 ml/min/1.73 m2.
BMI, body mass index; BUN, blood urea nitrogen; CKD, chronic kidney disease; DBP, diastolic blood pressure; DR, diabetic retinopathy; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; HPF, high power field; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; MAP, mean blood pressure; OHA, oral hypoglycemic agents; RAAS, renin-angiotensin-aldosterone system; RBC, red blood cell; SBP, systolic blood pressure; SD, standard deviation; UA, uric acid.
The baseline pathological characteristics of patients based on the renal pathology society classification system (Tervaert et al., 2010) are shown in Table 2. The total of 369 patients included 16 (4%) of class I, 74 (20%) of class IIa, 50 (14%) of class IIb, 165 (45%) of class III, and 64 (17%) of class IV. The interstitial fibrosis and tubular atrophy (IFTA) scores were 0 in 13 patients (4%), 1 in 184 patients (50%), 2 in 127 patients (34%), and 3 in 45 patients (12%). Glomerular classes were distributed similarly in the two groups. Patients in the high-altitude group had less severe IFTA lesions and interstitial inflammation, but these differences were not statistically significant. There were no significant differences in arteriosclerosis or arteriolar hyalinosis scores between the two groups.
Baseline Pathological Characteristics of Patients with Biopsy-Proven Diabetic Nephropathy
Data are presented as the percentages for categorical variables.
Defined by RPS diabetic nephropathy classification.
IFTA, interstitial fibrosis and tubular atrophy; RPS, renal pathology society.
Correlations between clinical and pathological parameters
Baseline hemoglobin concentration was significantly positively associated with altitude (R2 = 0.14, standard β = 0.37, p < 0.001), and eGFR was significantly associated with altitude (R2 = 0.01, standard β = 0.12, p < 0.02). None of the other pathological parameters investigated was significantly associated with altitude (p > 0.05).
Risk factors for progression to ESKD
Of the total 369 patients, 141 (38%) progressed to ESKD during a median follow-up period of 20 months. Figure 1 displays the survival curves of progression to ESKD in all patients. In the low-altitude group 42% of patients progressed to ESKD, but in the high-altitude group it was 17% (p < 0.01). Because the proportion of Han Chinese in the low-altitude group was much higher than that in the high-altitude group, 99% of the patients who progressed to ESKD in the low-altitude group were Han Chinese (Supplementary Fig. S2). In the univariate Cox proportional hazards model, living ≥2,000 m above sea level had a significant effect on renal survival (HR 0.47, 95% CI 0.24–0.92). In univariate Cox proportional hazards analysis, ethnicity, baseline hemoglobin, albumin, eGFR, and proteinuria were associated with ESKD (Fig. 2A). After adjusting for age, sex, baseline serum albumin, hemoglobin, fasting plasma glucose, eGFR, 24-hour proteinuria, renin-angiotensin aldosterone system inhibitor usage, and renal pathological parameters at the time of biopsy, living at a high altitude was not significantly associated with progression to ESKD (HR 0.84, 95% CI 0.38–1.83) (Fig. 2B). When additional adjustment for ethnicity was applied, however, living at a high altitude became an independent risk factor for progression to ESKD (HR 2.83, 95% CI 1.05–7.58) (Fig. 2C). Compared with Han Chinese, Tibetans were at a lower risk of progression to ESKD (HR 0.15, 95% CI 0.04–0.59). Other clinical parameters that were independently associated with progression to ESKD were baseline eGFR, hemoglobin, and albumin concentrations.
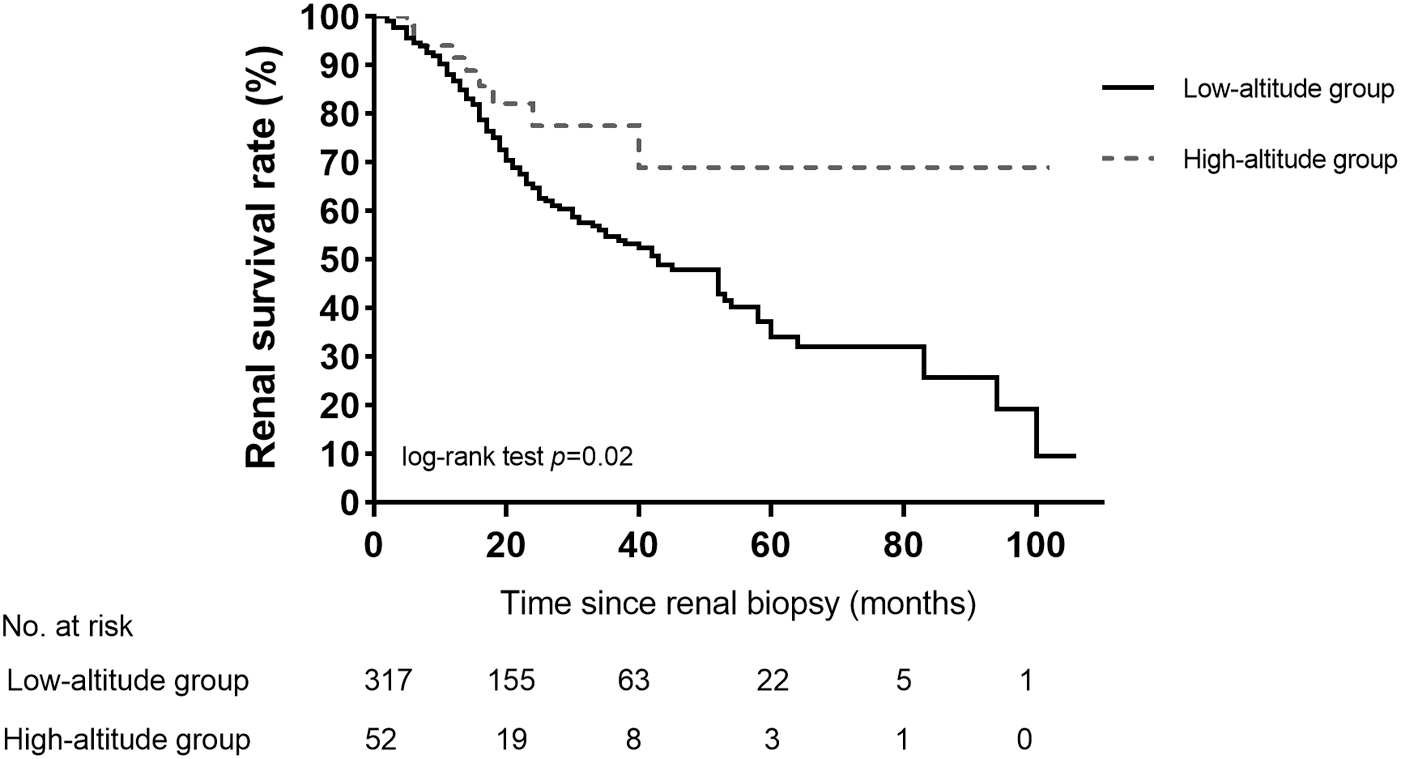
Kaplan–Meier survival curves for end-stage kidney disease stratified by altitude where patients lived. There were significant differences of the renal survival rate between the low-altitude group and the high-altitude group.

Univariate and multivariate Cox proportional hazard models for progression to end-stage kidney disease in 369 patients with type 2 diabetes mellitus.
Han Chinese increased the risk of progression to ESKD. To identify whether living at a high altitude was an independent risk factor in Han Chinese patients, Cox proportional hazard analysis was then applied in 324 Han Chinese with T2DM and DN. When adjusting for the age, sex, renal functions, and renal pathological parameters at the time of biopsy, living at a high altitude was significantly associated with progression to ESKD in Han Chinese (HR 3.36, 95% CI 1.31–8.65) (Fig. 3). However, for the 45 Tibetans, living at a high altitude was not associated with progression to ESKD (data not shown).
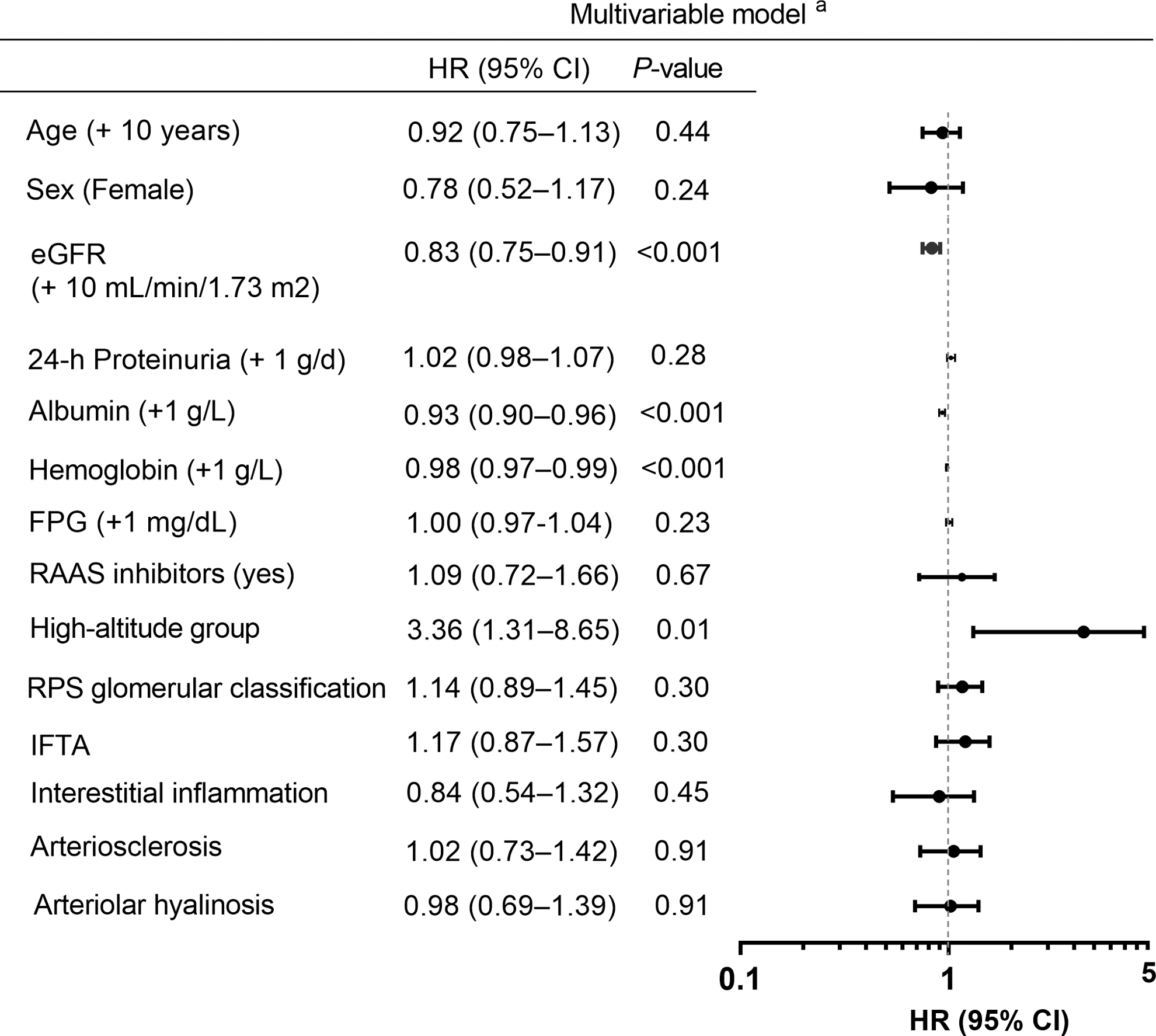
Multivariate Cox proportional hazard models for progression to end-stage kidney disease in 324 Han Chinese patients with type 2 diabetes mellitus. Model a: adjusted for age, sex, baseline estimated glomerular filtration rate, 24-hour proteinuria, serum albumin, hemoglobin, FPG, the usage of RAAS inhibitors, and pathological parameters. In the multivariable Cox proportional hazard model, living at a low altitude was considered as the reference.
Expression of HIF-1α in kidney biopsy specimens by immunohistochemistry
To determine the HIF-1α expression in the kidney, immunohistochemical staining of HIF-1α was carried out on the kidney biopsy specimens from Han Chinese in the low-altitude or high-altitude group. Figure 4 revealed that HIF-1α was slightly deposited in the tubules in Han Chinese who lived at a low altitude, but it was significantly positive in both the tubules and glomeruli in Han Chinese who lived at a high altitude.

Hypoxia-inducible factor-1α staining in kidney biopsy specimens.
Discussion
In this study, living at an altitude of ≥2,000 m above sea level was significantly associated with being Tibetan, and having higher eGFR, BMI, hemoglobin, and HbA1c than those living at lower altitudes. There were no significant differences in renal structural changes between the high-altitude and low-altitude groups. After adjustment for age, sex, baseline albumin, hemoglobin, renal function, pathological parameters, and ethnicity, living at a high altitude was an independent predictor of ESKD in patients with T2DM and biopsy-proven DN if they were Han Chinese, but not if they were native Tibetan. Moreover, lower baseline hemoglobin, serum albumin, and eGFR, and being of Han Chinese heritage increased the risk of progression to ESKD. The results of this study suggest that the genetic adaptability of different nationalities can make a greater contribution to the prognosis of DN in patients living ≥2,000 m above sea level than risk factors such as high-altitude hypoxia, diabetes, and obesity.
The popularity of traveling to mountainous regions and residing in them is increasing, and there is an estimated 415 million people with diabetes worldwide (Zimmet et al., 2016). As a consequence, there is much interest in high-altitude diseases. To our knowledge, this study is the first to investigate relationships between living at high altitude and renal outcomes in patients with biopsy-proven DN. Some previous clinical studies have investigated such associations in CKD patients (Megill et al., 1988; Hochman et al., 2007). Hochman et al. (2007) reported that the rate of ESKD in Navajo Indians living at altitudes of 1,600–3,000 m above sea level was 3.2-fold higher than the rate in the overall population in the United States, and 1.8-fold higher than that in Native Americans overall, most of whom lived at lower altitudes. In another study, the crude prevalence of ESKD among Navajo Indians was three times higher than that among Caucasians in the United States (Megill et al., 1988). Chronic systemic hypoxia associated with long-term residence at high altitude may contribute to kidney progression in patients with pre-existing CKD (Luks et al., 2008), but less is known about relationships between living at high altitude and renal outcomes in patients with DN.
Several factors contribute to the progression to ESKD in diabetic patients who live at high altitudes. Our immunohistochemistry staining of HIF-1α indicated that hypoxia might be one of the reasons. Long-term high-altitude exposure can reportedly result in arterial hypoxemia, which would worsen intrarenal oxygenation in DN patients (Luks et al., 2008). Under hyperglycemic conditions, a diabetic kidney exhibits higher oxygen consumption, due to increased tubular electrolyte transport as well as mitochondrial dysfunction (Laustsen et al., 2014). This increased oxygen consumption renders the kidney hypoxic, which has been proposed as a common mechanism of progression of kidney diseases (Fine et al., 2000). In a diabetic rat model, high altitude increased oxygen consumption and aggravated kidney injury (Laustsen et al., 2014). In this study, living at high altitude was an independent predictor of time to ESKD in Han Chinese patients with T2DM and biopsy-proven DN, but not in native Tibetan patients.
High altitude-mediated hypoxia and kidney injury might relate to a graded increased altitude in mediating changes in hypoxia and kidney injury. Harhay et al. (2016) reported that each 200 m above sea level was associated with a 26% increased odds ratio of CKD incidence in Costa Rica. In our cohort, 80% of patients lived at an altitude between 500 and 1,000 m whereas 75% of patients lived at altitudes between 3,500 and 4,000 m. Owing to the limited number of patients and the uneven distribution of altitude, high altitude was expressed as a binary category, after reviewing the literature regarding biomedical altitude (Betz et al., 2011; Yuwen et al., 2018).
Interestingly, in this study, the median eGFR was higher and the percentage of progression to ESKD was lower in patients who lived at high altitude. This counter-intuitive result may be related to the high prevalence of Tibetans living at high altitude. The higher percentages of ESKD incidence in the low-altitude group were attributed to the high proportion of Han Chinese, who have been shown to increase the risk for progression to ESKD. In the univariate Cox proportional hazards model, living at high altitude with a high proportion of Tibetans reduced the risk of adverse renal outcomes (HR 0.47). After applying ethnicity adjustment to the otherwise fully adjusted model, however, living at high altitude increased the risk of progression to ESKD (HR 2.83). The proteinuria level at the end of follow-up in patients living at high altitude was higher than that in patients living at low altitude (7.08 g/d vs. 5.42 g/d, respectively; data not shown), suggesting severe renal injury among those living at high altitude. The results mentioned earlier indicate that ethnicity plays an essential role in the relationship between altitude of residence and renal outcome.
It is well known that highlanders such as Tibetans have developed unique practices to enable them to survive in challenging environments with limited ecological resources (Okumiya et al., 2016). Han Chinese visitors to high-altitude regions often develop increased hemoglobin concentrations to compensate for the hypoxic environment, and this response is associated with adverse effects (Vargas and Spielvogel, 2006). We have previously reported that high-altitude-induced overexpression of red blood cells via oxygen-sensing pathways in Han Chinese resulted in polycythemia and secondary focal segmental glomerulosclerosis syndrome (Yin et al., 2014). Although Tibetan highlanders have higher hemoglobin levels than Han Chinese, they have genetic polymorphisms that protect them against polycythemia. It has also been reported that Tibetan highlanders exhibited lower hemoglobin concentrations than Andean populations living in similar high-altitude environments (Beall, 2007).
Several genomic analyses suggest that the EPAS1 haplotype and EGLN1 variants are associated with lowering hemoglobin in Tibetans (Simonson et al., 2010). EPAS1 controls the production of HIF-2α and expression of EGLN1, which regulates the production of PHD2, which targets HIF-α subunits for destruction in normoxic conditions—ultimately preventing the transcriptional cascade of hypoxia response genes, including erythropoietin (Simonson et al., 2010). In addition, Tibetans maintain normal aerobic metabolism that is associated with PPARA variants (Moore, 2017). The strong significant associations between hemoglobin concentration and EPAS1, EGLN1, and PPARA haplotype variants is evidence of a genetic contribution to a form of high-altitude adaptation that may be unique to Tibetan populations (Simonson et al., 2010).
In healthy volunteers, glycemic control was improved after short-term high-altitude exposure (Lee et al., 2003), which may be due to the increased glucose uptake and insulin sensitivity exhibited by isolated skeletal muscles as a physiological adaptation. In patients with pre-existing DM in this study, however, HbA1c concentrations were significantly higher in the high-altitude group than in the low-altitude group. This is concordant with previous studies (Allam et al., 2014). Another underlying mechanism of higher HbA1c levels in high-altitude residents may be related to variation in erythrocyte levels. The percentage of HbA1c depends on both the glucose-hemoglobin glycation rate and the time taken for glycation, which, in turn, depend on the ages of red blood cells (Cohen et al., 2008). When individuals were exposed to high altitude, hypoxia reportedly usually caused compensatory increases in hemoglobin concentrations and erythrocytosis (Basu et al., 2007), which may influence the life span of red blood cells and therefore affect HbA1c percentage. Notably, however, higher HbA1c did not affect renal outcomes in Tibetans with DN living at high altitudes.
In this study, the patients who lived at high altitudes exhibited slightly higher BMIs than those who did not. This may be related to the completely different lifestyles of highlanders and non-highlanders. Similar to Andeans, the inhabitants lived in plateau areas and depended on plants and well-adapted animals to generate meals with a high caloric content, and on the intake of large quantities of carbohydrates to meet their energy demands (Mohanna et al., 2006).
To date, there are no reports on the renal pathological characteristics of patients with DN living at high altitude. In a previous study, Henoch-Schonlein purpura was the most common secondary glomerular disease identified via renal biopsy in the Tibetan Plateau region, whereas lupus nephritis was prevalent in the plains region (Zhou et al., 2014). The prevalence of DN was lower in the plateau region than in the plains region. In another study, there was a high prevalence of non-DN in patients with diabetes (Li et al., 2017), which may also affect renal outcomes in patients with diabetes and CKD. Thus, only patients with biopsy-proven DN were enrolled in this study—in which there were no significant differences in glomerular, interstitial, or arteriolar lesions between the high-altitude group and the low-altitude group.
This study had several limitations. Renal biopsies were performed on the basis of clinical indications rather than a research protocol; therefore, there was intrinsic selection bias due to the study's retrospective observational design. Another potential limitation is that all of the patients included were patients of a single center. Notably, however, those who lived at high altitude were randomly and extensively distributed throughout the Tibetan Plateau, Tibetan Region of Sichuan Province, Gannan Tibetan Autonomous Prefecture, and Qinghai Tibet Plateau. These were the areas where the most highlanders were concentrated in China. Further, altitude, expressed as a binary covariate, was used to explore the association between high altitude and renal outcome. Altitude as a continuous and graded exposure was not analyzed in this study. The uneven distribution of patients in the low-altitude and high-altitude groups partly hindered analysis of the risks of graded exposure to altitude with respect to renal outcome. Further multicenter studies with larger prospective cohorts at varying altitudes will be helpful to improve understanding of diabetic kidney injury. A limited sample size of Han Chinese (12) in the high-altitude group and Tibetans (5) in the low-altitude group was another limitation in this study. The residual confounding may affect the association between high altitude and renal outcome, although stratification analysis by ethnicity suggested that living at high altitude was an independent risk factor. Prospective cohorts conducted among patients with diabetes who do not undergo kidney biopsy would provide a larger sample of Han Chinese at high altitude and Tibetans at low altitude, which will be useful to validate our conclusions. Lastly, there were substantial differences between the diets and lifestyles of the high-altitude group and the low-altitude group. Analyses incorporating these two factors were beyond the scope of this study.
In this study, living at a high altitude was an independent predictor of ESKD in patients with T2DM and biopsy-proven DN if they were Han Chinese, but not if they were native Tibetan. Given the uncertainty of the mechanisms involved, we recommend that more research be conducted in Han Chinese populations living at altitudes of ≥2,000 m above sea level.
Footnotes
Acknowledgments
The authors thank Dr. Owen Proudfoot for editing the English text of a draft of this article. They would like to thank the participating patients for their cooperation with this study.
Authors' Contributions
All authors participated in conceiving, designing, and reviewing of this article. L.Z. analyzed the data and interpreted the results. L.Z. drafted the article. F.L. analyzed and interpreted data, edited/revised, and approved the final version of the article. H.X. performed pathological reviewing. L.Z., X.W., T.W., W.F., H.R., R.Z., Y.Z., H.X., J.Z., and Y.W. carried out the data collection and recording, contributed to the discussion. Fang Liu is the guarantor of this work and had full access to all the data in this study, and takes responsibility for the integrity of the data. All coauthors have reviewed and approved of the article before submission.
Author Disclosure Statement
The authors declare no conflicting financial interests.
Funding Information
This study was supported by the projects of the National Natural Science Foundation of China (Grant Nos. 81970626 and 81670662), Key Research and Development Project of Sichuan Science and Technology Department (Grant No. 19ZDYF1273). The funding source played no role in study design, data analysis, and article writing or submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.