
Abstract
Hamm, Wolfgang, Sari Kassem, Lukas von Stülpnagel, Florian Maier, Mathias Klemm, Dominik Schüttler, Felix Grabher, Ludwig T. Weckbach, Bruno C. Huber, Axel Bauer, Konstantinos D. Rizas, and Stefan Brunner. Deceleration capacity and periodic repolarization dynamics as predictors of acute mountain sickness. High Alt Med Biol. 21:417–422, 2020.
Background:
The autonomic nervous system plays an important role in adaptive changes after acute altitude exposure. Periodic repolarization dynamics (PRD) and deceleration capacity (DC) of heart rate are advanced electrocardiogram (ECG)-based parameters reflecting sympathetic (PRD) and parasympathetic (DC) tone. These parameters have not been investigated in the context of acute mountain sickness (AMS) yet.
Methods:
In 23 healthy individuals (13 women), a high-resolution digital 30-minute ECG in Frank leads configuration was performed in a resting supine position at baseline (521 m altitude) and after a sojourn of 24 hours at the Environmental Research Station Schneefernerhaus (UFS) at Zugspitze (2,650 m altitude). PRD and DC were assessed using validated software. Symptoms of AMS were assessed with the Lake Louise Acute Mountain Sickness Score (LLS).
Results:
During altitude exposure, PRD significantly increased from 1.50 ± 1.01 (mean ± standard deviation) deg2 to 3.51 ± 4.46 deg2 (p = 0.03). DC significantly decreased from 11.48 ± 2.91 ms to 9.94 ± 2.78 ms (p = 0.001). An increase of PRD and/or a decrease of DC correlated significantly with the level of LLS. The combined finding of an increase of PRD and a decrease of DC had a sensitivity of 100% and a specificity of 76.5% to diagnose AMS (LLS ≥3). Receiver operating characteristic (ROC) analysis showed an AUC (area under the ROC curve) of 0.77. Linear regression analysis revealed a significant association between LLS and an increase in PRD during high-altitude exposure.
Conclusions:
Our findings show an increase of PRD and a decrease of DC during altitude exposure. Combined PRD and DC analysis may have potential for the diagnosis of AMS.
Introduction
Acute mountain sickness (AMS), the most frequent form of altitude illness, consists of nonspecific symptoms occurring at altitudes ≥2,500 m in unacclimatized individuals. The symptoms typically begin with a delay of 6 to 10 hours after arrival at a new altitude and are most pronounced after the first night of stay at high altitude (Hackett and Roach, 2001).
The autonomic nervous system (ANS) plays an important role in adaptive changes during high-altitude exposure. Several studies have used heart rate variability (HRV) parameters before and after altitude exposure to reveal changes in autonomic tone (Kanai et al., 2001). However, there is only a limited consistency regarding studies on HRV changes at high altitude (Loeppky et al., 2003; Lanfranchi et al., 2005; Boos et al., 2017). Furthermore, most studies describing changes of conventional HRV parameters were performed at altitudes >3,000 m (Loeppky et al., 2003; Lanfranchi et al., 2005; Boos et al., 2017; Sutherland et al., 2017). Therefore, more sensitive parameters of cardiac autonomic tone are needed.
Periodic repolarization dynamics (PRD) is a novel electrocardiogram (ECG)-based parameter likely reflecting the activity of the sympathetic branch of the ANS within the ventricular myocardium. PRD calculation relies on periodic changes of the T-wave vector (Rizas et al., 2014). Clinical trials have shown that PRD is highly predictive for mortality in patients after myocardial infarction and heart failure (Rizas et al., 2014, 2017; Bauer et al., 2019).
Deceleration capacity (DC) of heart rate is a robust ECG-based marker of HRV reflecting predominantly the vagal branch of the cardiac ANS. DC integrates all deceleration-related oscillations of heart rate (Bauer et al., 2006; Rizas et al., 2018). In clinical studies, the prognostic value of impaired DC in predicting mortality after myocardial infarction exceeded that of abnormal standard measures of HRV (Bauer et al., 2006; Rizas et al., 2018).
In this study, we aimed to investigate the association of symptoms of AMS with alterations of cardiac autonomic function by means of the assessment of the sympathetic (PRD) and vagal (DC) tone.
Methods
Twenty-three healthy individuals (13 women) aged 32.7 ± 8.1 years were included in the study. The study protocol was approved by the local ethics committee (Ethikkommission der Medizinischen Fakultät der LMU München). Informed consent was obtained from each patient, and the study protocol conforms to the ethical guidelines of the 2013 Declaration of Helsinki.
In all individuals, a high-resolution digital 30-min ECG (Schiller medilog® AR4plus; Schiller AG Switzerland) was performed in Frank leads configuration in a resting supine position, not talking, and quiet surroundings. Baseline recordings were done in Munich (521 m alt.) 3 hours before the ascent. The ascent was passive via cogwheel train without physical exercise. The second recordings were performed in the Environmental Research Station Schneefernerhaus (UFS) at the Zugspitze (2,650 m alt.) after a sojourn of 24 hours in the UFS. In addition, peripheral oxygen saturation and respiratory rate were measured. All data were acquired at the same time of day (between 9 and 11 a.m.). Individuals were required to abstain from caffeine and alcohol consumption 3 days before and during the study. All individuals were nonsmokers.
DC was assessed as previously described (Bauer et al., 2006; Hamm et al., 2018b): DC is based on a novel mathematical signal analysis method (phase-rectified signal averaging [PRSA]), which transforms complex time series (i.e., heart rate recordings) in a significantly shorter signal. To calculate DC in a first step, heartbeat intervals longer than the preceding interval are defined as decelerating anchors. In a second step, segments around anchors are defined, aligned at the anchors (phase rectification), and averaged (signal averaging) to obtain the PRSA signal. The central part of the PRSA signal is quantified by wavelet analysis to obtain the numerical measure of DC (Fig. 1).
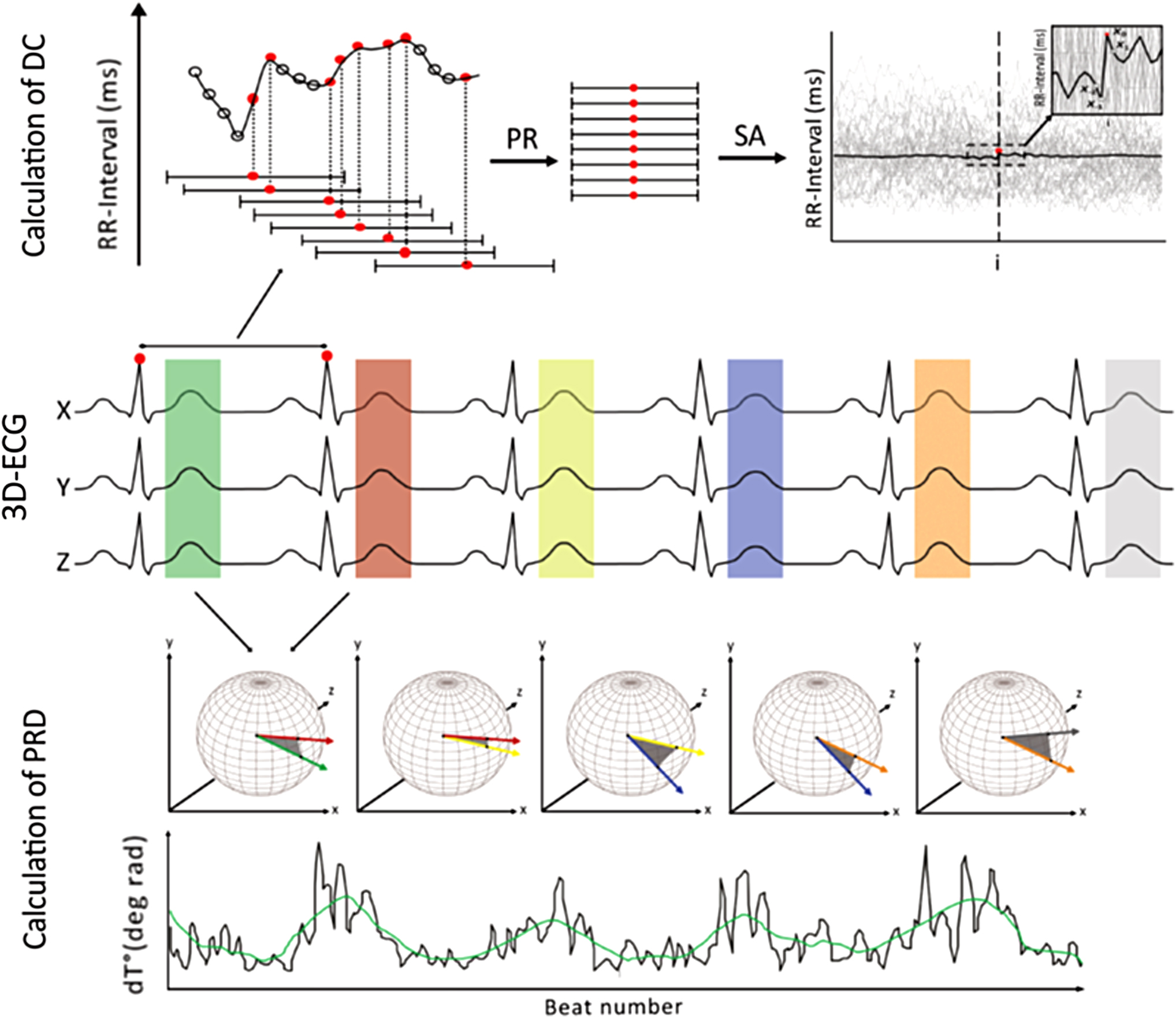
Principle of DC and PRD calculation (adapted from Hamm et al., 2019): DC quantifies dynamics of RR intervals: (1) RR intervals longer than the preceding interval are marked (anchors). (2) Segments are defined and aligned (phase rectified) at the anchors. (3) Signals within aligned segments are averaged (signal averaging). (4) DC is quantified by means of wavelet analysis. PRD quantifies T-vector dynamics: (1) 3D visualization of successive T-wave vectors. (2) The dT° angle between each vector is plotted over time and shows low-frequency oscillations. (3) PRD is quantified by means of wavelet analysis. DC, deceleration capacity; ECG, electrocardiogram; i, index of PRSA signal X(i); PR, phase rectification; PRD, periodic repolarization dynamics; PRSA, phase-rectified signal averaging; RR, interbeat; SA, signal averaging.
PRD was assessed as previously described (Rizas et al., 2014; Hamm et al., 2019): To calculate PRD, the spatiotemporal characteristics of each T wave were mathematically integrated into a single vector T°. The angle dT° between two successive repolarization vectors was calculated and displayed over time, representing the spontaneous fluctuation of instantaneous repolarization instability. Typically, a low-frequency periodic augmentation of dT° can be observed. The spectral properties of the dT°signal were quantified by means of continuous wavelet transformation that provides wavelet coefficients for each scale at each time point. PRD was defined as the average wavelet coefficient corresponding to frequencies of 0.1 Hz or less (Fig. 1).
ECG signals were analyzed using MATLAB with established algorithms for calculation of DC and PRD.
Symptoms of AMS were based on the Lake Louise Acute Mountain Sickness Score (LLS) (Roach et al., 2018). AMS was diagnosed when the Lake Louise AMS score was ≥3 points, including at least 1 point from headache.
Results are expressed as mean ± standard deviation or as median and interquartile range (IQR). For statistical testing, we used the Wilcoxon signed-rank test or paired t-test. Values of p < 0.05 were considered statistically significant. Linear regression analysis was adopted to test the association between Lake Louise Score and the change in vital parameters, as well as change in HRV parameters after high-altitude exposure. We performed receiver operating characteristic (ROC) analysis on the basis of the presence or absence of the following finding: increase of PRD and decrease of DC. The area under the ROC curve (AUC) was calculated using the “R” software. Sensitivity and specificity were derived from the respective two-by-two table.
Results
Mean resting heart rate at baseline was 64.7 ± 8.1 and increased to 67.2 ± 10.0 (p = 0.11) after a sojourn of 24 hours in the high-altitude environment. SpO2 (oxygen saturation as measured by pulse oximetry) decreased from 97.3% ± 1.0% to 94.8% ± 1.8% (p < 0.001), and the respiratory rate increased from 13.1 ± 2.2 to 14.6 ± 3.1 (p = 0.03).
PRD at baseline was 1.50 ± 1.01 deg2 and significantly increased to 3.51 ± 4.46 deg2 (p = 0.03) after 24 hours in the high-altitude environment, DC significantly decreased from 11.48 ± 2.91 to 9.94 ± 2.78 ms (p = 0.001).
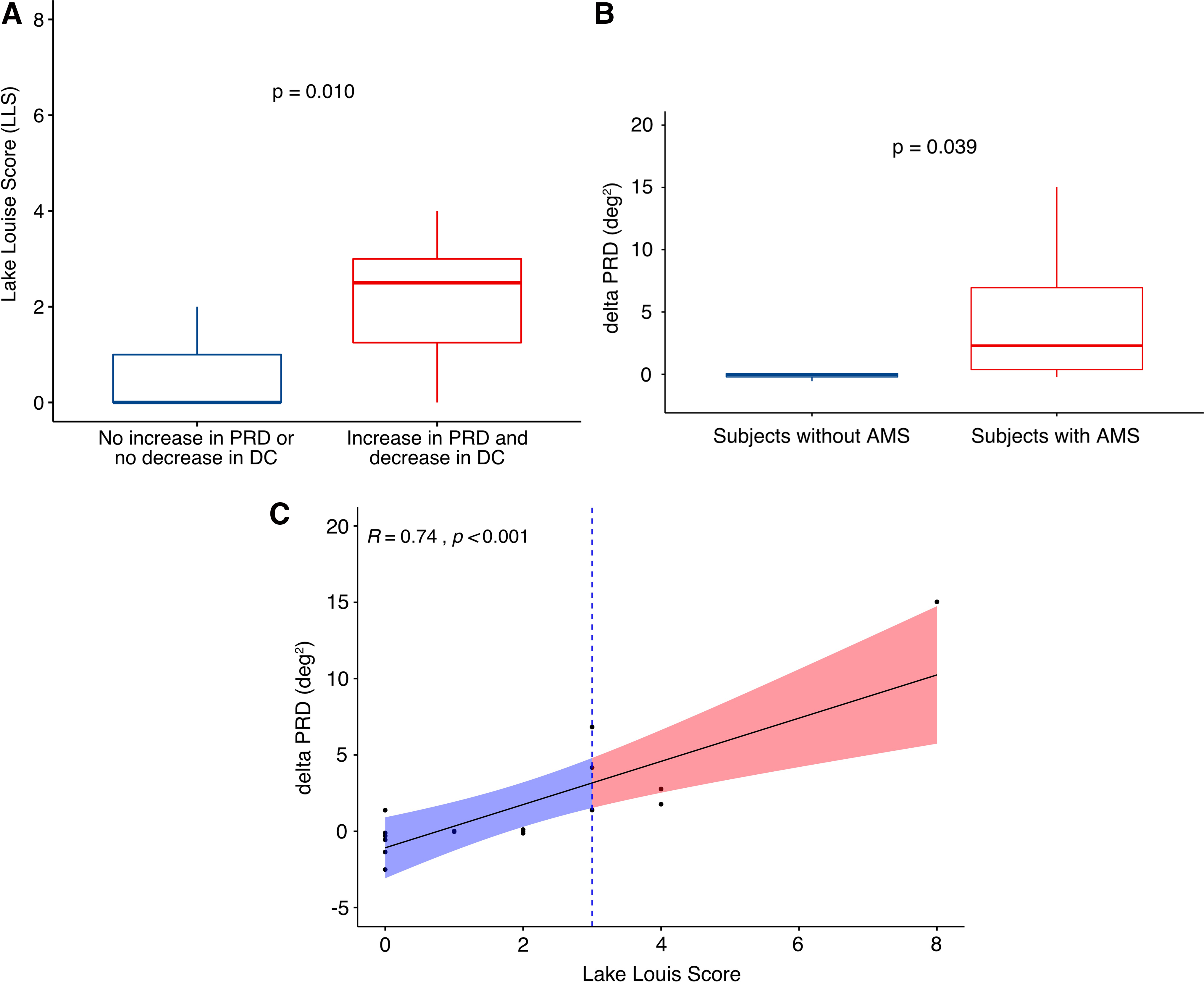
The mean LLS after 24 hours in the high-altitude environment was 1.5 ± 1.9 points with six participants meeting the criteria for AMS. A significantly higher LLS was reported by participants with a decrease of DC (2.0, IQR [0 to 3.0] vs. 0.5, IQR [0 to 1.0] points, p = 0.048) or an increase of PRD (1.5, IQR [0 to 3.0] vs. 1.0, IQR [0 to 2.0] points, p = 0.025) after 24 hours of altitude exposure. The highest LLS was reported by participants with both a decrease of DC and an increase of PRD (2.5, IQR [1.3 to 3.0] vs. 0.0, IQR [0 to 1.0] points, p = 0.001; Fig. 2A). This combined finding of a decrease of DC and an increase of PRD had a sensitivity of 100% and a specificity of 76.5% to diagnose AMS (LLS ≥3). ROC analysis showed an AUC of 0.77. Linear regression analysis revealed a significant association between LLS and increase in PRD after high-altitude exposure (β = 0.240 [95% CI 0.068 to 0.412], p = 0.012, Table 1).
Linear Regression
Lake Louis Score = dependent variable. Covariates represent independent variables.
CI, confidence interval; DC, deceleration capacity; PRD, periodic repolarization dynamics; SpO2, peripheral oxygen saturation.
Participants with AMS (LLS ≥3) and a decrease of DC had significant higher ΔPRD levels (Fig. 2B). In these participants with a decrease of DC, the association between LLS and an increase of PRD levels was highly significant (Fig. 2C).
Standard HRV parameters showed no significant change during altitude exposure. Also, there was no difference between subjects with and without AMS (Table 2). Furthermore, there was no significant correlation between PRD and DC levels with oxygen saturation.
Change of Standard Heart Rate Variability Parameters
Difference of HRV parameters between high-altitude exposure and baseline.
AMS, acute mountain sickness; HF, high frequency; HRV, heart rate variability; HRVi heart rate variability index; LF, low frequency; RMSSD, root mean square of successive differences; SDNN, standard deviation of NN intervals.
Discussion
In the present study, we investigated the association of alterations of the cardiac ANS by means of a combined assessment of the sympathetic (PRD) and vagal (DC) tone with symptoms of AMS. We found a significant increase of PRD and a significant decrease of DC during altitude exposure. Of note, participants with an increase of PRD and/or a decrease of DC had significantly more symptoms of AMS assessed by the Lake Louise Score. The combined finding of an increase of PRD and a decrease of DC had a sensitivity of 100% and a specificity of 76.5% to diagnose AMS (LLS ≥3). Linear regression analysis revealed a significant association between symptoms of AMS and an increase in PRD during altitude exposure.
The physiologic response after altitude exposure is complex and involves several mechanisms and feedback loops. Hence, it is not surprising that results of different studies are not always consistent (Loeppky et al., 2003; Lanfranchi et al., 2005; Huang et al., 2010; Karinen et al., 2012; Wille et al., 2012; Mairer et al., 2013). However, most studies support the concept of a withdrawal of vagal activity as well as an increase of sympathetic activity during altitude exposure. Accordingly, assessment of autonomic tone is of particular importance, especially in high-altitude medicine. Among the noninvasive methods to study the ANS, calculation of HRV is probably the most widely used technique. All methods are based on the principle that sympathetic and parasympathetic activity evokes effects on the cardiovascular system, that is, change of heart rate, vasomotor tone, or cardiac contractility (Rubart and Zipes, 2005). The respective physiological responses result in oscillations of varying frequency ranges, which allow for a noninvasive estimation of autonomic tone.
PRD is a novel ECG-based marker, which is based on low-frequency alterations of cardiac repolarization (Rizas et al., 2014). Although the exact mechanisms underlying PRD are unknown, it is most likely that PRD reflects the effect of the sympathetic nervous system on the ventricular myocardium (Rizas et al., 2016). Increased PRD is highly predictive in various clinical settings (Rizas et al., 2014, 2017; Hamm et al., 2018a; Bauer et al., 2019). Since increased sympathetic activity is one of the main mechanisms leading to AMS, the assessment of PRD offers an excellent diagnostic tool. In our study, increased PRD was significantly associated with symptoms of AMS.
On the contrary, a transient reduction of parasympathetic activity is part of the autonomic response during altitude exposure. In our study, we used DC of heart rate as a robust marker of the vagal branch of the cardiac ANS. Of note, the prognostic power of DC exceeded the conventional ECG-based risk markers in several studies (Bauer et al., 2006; Rizas et al., 2018). In the present study, DC significantly decreased during altitude exposure confirming the results of our previous pilot study (Hamm et al., 2018b). Also, participants with a decrease of DC were more likely to suffer from symptoms of AMS. However, linear regression analysis revealed no significant association between LLS and a decrease in DC after high-altitude exposure.
Despite promising results, this pilot study has limitations. First, the number of participants is low. Second, the altitude exposure was moderate. Therefore, only 26% of participants developed AMS (LLS ≥3). Further studies with exposure to higher altitude levels are needed to validate our approach.
In conclusion, the assessment of cardiac autonomic function by calculating PRD and DC from high-resolution ECG seems a promising approach to identify individuals who suffer from AMS. Since our results were obtained with a limited number of participants at moderate altitude, our findings need to be confirmed with larger cohorts at higher altitudes.
Footnotes
Authors' Contributions
W.H., S.K., and S.B. conceived and designed the research. W.H., S.K., L.v.S., F.M., M.K., D.S., F.G., and S.B. conducted the experiments. W.H., S.K., L.T.W., B.C.H., A.B., K.D.R., and S.B. analyzed the data. W.H. and S.K. wrote the article. All authors have reviewed and approved the article before submission.
Acknowledgments
We are grateful to Monika Baylacher and Gabriele Büschges for supporting the conduction of the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by institutional funds of the Department of Medicine I, University Hospital Munich.