
Abstract
Small, Elan, Nicholas Juul, David Pomeranz, Patrick Burns, Caleb Phillips, Mary Cheffers, and Grant S. Lipman. Predictive capacity of pulmonary function tests for acute mountain sickness. High Alt Med Biol. 22: 193–200, 2021.
Background:
Pulmonary function as measured by spirometry has been investigated at altitude with heterogenous results, though data focused on spirometry and acute mountain sickness (AMS) are limited. The objective of this study was to investigate the capacity of pulmonary function tests (PFTs) to predict the development of AMS.
Materials and Methods:
This study was a blinded prospective observational study run during a randomized controlled trial comparing acetazolamide, budesonide, and placebo for AMS prevention on White Mountain, CA. Spirometry measurements of forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and peak expiratory flow were taken at a baseline altitude of 1,250 m, and the evening of and morning after ascent to 3,810 m. Measurements were assessed for correlation with AMS.
Results:
One hundred three participants were analyzed with well-matched baseline demographics and AMS incidence of 75 (73%) and severe AMS of 48 (47%). There were no statistically significant associations between changes in mean spirometry values on ascent to high altitude with incidence of AMS or severe AMS. Lake Louise Questionnaire scores were negatively correlated with FVC (r = −0.31) and FEV1 (r = −0.29) the night of ascent. Baseline PFT had a predictive accuracy of 65%–73% for AMS, with a receiver operating characteristic of 0.51–0.65.
Conclusions:
Spirometry did not demonstrate statistically significant changes on ascent to high altitude, nor were there significant associations with incidence of AMS or severe AMS. Low-altitude spirometry did not accurately predict development of AMS, and it should not be recommended for risk stratification.
Introduction
Exposure to hypobaric hypoxia can cause acute mountain sickness (AMS), a distressing and often debilitating malady defined by headache in combination with additional symptoms commonly encountered on rapid ascent higher than 2,500 m (8,202 ft) (Roach et al., 1993, 2018).
Risk stratification and prediction models aim at identifying those at risk of developing AMS to reduce morbidity, mortality, and potentially avoid the burden of high-altitude rescue. Various physiologic measurements have been investigated to predict AMS, including hypoxic ventilatory response (Richalet et al., 1988, 2012; Bartsch et al., 2002; Burtscher et al., 2004), 6-minute walk test (Lazio et al., 2010; Shea et al., 2016), arterial oxygen saturation (Burtscher et al., 2004, 2019; Chen et al., 2012; Richalet et al., 2012; Guo et al., 2014), and heart rate variability (Huang et al., 2010; Mellor et al., 2018; Sutherland et al., 2017) without clear support regarding their utility.
Researchers have explored the relationship between the high-altitude hypobaric hypoxia and changes in pulmonary function tests (PFTs) via spirometry, an attractive modality given its simplicity and noninvasive potential insight into the pulmonary effects of high altitude and pathophysiology of AMS (Luks and Hopkins, 2014). The majority of studies report decreases in forced vital capacity (FVC) (Anholm et al., 1979; Pollard et al., 1996; Hashimoto et al., 1997; Mason et al., 2000; Senn et al., 2006), and increases in peak expiratory flow (PEF) (Gautier et al., 1982; Pollard et al., 1996; Cogo et al., 1997; Mason et al., 2000; Deboeck et al., 2005), with variable changes in forced expiratory volume in one second (FEV1) on ascent to high altitude (Selland et al., 1993; Hashimoto et al., 1997; Mason et al., 2000; Cremona et al., 2002). However, other high-altitude studies, including the largest PFT study to date, have found no changes at high altitude with FVC (Cremona et al., 2002; Dehnert et al., 2010), and even transient increases in FVC (Sharma and Brown, 2007).
Though some data suggest a relationship between spirometry and AMS (Anholm et al., 1979; Selland et al., 1993; Cremona et al., 2002), a few have formally assessed their relationship. Limited data support negative correlations between AMS and PEF (Pollard et al., 1996), as well as between FEV1 and FVC (Song et al., 2013). Comparisons of these studies are limited due to varying methodologies, nonstandardized ascent profiles, equipment inaccuracies, and varying definitions of AMS. As such, there is no clear consensus on both the impact of high altitude on lung function measurements (Dehnert et al., 2010; Swenson, 2011; Luks and Hopkins, 2014), and their association with AMS (Mason et al., 2000; Dehnert et al., 2010). The role of the lungs in the hypoxia-driven process of AMS remains controversial, as it is unknown whether the decreased arterial oxygen saturation and observed pulmonary vascular changes act as a driver of altitude illness or downstream casualty (Swenson, 2014; Mairbaurl et al., 2019).
Although a review of the literature reveals an actively ongoing, decade-long discussion regarding spirometric changes at altitude, it also reveals a knowledge gap in the association between spirometry and AMS and the need for larger studies with a systematic AMS definition and standardized ascent profile. Thus, the objectives of this study were to extend prior findings of changes in pulmonary function on ascent to high altitude and association with AMS, and to determine the predictive capacity of pulmonary spirometry for the development of AMS.
Materials and Methods
Study design
This prospective observational study was run concurrently with a double-blind, randomized placebo controlled trial comparing inhaled budesonide, acetazolamide, and placebo for prevention of AMS. The trial was a two-sample comparison of drug versus placebo, with a one-sided alternative analysis of drug to drug, approved by Stanford University School of Medicine and was registered with clinicaltrials.gov (NCT02604173) (Lipman et al., 2018). Participants were enrolled at 1,250 m (4,100 ft), drove to 3,545 m (11,700 ft), and subsequently hiked to and slept at 3,810 m (12,500 ft).
Selection of participants
Participants were selected via a variety of local regional and national distribution e-mail lists. Participants were provided inclusion and exclusion criteria for self-screened eligibility before enrollment. Inclusion criteria included: healthy, resident at low altitude (<1,250 m, 4,100 ft), and ability to complete a moderately strenuous hike. Exclusion criteria included: <18 years or >65 years of age, pregnant or thought to be pregnant, having lived or slept at >1,250 m (4,100 ft) in the past week, having taken diuretics, steroids, acetazolamide, or nonsteroidal anti-inflammatory drugs the week before the study, allergy to acetazolamide, sulfa medications, or corticosteroids; or a hazardous condition that precluded ability to hike to high altitude, including sickle cell anemia, severe asthma or chronic obstructive pulmonary disease, severe anemia, or severe coronary artery disease.
This study was ultimately conducted during the summer of 2016 on White Mountain, California over four weekends. Participants were enrolled in the city of Bishop, California with signed informed consent. Participants were randomized by using a computer-generated random sequence with an allocation of 1:1:1, with the code blinded to administrators and participants.
Data collection and pulmonary function testing
Pulmonary function testing was conducted by using a pneumotachometer (CareFusion Jaeger® Vyntus® SPIRO), which was calibrated with a 3-l syringe. In addition, measurements of barometric pressure, temperature, altitude, and percent humidity were imputed into the testing software (SentrySuite version 2.13). Participants received handouts regarding proper performance of PFT as well as personal coaching on correct performance for each maneuver. Per American Thoracic Society criteria, three reproducible loops were obtained for each time point (Miller et al., 2005). Measurements of FVC, FEV1, and PEF from the best effort as determined by the staff pulmonologist were then collected for eventual analysis.
Data collectors were blinded to treatment groups and AMS scores. PFT measurements were conducted in the morning (8 am–11 am) before ascent, in the evening at least 4 hours after ascent (6 pm–9 pm), and the next morning at high altitude (6.30 am–9.30 am). At the time of the analysis, food intake was not controlled nor the level of exertion. Participants who were unable to complete the study due to AMS had PFT recorded before rescue medications. Diagnosis with AMS was defined by the 1993 Lake Louise Questionnaire (LLQ) score of 3 or greater with the presence of a headache and at least one additional symptom (Roach et al., 1993). The maximum score reached for each participant was used for analysis (Lipman et al., 2018). Severe AMS was defined by an LLQ score greater than 5 (Roach et al., 1993).
Statistical methods
All categorical variables were analyzed by Pearson's χ2 test. Wilcoxon rank-sum test and Welch two-sample t-tests were utilized for spirometry analysis of altitude cohorts. Correlation between PFT and LLQ was investigated by using correlogram analysis. p-Values <0.05 were considered significant, and 95% confidence intervals were used. Prediction modeling was conducted; variable importance for each model was calculated by using a receiver operating characteristic (ROC) for each variable. All analysis was performed by using the R environment for statistical computing version 4.0 (Kuhn, 2020; Team, 2020).
Results
One hundred three participants were analyzed with well-matched comparisons of baseline demographics (Table 1) (Lipman et al., 2018). The cumulative incidence of AMS was 75 (73%) participants, with an incidence of severe AMS of 48 (47%) and mean cumulative LLQ of 4.3 ± 3.1. Acetazolamide reduced AMS by 30% compared with budesonide and 20% versus placebo (Lipman et al., 2018). When PFT was analyzed by drug arm and placebo at high altitude, there were no significant differences (Appendix Tables A1 and A2), allowing them to be combined into a single cohort for analysis (Kanaan et al., 2015; Alsup et al., 2019).
Participant Demographics
Arrival route n = 98, birth country n = 102 as this information was missing from some survey results.
SD, standard deviation.
Mean spirometry values are presented in Table 2. No statistically significant changes were found between mean spirometry values at low altitude baseline, evening of, and morning after ascent (Table 3). In addition, there were no statistically significant associations between changes in mean PFT values with incidence of AMS or severe AMS (Table 4).
Spirometry at Low Altitude (A1), Night of Ascent (B1), and Morning After Ascent (B2)
Sample size was 103 participants.
Indicates sample size 102.
FEF25–75, mean forced expiratory flow between 25% and 75% of the forced vital capacity; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PEF, peak expiratory flow.
Percent Changes in Mean Spirometry Values from Low Altitude Baseline (A) to Evening of Ascent (B1) and Morning After Ascent (B2)
p-Value <0.05 considered significant, sample size was 103 participants.
Indicates sample size 102.
CI, confidence interval.
Association of Changes in Spirometry from Low Altitude Baseline with Acute Mountain Sickness and Severe Acute Mountain Sickness
p-Value <0.05 indicates significance, AMS defined as headache in addition to Lake Louise Questionnaire score ≥3, severe AMS defined as headache plus Lake Louise Questionnaire score >5.
AMS, acute mountain sickness.
Correlogram analysis investigating the relationship between low-altitude spirometry values and high-altitude LLQ scores demonstrated statistically significant slight negative correlations with PEF > FVC > FEV1 the evening of ascent but not the next morning (Fig. 1). When high-altitude spirometry was correlated with LLQ scores, analysis found similar relationships the evening of ascent, which were diminished the next morning at peak altitude (Fig. 2). Prediction modeling for low-altitude PFT to predict eventual AMS yielded 65%–73% accuracy, with an ROC range of 0.51–0.65 between statistical models.
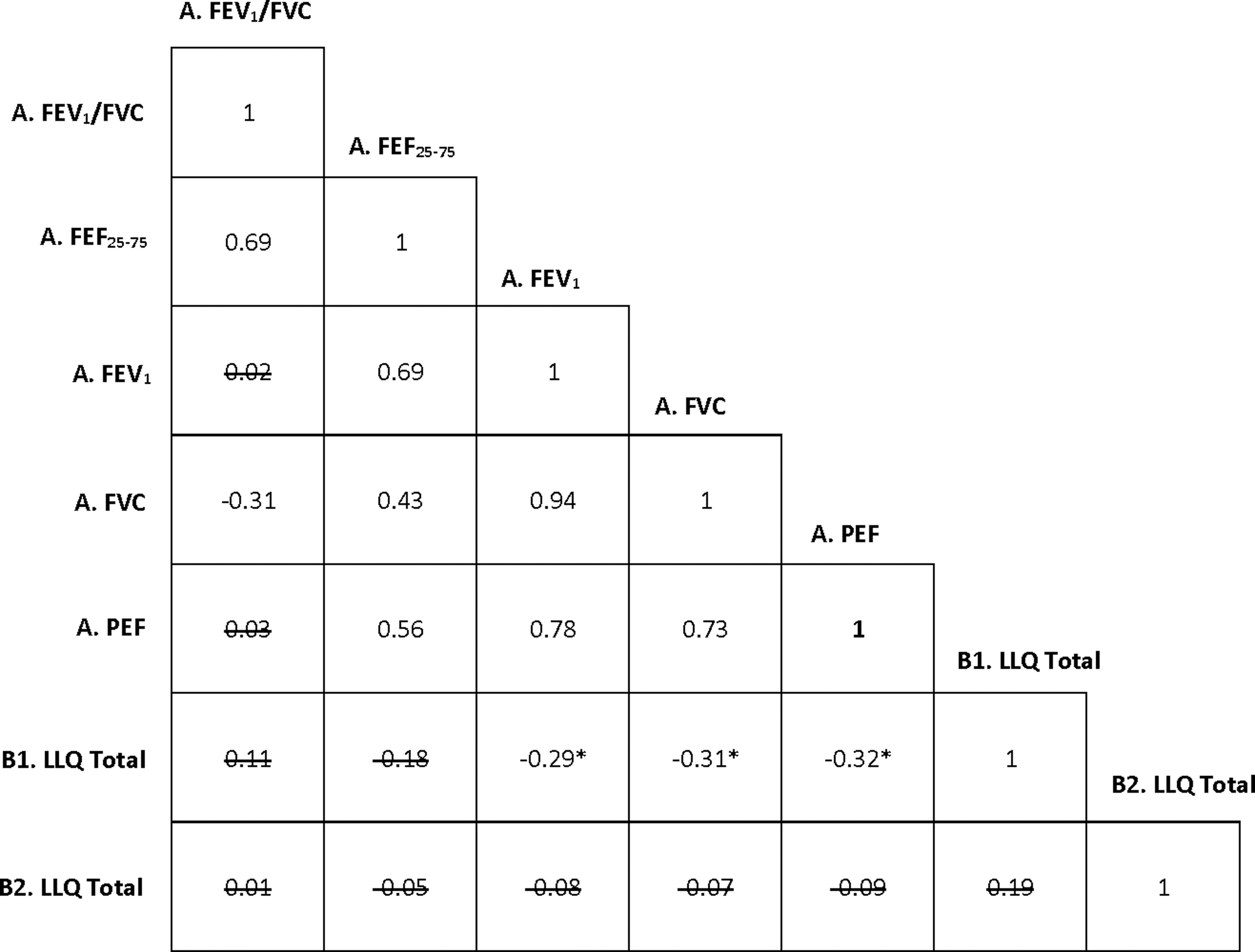
Correlogram of PFTs at baseline low altitude with LLQ scores the evening of and morning after ascent. Strikethrough indicates insignificant values with alpha = 0.05 as marker of significance,* highlighted pertinent values. A, low altitude baseline; B1, evening of ascent to high altitude; B2, morning after ascent to high altitude; FEF25–75, mean forced expiratory flow between 25% and 75% of the forced vital capacity; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; LLQ, Lake Louise Questionnaire; PEF, peak expiratory flow; PFT, pulmonary function test.
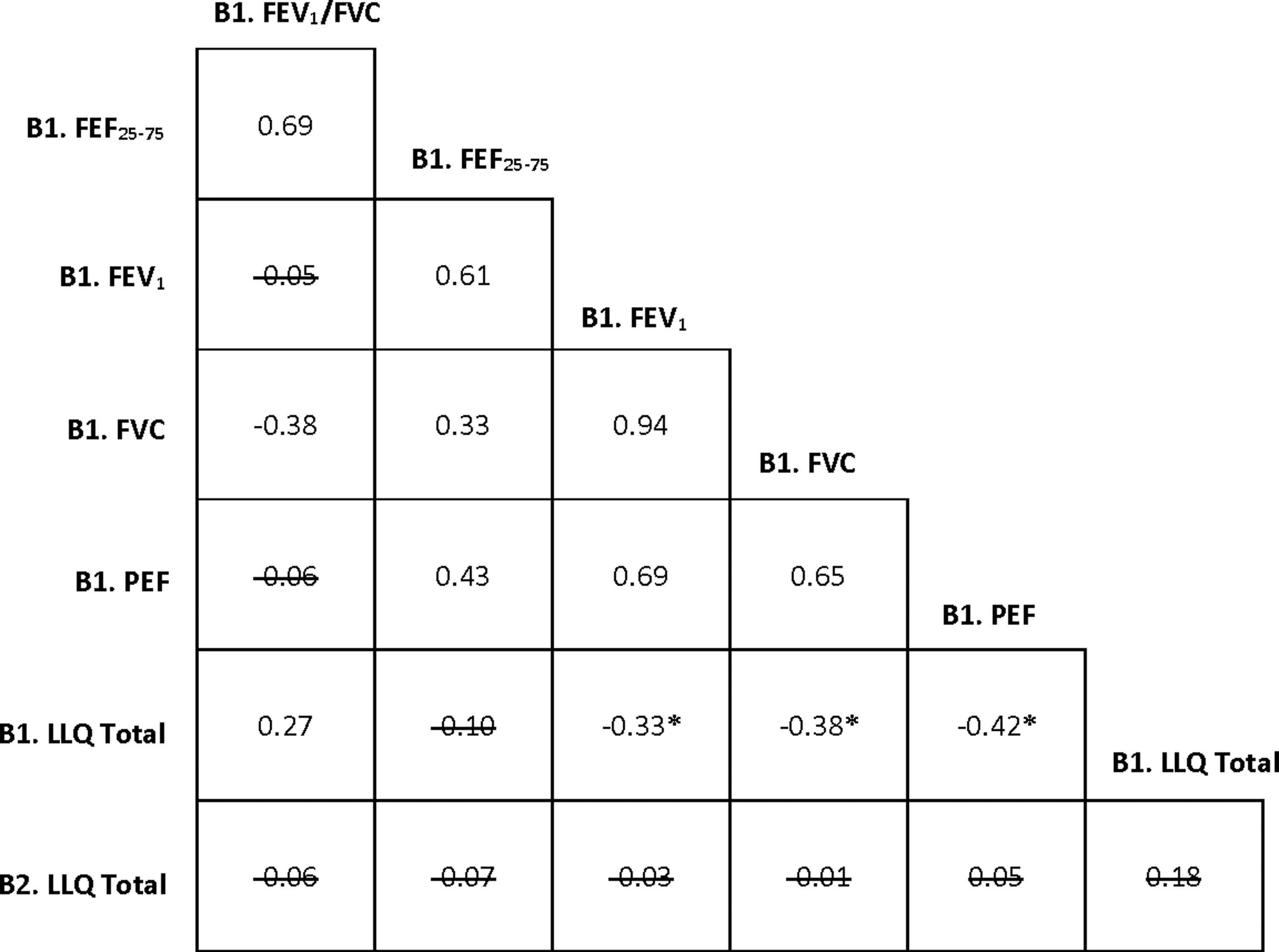
Correlogram of PFTs at evening of ascent with LLQ scores the evening of and morning after ascent. Strikethrough indicates insignificant values with alpha = 0.05 as marker of significance, * highlighted pertinent values. B1, evening of ascent to high altitude; B2, morning after ascent to high altitude.
Discussion
This was the largest study to date to investigate the relationship between PFTs and AMS defined by LLQ criteria. Despite the high incidence of AMS and severe AMS encountered, we did not find a significant association of disease with spirometric changes, consistent with previous investigations (Mason et al., 2000; Dehnert et al., 2010). Though slight negative correlations were found between baseline spirometry and AMS symptom severity reflected in raw LLQ scores the evening of ascent, this relationship diminished the morning after ascent and did not translate into clinically significant AMS. This weak correlation between severity of symptoms per LLQ score and decreased PFT is similar to prior observations (Anholm et al., 1979; Selland et al., 1993), but as the prior research did not systematically quantify AMS symptoms, direct comparisons are challenging.
Our observed lack of any statistically significant association of AMS with PFT changes contrasts a similar-sized military manuscript (Zhou et al., 2004), but any insights into methodological differences are limited due to its unavailability. Though larger sample sizes have been studied (Cremona et al., 2002), the largest study with comparative AMS definitions and spirometry did not analyze PFT outcomes per AMS incidence or severity (Zheng et al., 2014). They too examined oral and inhaled chemoprophylactic AMS medications, and similarly found no significant impact of medicines versus placebo on PFT other than Δ FVC in one arm. However, the authors' primary pharmacologic outcomes were subsequently unverifiable (Berger et al., 2017; Lipman et al., 2018). Likewise, we did not find significant changes in PFT on ascent in either drug, nor when limiting the analysis to just the placebo group, which further supports our conclusions. With a weak predictive accuracy of all pulmonary testing variables, our results support that PFT is a poor predictor of AMS.
In the decade-old body of spirometry literature, many studies, though methodologically sound, involved relatively small populations (Gautier et al., 1982; Selland et al., 1993; Hashimoto et al., 1997; Sharma and Brown, 2007), making definitive associations between spirometry and AMS difficult to demonstrate. Though debated (Swenson, 2011), spirometric derangement at altitude may suggest the presence of sub-clinical interstitial pulmonary edema which has been demonstrated at high altitude (Welsh et al., 1993; Cremona et al., 2002; Alsup et al., 2019), and postulated to be associated with higher rates of AMS (Cremona et al., 2002). Pulmonary edema in AMS is supported by lung ultrasound findings and pulmonary oxygen diffusion changes (Ge et al., 1997; Alsup et al., 2019). However, the statistical significance of these ultrasound changes (from the same cohort) was very slight (Alsup et al., 2019), which could reasonably correspond to a lack of observed significant associations between PFT and AMS.
Changes in PFT on ascent to high altitude would ideally be examined through a mechanistic lens; however, the causative physiology is poorly understood and proposed theories for observed changes have been historically conflicted. Early literature postulated that cold-induced broncho-constriction may have contributed to decreased FVC, though this was largely disproven with bronchodilators (Hashimoto et al., 1997). It was proposed that sub-diaphragmatic gas expansion from hypobaria or hypoxia-driven respiratory muscle fatigue contributes to decreases in FVC (Rahn and Hammond, 1952; Finkelstein et al., 1965; Deboeck et al., 2005), although both theories have been opposed (Tenney et al., 1953; Sharma and Brown, 2007). The largest high-altitude PFT cohort failed to demonstrate significant changes in FVC on ascent (Cremona et al., 2002); however, the next largest study published nearly a decade later produced contrary results, further complicating consensus (Zheng et al., 2014).
Contributing to the heterogeneity and limiting comparisons are methodological discrepancies in the peak altitude reached, speed of ascent, length of high-altitude exposure and consequential extended time course of spirometry measurements, lack of AMS as primary outcome, and a myriad of uncontrollable environmental variables in the case of field studies—all of which may contribute to pulmonary function at high altitude. As such, spirometry is unlikely to advance our understanding of AMS.
Limitations
This study was concurrently run during an ongoing randomized controlled trial investigating acetazolamide and inhaled budesonide versus placebo for the prevention of AMS. Though our analysis did not find any statistically significant spirometric differences between cohorts, it is inherently possible that interventions introduced slight changes in spirometry. Our convenience sample included mostly Californian residents, with roughly 70% white participants, potentially limiting generalizability. In addition, though our study design attempted to avoid preacclimitization by excluding high-altitude exposure in the past week, some lingering effect of preacclimatization cannot entirely be excluded. Level of exertion was not controlled for and thus, similarly, resultant effects on spirometry cannot entirely be excluded.
This study utilized the 1993 LLQ scoring, which was current at the time of data collection. However, the definition of AMS has since been updated (Roach et al., 2018). This discrepancy has been investigated previously at this clinical site where the original 1993 definition of AMS has been demonstrated to be 96% accurate when compared with the 2018 LLQ (Lipman et al., 2019), suggesting the generalizability of our findings in accordance with the newer definition. Lastly, measurements were taken at baseline and altitude; our findings may have been strengthened by more frequent spirometric measurements.
Conclusions
Spirometry did not demonstrate statistically significant changes on ascent to high altitude, nor with the development of AMS or severe AMS. Low-altitude spirometry was not a useful predictor for the development of AMS and should not be recommended for risk stratification of potential disease.
Footnotes
Authors' Contributions
E.S., C.P., and G.S.L. had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. All authors were responsible for data collection, data analysis, and/or interpretation. N.J., D.P., and G.S.L. were responsible for design and conduct of the study. All authors were responsible for the preparation, review, and approval of the article. E.S. takes responsibility of the article as a whole. All authors reviewed and approved of the article before submission.
Acknowledgments
The authors are grateful to all the participants who enrolled in this project, and their enthusiasm for the mountains made this study feasible. They are also grateful to Drs. Kristina Evans and Carrie Jurkiewicz for their assistance in collecting data and Dr. Peter Hackett for his editorial input.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was made possible by the generous support from the Wilderness Medical Society's Herbert N. Hultgren grant by the Academy of Wilderness Medicine®, the American Alpine Club, and the Institute for Altitude Medicine.
Appendix
Spirometry Morning After Ascent by Study Arm
| Variable | Placebo, mean (SD) | Budesonide, mean (SD) | Acetazolamide, mean (SD) | Difference between acetazolamide and placebo, p (95% CI) | Difference between budesonide and placebo, p (95% CI) | Difference between acetazolamide and budesonide, p (95% CI) |
|---|---|---|---|---|---|---|
| FVC, l N (%) |
4.5 (0.8) 32(31) | 4.7 (1.2) 31 (30) | 5 (1.1) 34 (33) |
0.1 (−0.03 to 0.9) | 0.7 (−0.4 to 0.6) | 0.3 (−0.3 to 0.9) |
| FEV1, l N (%) |
3.8 (0.7) 32 (31) | 3.8 (0.8) 31 (30) | 4.1 (0.9) 34 (33) |
0.1 (−0.02 to 0.7) | 0.8 (−0.3 to 0.4) | 0.1 (−0.1 to 0.7) |
| PEF, l/s N (%) |
9.3 (1.8) 32 (31) | 9.5 (2.0) 31 (30) |
10 (2.2) 34 (33) |
0.2 (−0.3 to 1.7) | 0.8 (−0.8 to 1.1) | 0.3 (−0.5 to 1.6) |
| FEV1/FVC N (%) |
83.1 (6) 32 (31) | 83 (7.5) 31 (30) |
83 (5.8) 34 (33) |
0.9 (−3.2 to 2.6) | 1.0 (−3.5 to 3.4) | 0.9 (−3.6 to 3.2) |
| FEF25–75 N (%) |
4.1 (1.2) 32 (31) | 4.2 (1.2) 31 (30) |
4.4 (1.2) 34 (33) |
0.4 (−0.33 to 0.83) | 0.9 (−0.6 to 0.6) | 0.5 (−0.4 to 0.8) |
p < 0.05 indicates significance.