
Abstract
Sherpa, Mingma Thsering, and Raksha Shrestha. Stroke at high altitude in an experienced Sherpa climber: A case report. High Alt Med Biol. 21:406–408, 2020.—A 44-year-old experienced Sherpa climber had dizziness with nausea and several episodes of vomiting while at Camp 2 of Mount Everest (6400 m). He was airlifted from Everest Base Camp to Kathmandu for further treatment. Neurological assessment revealed cerebellar signs with ataxia. Sensory examination revealed hypoesthesia on the extremities of the left side and right half of the face. Laboratory workup revealed increased hemoglobin and hematocrit levels. Magnetic resonance imaging of brain revealed ischemic infarction of right cerebellar hemisphere in the right posterior inferior cerebellar artery territory extending to medulla. Patient was managed with aspirin, supportive measures, and physiotherapy, and made a complete recovery after 2 months. This is the first documented case of ischemic stroke in a healthy experienced Sherpa climber. Although the exact cause of stroke in our patient remains uncertain, the prothrombotic state due to high altitude compounded by impaired cerebral autoregulation and dehydration may have been contributory factors.
Case Report
A 44-
The next morning, he was airlifted from the Everest Base Camp to Kathmandu (1400 m) for further treatment. On initial assessment he was afebrile, with blood pressure of 100/70 mmHg, pulse rate of 58/min, and SpO2 of 94% on ambient air. Neurological assessment revealed cerebellar signs with ataxia. Sensory examination revealed hypoesthesia of the extremities of the left side and right half of the face. Motor examination was normal. There were no signs of meningeal irritation and cranial nerves were intact. Respiratory, cardiovascular, and abdominal examinations were unremarkable. Laboratory investigations revealed hemoglobin of 20.1 g/dL and hematocrit level of 62.8%. Magnetic resonance imaging of brain was suggestive of ischemic infarction of right cerebellar hemisphere in the right posterior inferior cerebellar artery territory extending to medulla (Figs. 1 and 2). Conservative treatment was started with aspirin, a statin, supportive measures, and physiotherapy. During his hospital stay, he developed hoarseness and nasopharyngolaryngoscopy was suggestive of a right vocal cord palsy possible secondary to his stroke (Fig. 3). The patient improved significantly for the duration of 3 weeks with physiotherapy and rehabilitation. After 2 months of follow-up visits and rehabilitation he made a complete recovery.
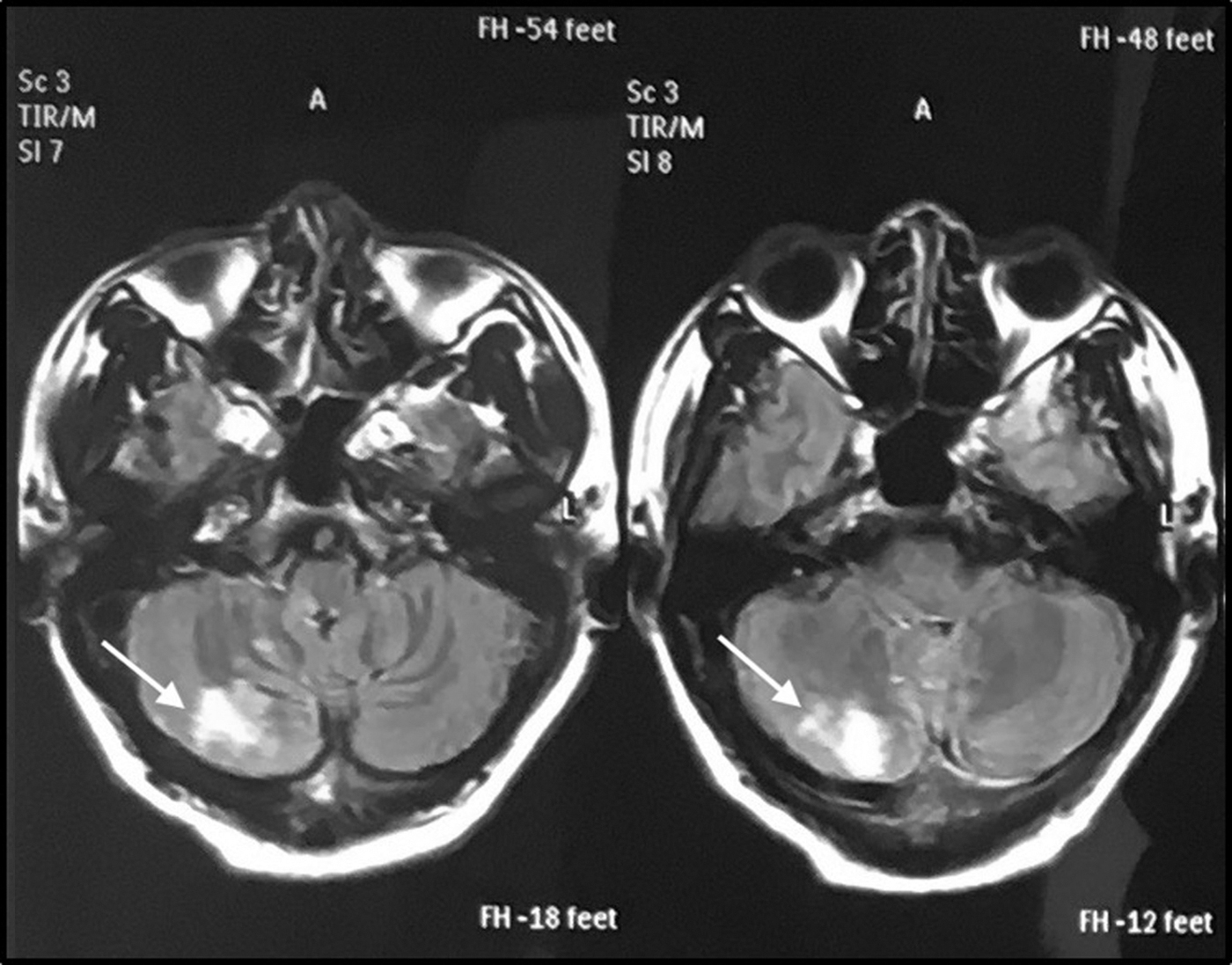
Axial T2-weighted slice through the brain showing high signal intensity lesion in the right cerebellar hemisphere (arrow) with restriction of diffusion suggestive of acute infarct.
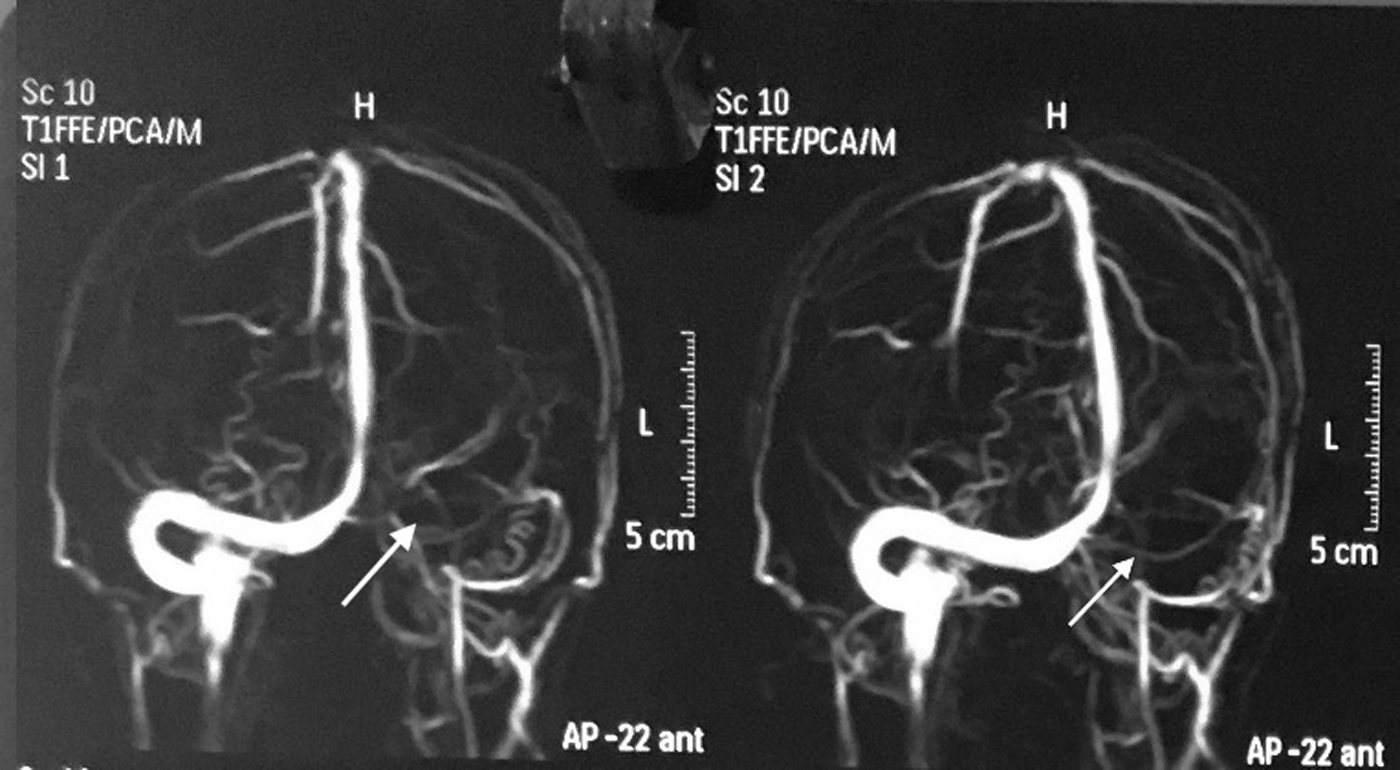
Loss of signal in left transverse sinus (arrow), sigmoid sinus, and left internal jugular vein suggestive of venous thrombosis with markedly atrophied left-sided venous system.
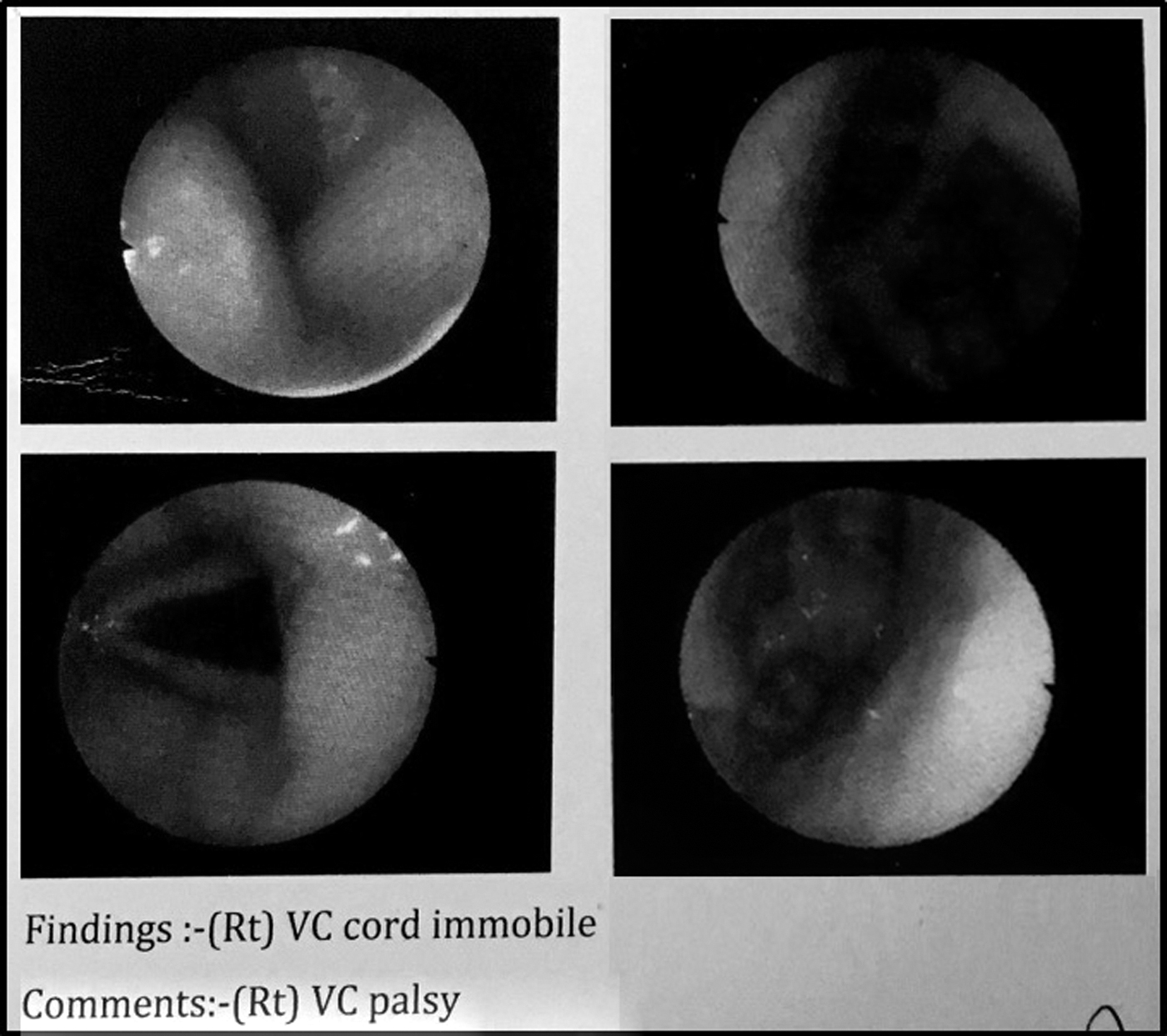
Nasopharyngolaryngoscopy showing immobile right vocal cord (arrow) suggestive of right vocal cord palsy.
Discussion
Stroke at high altitude have been reported in the published literature (Beall and Reichsman, 1984; Jha et al., 2002; Wheatley et al., 2011); however, none among the Sherpas residing at high altitude. Sherpas are known to be elite climbers due to their genetic adaptation to high altitude (Bhandari and Cavalleri, 2019). In this study, we report the first case of stroke in an experienced Sherpa climber. He is a permanent resident of Khumbu (Sherpa village) at 3800 m in Nepal. He started his career as a mountain climber at the age of 16. Since then he had summited Mount Everest uneventfully 16 times and hence can be regarded as a highly experienced veteran climber.
Hypobaric hypoxia at high altitude stimulates erythropoietin secretion resulting in increased red blood cell production, hematocrit, and hemoglobin concentration. This together with decreased plasma volume may lead to a prothrombotic state (Wheatley et al., 2011). Polycythemia was an important risk factor for ischemic stroke in soldiers based at high altitude (>4000 m) for many months (Jha et al., 2002). However, it is difficult to ascertain the events that led to the stroke in our patient as studies have shown that compared with the lowlanders, the Sherpa population residing at high altitudes have lower hemoglobin concentration (Beall and Reichsman, 1984). This is attributed to a blunted erythropoietic response or other factors that affect the hemoglobin concentrations (Bhandari and Cavalleri, 2019). A possible cause for his high hemoglobin concentration may be explained by dehydration and less likely due to high altitude given his genetic heritage, experience as a climber, and his permanent residence above 3000 m.
Cerebral autoregulation (CA) is a sensitive mechanism that plays an important role in maintaining a constant blood supply to the brain and its role in ischemic stroke has also been implicated. Although it is assumed that high altitude residents have preserved CA, Jansen et al. (2000) found that it was impaired at high altitude even in Sherpas when compared with lowlanders at high altitude; the underlying reason still remains elusive.
Neurological problems at altitude are not uncommon at high altitude and may mimic acute altitude sickness (Basnyat et al., 2000). High altitude cerebral edema (HACE) is the most common differential diagnosis of neurological deficit at high altitude and usually presents with global neurological deficits, whereas focal neurological deficits are less common. However, HACE may also present with reversible focal neurological deficit mimicking stroke (Yanamandra et al., 2014). Although it may be difficult to diagnose stroke in a high-altitude setting, portable ultrasound with transcranial Doppler can aid in the diagnosis of stroke (Wilson et al., 2011).
This is the first documented case of an ischemic stroke in a healthy experienced Sherpa climber. Although the exact cause of his stroke remains uncertain, the prothrombotic state due to high altitude compounded by impaired CA and dehydration may have been contributory factors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.