
Abstract
García, Iker, Franchek Drobnic, Casimiro Javierre, Victoria Pons, and Ginés Viscor. Severe hypoxic exercise does not impair lung diffusion in elite swimmers. High Alt Med Biol. 22:90–95, 2021.
Background:
Exercise performed at high altitude may cause a subclinical pulmonary interstitial edema that can worsen gas exchange function. This study aimed to evaluate whether there are changes in alveolar–capillary diffusion after exercise during a short-term exposure to hypobaric hypoxia in elite swimmers.
Materials and Methods:
Seven elite swimmers (age: 20.4 ± 1.4 years, height: 1.78 ± 10.8 m, body mass: 69.7 ± 11.1 kg) participated in the study. Diffusing capacity of the lungs for carbon monoxide (DLCO), transfer coefficient of carbon monoxide, pulse oximeter oxygen saturation (SpO2), and heart rate (HR) were measured at sea level at rest (SL-R), and after a short-term hypobaric hypoxia exposure (4,000 m), both at rest (HA-R) and at the end of moderate interval exercise (HA-E).
Results:
The combined exposure to high altitude and exercise did not change DLCO from SL-R to HA-R, or HA-E (43.8 ± 9.8 to 41.3 ± 10.5 to 42.4 ± 8.6 ml minutes−1 mmHg−1, p = 0.391). As expected, elite swimmers showed large decrease in SpO2 (72 ± 5; p < 0.001) and increase in HR (139 ± 9 beats minutes−1; p < 0.003) after HA-E.
Conclusions:
An acute high-altitude exposure combined with submaximal exercise does not change alveolar-capillary diffusion in elite swimmers.
Introduction
Evidence is accumulating on the growth limitations of the pulmonary system as fitness level increases (Sheel et al., 2004). Endurance training does not improve the structural and functional properties of the lungs to the same extent as the cardiovascular or muscular system in land-based athletes (Dempsey, 1986; McKenzie, 2012). However water-based athletes, such as swimmers, have larger lungs and higher diffusing capacity than other athletes (Armour et al., 1993; Mickleborough et al., 2008) probably because of repeated exposure to mechanical strain and hypoxia during swimming (Wagner, 2005).
Altitude training camps are extensively utilized by elite swimming coaches (Lundby and Robach, 2016), but the possible modifications of the alveolar–capillary exchange are still unknown. Under severe altitude exposure and/or high-intensity exercise, the O2 delivery to active tissues may not be sufficient to ensure an adequate function, leading to hypoxemia (Naeije and Chesler, 2012), diffusion limitation (Mairbäurl et al., 2019), and lung interstitial edema (Anholm et al., 1999; Eldridge et al., 2006; Marabotti et al., 2017). In particular, the practice of swimming has been associated with the occurrence of pulmonary edema (Hohmann et al., 2018), with a specific denomination (swimming-induced pulmonary edema, SIPE).
Different modalities of altitude training have been proposed although Living High—Training High protocol is still the most feasible modality among swimmers (Rodríguez et al., 2015). However, the application of intermittent hypoxic exercise in hypobaric hypoxic chamber or normobaric hypoxic tents at severe altitude (>3,000 m) are becoming popular among elite athletes to enhance exercise performance (Viscor et al., 2018). The exposure to severe hypoxia may provoke changes in the diffusing capacity of the lungs for carbon monoxide (DLCO), although there are no consensus about the conditions needed to provoke these changes in lung diffusing parameters (Clarenbach et al., 2012; de Bisschop et al., 2012; Taylor et al., 2016; Coffman et al., 2017). Recently, we showed that a session of moderate cycling at normobaric hypoxia (3,000 m) during a 14-day altitude training camp at moderate altitude (1,850 m) acutely decreases DLCO in elite swimmers (García et al., 2020).
As a result of these new approaches in hypoxic training (Viscor et al., 2018), the main goal of this study was to evaluate the lung diffusing response during exercise under acute hypobaric hypoxia exposure in unacclimated elite swimmers. These include exposures of this kind to exercise at high altitude while they reside at sea level. So we aimed to evaluate the possible changes in DLCO after a short-term bout of exercise at 4,000 m high altitude (HA). We evaluate DLCO at rest at sea level (SL-R), and then at 4,000 m, both at rest (HA-R) and after moderate intensity interval exercise (HA-E). We hypothesized that there will be an increase in lung diffusion at rest in HA (HA-R) due to a recruitment and distension of the pulmonary vasculature, but there will be a decrease after exercise at HA (HA-E) because of an accumulation of interstitial fluid.
Materials and Methods
Participants
Seven elite swimmers, including two women and five men, were the participants of the study (age: 20.4 ± 1.4 years, height: 1.78 ± 10.8 m, body mass [BM]: 69.7 ± 11.1 kg). The participants had an average FINA (Fédération Internationale de Natation) points in their best event of 781 FINA points at the time of the study and five of them have participated in European and World junior championships. The training schedule of the swimmers were composed of 10 swimming training sessions and 5 dry land sessions per week, amounting to 25 hours of training per week. None of them had asthma and none were smokers.
Experimental design
The study was performed in a hypobaric chamber sited at the University of Barcelona. The participants performed two DLCO measurements before the start of the study to become familiar with the procedure. A cycle ergometer (Corival Lode BV, Groningen, the Netherlands) was used to do the exercise protocols, and a computerized spirometer (Easy One Pro; ndd Medical Technologies, Zurich, Switzerland) was used to evaluate DLCO and other pulmonary parameters.
Lung diffusing capacity was evaluated in relation to exercise during a short-term exposure to hypobaric HA at 4,000 m. The participants performed a basal measurement in resting condition at sea level (SL-R). They reached the target barometric pressure of 462 torr (equivalent to 4,000 m of altitude) in the hypobaric chamber in a time lapse of 30 minutes of pressure stabilization. Then, measurements were performed in a resting condition at high altitude (HA-R), and immediately at the end of 30 minutes of moderate interval exercise at the same high altitude (HA-E). The exercise interval protocol consisted of five sets with 3 minutes at moderate intensity (2 W per kilogram of individual BM; 139 ± 23 W) and 3 minutes of active recovery (25 W). The computerized spirometer used to measure DLCO was placed within the hypobaric chamber during the HA measurements. The subjects were instructed to perform the DLCO maneuver <1 minute after the exercise. Exercise at HA was monitored by pulse oximeter oxygen saturation (SpO2) and heart rate (HR) to ensure an optimal health status during exercise.
All measures considered in this study were “grade A” maneuvers, as identified by the system (Graham et al., 2017). In addition, the hemoglobin (Hb) concentration was determined from a small blood sample obtained by venepuncture to adjust DLCO to individual parameters before the beginning of the study and DLCO was also corrected to actual barometric pressure (DLCOadj) in the HA-R and HA-E conditions.
Pulmonary function measurements
The procedure used to obtain diffusion lung capacity parameters was the single-breath method, for which a computerized spirometer was attached to a gas mixture cylinder. This method involves measuring the uptake of CO from the lungs over a short breath-holding period. The recommendations made in a recent joint statement by the American Thoracic Society (ATS) and the European Respiratory Society (ERS) were followed (Graham et al., 2017).
The participants were placed in a seated position, with a mouthpiece and nose-clip in place throughout the test procedure. The test started with tidal breathing for two to four breaths until the subject felt comfortable with the mouthpiece. Then the DLCO maneuver began with an unforced exhalation to residual volume (RV). At RV the subject's mouthpiece was connected to the source of test gas, and the subject inhaled rapidly to maximal inspiration. After that, the participant was asked to hold their breath for 10 seconds and then exhale completely without interruption in <4 seconds and to continue with a tidal breath to finish the test.
The test gases mixture used to calculate pulmonary function and diffusion capacity was composed of 0.3% of carbon monoxide (CO), 11% of a tracer inert gas (He) used to measure alveolar volume (VA) and the initial alveolar CO, a mixture of 20.9% of oxygen (O2), and the rest was nitrogen (N2). In addition to DLCO and VA, transfer coefficient of the lung for carbon monoxide (KCO), total lung capacity, vital capacity inspired, and RV were calculated.
Ethics
The study was developed in accordance with the Declaration of Helsinki concerning the ethical principles of human experimentation and approved by the Institutional Ethical Committee from the University of Barcelona (Institutional Review Board no. IRB00003099), in accordance with current Spanish legislation. The participants were informed and familiarized with all the experimental procedures, as well as the risks and benefits of the study. They signed an informed consent form and were free to withdraw from the experimental protocol at any time.
Statistical analysis
Data are reported as mean values ± standard deviation. Differences in pulmonary parameters among different conditions (SL-R, HA-R, and HA-E) were analyzed using a one-way repeated-measures analysis of variance (ANOVA), and in case of detecting statistical effects (p < 0.05), Bonferroni corrections were performed. Effect sizes as partial eta-squared (
Results
Basal lung capacity and diffusing capacity of elite swimmers were higher than predicted by age and height, including DLCO (139% ± 6%), KCO (120% ± 7%), and VA (116% ± 8%).
Table 1 provides the response in pulmonary functional and structural parameters to HA conditions. At the hypobaric chamber, there were no differences between SL-R, HA-R, and HA-E in any of the main pulmonary parameters evaluated such as DLCOadj (43.8 ± 9.8 to 41.3 ± 10.5 to 42.4 ± 8.6 ml min−1 mmHg−1, p = 0.319), KCOadj (6.02 ± 0.48 to 5.79 ± 0.52 to 5.77 ± 0.84 ml min−1 mmHg−1 l−1, p = 0.541), and VA (7.22 ± 1.34 to 7.10 ± 1.57 to 7.31 ± 0.92 l, p = 0.787).
Pulmonary Parameters of Swimmers and Control Subjects Under Different Environmental and Exercise Conditions: Sea Level at Rest, Simulated High Altitude at Rest and Simulated High Altitude Immediately at the End of Exercise
Significantly different than SL-R (p < 0.05). †Significantly different than HA-R (p < 0.05).
DLCO, diffusing capacity of the lungs for carbon monoxide; DLCOadj, DLCO was also corrected to actual barometric pressure; HA-E, high altitude immediately at the end of exercise; HA-R, high altitude at rest; KCO, transfer coefficient of carbon monoxide; RV, residual volume; SL-R, sea level at rest; TLC, total lung capacity; VCIN, vital capacity inspired; VA, alveolar volume.
Figure 1 shows the response in the cardiovascular parameters during the different conditions studied and Figure 2 shows the individual changes in SpO2, HR, and DLCOadj from HA-R to HA-E in the sample of elite swimmers.
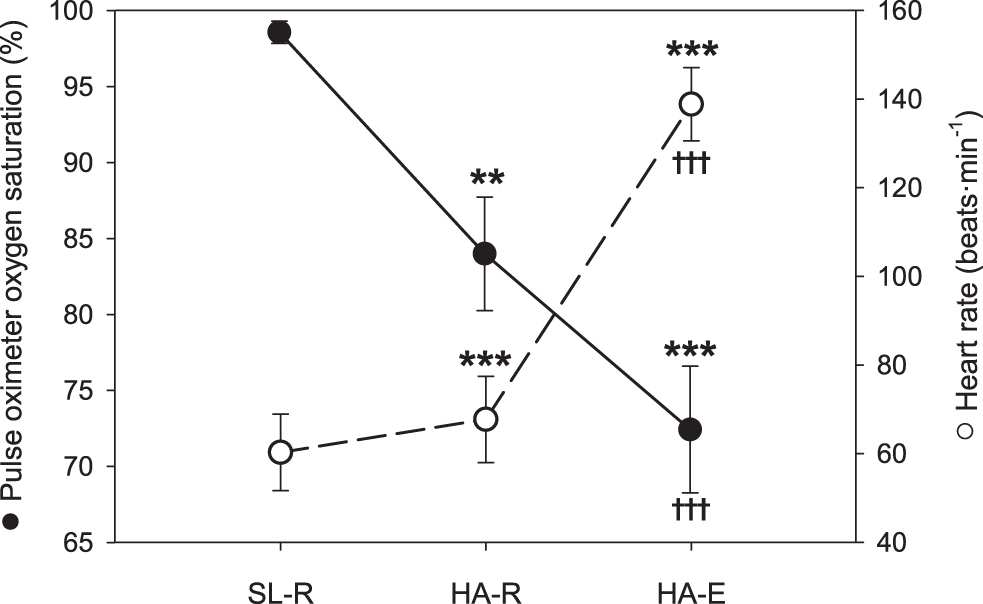
SpO2 (black circles, left scale) and HR (white circles, right scale) at different conditions. Statistical significance (p < 0.05) is denoted by asterisks (*) for the comparison to SL-R and by cross (†) for the comparison between HA-R and HA-E at simulated altitude (4,000 m). Two symbols indicate p < 0.01 and three symbols mean p < 0.001. HA-E, high altitude after exercise; HA-R, high altitude at rest; HR, heart rate; SL-R, sea level at rest; SpO2, pulse oximeter oxygen saturation.

Individual changes in SpO2, HR, and DLCOadj from HA-R to HA-E in each one of the seven unacclimated elite swimmers. DLCOadj, diffusing capacity of the lungs for carbon monoxide; HA-E, postexercise at high altitude; HA-R, resting position at high altitude.
Regarding SpO2, there were a significant interaction between SpO2 and the studied conditions (F = 124.17, p < 0.001,
Regarding HR, there were a significant interaction between HR and the studied conditions (F = 175.86, p < 0.001,
Discussion
The main finding of this study is that there were no changes in any lung diffusion parameter during the exposure to 4,000 m in the hypobaric chamber (HA-R and HA-E), suggesting that the cardiopulmonary system of healthy subjects cope well with a short-term exposure to exercise at high altitude.
During an exposure to HA, a hypobaric pulmonary vasoconstriction and a raise in pulmonary arterial pressure are produced (West, 2012), conditions that may be aggravated by the high cardiac output and high pulmonary flow induced by exercise (Naeije and Chesler, 2012; Marabotti et al., 2017). In some cases an additional functional reserve can be recruited to improve membrane O2 diffusing capacity during exercise in hypoxia (Hanson et al., 1989; Taylor et al., 2016).
Regarding the literature, hypoxic exercise does not acutely impair lung diffusion (Guenette et al., 2007; de Bisschop et al., 2012), although some studies have found a slight increase (Snyder et al., 2006; Taylor et al., 2016) or decrease (Senn et al., 2006; Agostoni et al., 2013).
The DLCO response to short-term hypobaric hypoxia may be complex. Several hypotheses can explain our results. The hypobaric exposure could have been too short to induce interstitial fluid accumulation and thus a reduction in DLCO, although some relevant risk factors to the development of pulmonary edema were induced in our experimental design such as rapid ascent rate, high altitude, and intense exercise. However, the proposed exercise protocol could have been insufficient to present a challenge in the respiratory system. Therefore, the HR got during exercise (139 ± 9 bpm) could not be enough to stress lung diffusion.
The time of exposure to hypoxia and the intensity of the exercise may be decisive to find an increase, no changes, or a decrease in DLCO. In a recent study, elite swimmers acclimated to 1,850 m had a significant decrease in DLCO after a similar exercise protocol even at lower simulated altitude (García et al., 2020). However, that cycling session was conducted after a swimming training within a 14-day altitude training camp and under normobaric hypoxia conditions (3,000 m). In addition, in this previous study, a lower HR in acclimated athletes may result in less lung perfusion and therefore greater diffusion limitation.
Dynamics of lung diffusing equilibrium may change depending on intensity, duration of the stimulus and interindividual physiological status. In addition, the similarity between hypobaric and normobaric hypoxia stimuli are still under discussion (Viscor et al., 2018; Millet and Debevec, 2020; Richalet, 2020), which could have affected the divergent results.
Apart from that, a maintained balance between the reduction in alveolar–capillary diffusion secondary to interstitial fluid accumulation and the increase in capillary lung perfusion because of the presented increase in HR (Bates et al., 2011; Taylor et al., 2014) could also explain the lack of changes in DLCO. Therefore, the induced increase in interstitial lung fluid could have been masked by the additional recruitment of the pulmonary vasculature during hypoxic exercise.
The appearance of pulmonary edema or the reduced transit time under specific conditions of low PO2 and high flow of the blood such as exercise may provoke diffusion disequilibrium (Torre-Bueno et al., 1985; Ayappa et al., 1998), limiting the O2 uptake in the lungs and the supplementary increases in DLCO. In our study, we did not measure SIPE with direct techniques (computed tomography [CT]-scan or X-ray), but it cannot be dismissed that some interstitial fluid was still accumulating. The partition of DLCO into its membrane (DM) and capillary blood volume (VC) components (Roughton and Forster, 1957) is necessary to understand whether the absence of changes in lung diffusion capacity is related to changes in alveolar–capillary diffusion from basal to postexercise in hypoxia.
Regarding the response in SpO2, there was an expected decrease in SpO2 during the studied conditions. Aquatic athletes such as artistic swimmers (Bjurstrom and Schoene, 1987) and divers (Foster and Sheel, 2005) have a low hypoxic ventilatory response, which is associated with high-altitude pulmonary edema (HAPE)-susceptible individuals (Hohenhaus et al., 1995). That is why, in some cases, elite athletes have been described as more susceptible to HAPE than control subjects (Hohenhaus et al., 1995). However, we could not associate this serious decrease in SpO2 (72% ± 5%) to a diffusion limitation.
One concern of the study is the use of indirect measures of interstitial lung fluid. Although DLCO has been consistently associated with an increase in extravascular lung water (Snyder et al., 2006; Clarenbach et al., 2012), a combined study of DLCO and diffusion capacity of the lung for nitric oxide (DLNO) would be more accurate to detect very mild interstitial fluid accumulation (Dehnert et al., 2010), because DLNO reflects more sensitively the changes in membrane diffusing capacity (Zavorsky and Van Der Lee, 2017). Additional measurements of cardiac output or stroke volume could also explain the disassociation between the raise in HR and the unchanged DLCO after HA-E.
One strength of this study is that all the DLCO measurements were taken at 30 seconds to 1 minute after exercise. Most of the studies assess DLCO 30–120 minutes after exercise suggesting that the potential decrease in DLCO is because of blood volume redistribution to the peripheral organs after exercise, a hypothesis that may be dismissed in our study.
In conclusion, this study shows that submaximal exercise during acute exposure to high altitude does not change lung diffusing capacity in elite swimmers, suggesting that healthy participants can deal with this type of combined environmental stressors without compromise of respiratory exchange. However, this study does not definitively show that submaximal exercise during acute exposure to altitude does not impair alveolar–capillary diffusion in the lungs, because of the possible interference between the VC and DM in our exercise protocol. Some methodological limitations in this study do not allow to completely rule out the possibility of the unchanged lung gas diffusion not being also due, at least in part, to the small number of subjects studied, the relatively short duration and intensity of the exercise performed at simulated altitude, and the intrinsic inaccuracy of this type of gas exchange measurements.
Further studies should consider measurements of CT scan, DLNO, DM, and VC to fully understand the physiological implications of severe acute hypoxic exercise in the lungs.
Footnotes
Acknowledgments
The authors thank all participants for their time and commitment in undertaking this study and the coach from the Sabadell Swimming Club, Alex López, for his collaboration during the study. Also the authors thank Álvaro Sánchez–Nieva (Sanro Electromedicina) for kindly supplying the equipment needed to conduct this research. The authors are grateful to Lynette Stewart for her help in the proofreading of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.