
Abstract
Ribeiro Baptista, Bruno, Morgane Faure, Gimbada Benny Mwenge, Capucine Morelot-Panzini, Christian Straus, Thomas Similowski, and Jésus Gonzalez-Bermejo. Feasibility of a hypoxic challenge test under noninvasive ventilation versus oxygen in neuromuscular patients with chronic respiratory insufficiency. High Alt Med Biol. 22:346–350, 2021.
Background:
The British Thoracic Society recommendations suggest that all patients with an oxygen saturation (SpO2) <85% during a hypoxic challenge test (HCT) should receive supplemental oxygen during air travel. However, neuromuscular patients already using ventilatory support are a specific population and noninvasive ventilation (NIV) during a flight could be an alternative to oxygen for hypoxemia correction, through the augmentation of ventilation.
Methods:
We conducted a comparative, observational study of neuromuscular patients with chronic respiratory failure, requiring nocturnal mechanical ventilation, who were planning to take a flight. HCT was performed with a ventilated canopy placed over the patient's head or the patient's home ventilator. The positive threshold value chosen for the HCT was <90% SpO2.
Results:
HCTs were performed on 13 adults with neuromuscular diseases using their home ventilator. Among them, 11 had a positive HCT. For all patients with a positive test, hypoxemia was corrected (SpO2 to >90%) by oxygen therapy (+9 [6–12]%, p = 0.0029). Patient's home ventilator also significantly increased the SpO2 by 8 [7–12]% (p = 0.016). Correction of SpO2 during the HCT was not different between oxygen and NIV. NIV was associated with a significant decrease in pressure, end tidal, carbon dioxide (PetCO2) (−10 [−16 to −7.5] mmHg, p = 0.04).
Conclusions:
The performance of an adapted HCT in home-ventilated patients with a neuromuscular pathology may be useful in a personalized treatment plan for air travel. NIV can be a new alternative to oxygen therapy for neuromuscular patients planning to take a flight.
Introduction
In 2018, 4
In 2011, the British Thoracic Society (BTS) recommended performing a hypoxic challenge test (HCT) for all patients planning air travel with severe restrictive lung disease (vital capacity <1 l), especially for those with hypoxemia and/or hypercapnia, as well as for those requiring ventilatory support (Ahmedzai et al., 2011). If the SpO2 at the end of the test remains >85%, oxygen supplementation is not required. Below this value, it is recommended to add 2–4 l/min of oxygen through a nasal cannula. However, the correction of hypoxemia in patients with chronic respiratory failure due to advanced neuromuscular disease can be achieved by ventilatory support, which allows the patient to reach a level of ventilation equivalent to that of a normal subject (Mestry et al., 2009). Few studies have investigated the use of a ventilator instead of oxygen to correct hypoxia during air travel in these particular patients.
This study was designed to evaluate the feasibility of an HCT under noninvasive ventilation (NIV) and to compare the correction of hypoxemia by increasing ventilation with NIV to that by oxygen therapy during an HCT in patients with chronic respiratory failure due to neuromuscular diseases already treated with home ventilatory support.
Methods
We conducted a comparative, observational study in the respiratory medicine department of the Pitié Salpêtrière Hospital (Paris) over a 6-month period. We extracted retrospectively the data from the medical files from patients tested before air travelling. The study was approved by the ethics committee from the Institutional Review Board of the French Learned Society for Respiratory Medicine (CEPRO 2012-039). Written informed consent was obtained from all subjects.
Patients were included if they suffered from chronic respiratory failure due to neuromuscular disorders and required nocturnal mechanical ventilation, and if they were planning a flight. Patients with nontreated cardiovascular diseases, recent myocardial infarction, cardiac arrhythmia, pregnancy, Forced Expiratory Volume in the first second < 30% due to obstructive disease, pulmonary arterial hypertension, infectious tuberculosis, or ongoing pneumothorax with persistent air leak and major hemoptysis were excluded (Ahmedzai et al., 2011). Data collected were age, diagnosis, sitting and supine force vital capacity, SpO2, expired CO2 (pressure, end tidal, carbon dioxide [PetCO2]), room air blood gases, and daily adherence to home mechanical ventilation.
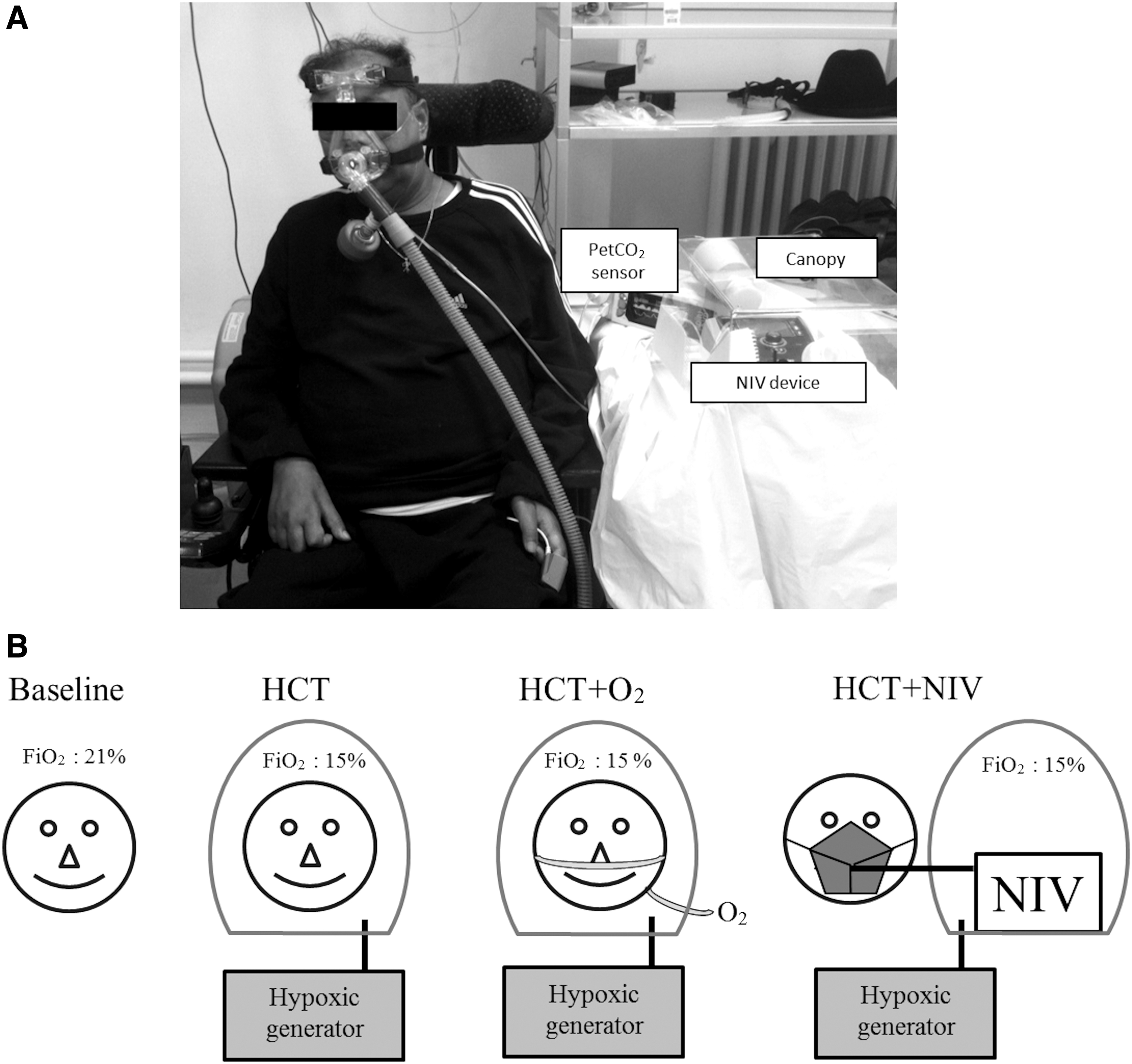
The HCT was performed with a ventilated canopy placed over the patient's head or the patient's home ventilator (Fig. 1A) and connected to a hypoxia generator (HYPOXICO, Inc., Jalhay, Belgium). The extraction of O2 was adapted to obtain a stable FiO2 of 15% ± 0.2%. FiO2 was measured using an FiO2 sensor (MAXTEC, Inc., UT) placed inside the canopy. The measurement of SpO2, PetCO2, heart rate, and respiratory rate was performed using an integrated monitor (Capnocheck® Plus; Smiths Medical PM, Inc., WI), including pulse oximetry and nasal cannula for measuring CO2. Oxygen was administered using another nasal cannula previously placed in superposition of the Capnocheck cannula. The HCT was performed with the patients seated at rest in four successive measurements (15 min each): (i) spontaneous ventilation, room air (baseline), (ii) under the canopy, spontaneous ventilation, FiO2 of 15%, if the test was positive (SpO2 <90%), (iii) under the canopy, spontaneous ventilation, FiO2 of 15%, with an oxygen flow of 2 l/min, and finally (iv) under patient's home ventilator, FiO2 of 15% (Fig. 1B). Dyspnea and headaches were measured at the end of each period by visual analog scales (VAS) rated from 0 to 10.
We chose a positive value for the HCT of <90% SpO2, which is different from that of the BTS recommendation (positive <85% of SaO2). Indeed, patients with neuromuscular disease or extrapulmonary restrictive chest wall deformity are more at risk of hypoxemia during an HCT, even with a resting saturation of >95% (Masa et al., 1997). Our choice of 90% was selected for two reasons. First, the related effect of hypoxemia, such as an increase in respiratory rate, was observed at <90% of the SpO2, suggesting a lower respiratory tolerance. Second, the BTS threshold is common to all respiratory disease, broadly based on studies that include obstructive lung disease. Our patients had normal lung parenchyma associated with reduced ventilatory adaptation in a hypoxemia condition. Thus, a threshold of 90% appeared to be more clinically relevant for this neuromuscular population. It was a choice of caution; it is difficult to formally prove that a patient with severe diaphragmatic dysfunction can remain with an SpO2 between 85% and 90% for a long time.
A p-value of <0.05 was considered statistically significant. Quantitative variables were compared using a Friedman's test and a post hoc Dunn test and the results expressed as their standard value (median and interquartile range). Qualitative variables were compared using Fisher's exact test and are expressed in terms of numbers and percentage. All statistical analyses were performed using GraphPad Prism software.
Results
Thirteen patients were included, of whom seven had amyotrophic lateral sclerosis. Their characteristics are presented in Table 1.
Baseline Characteristics (n = 13)
The values shown are median and interquartile range, except for gender and disease.
Other: Central core disease, Steinert's disease, two diaphragmatic dysfunction, and two Charcot Marie Tooth neuropathy.
FVC, force vital capacity; NIV, noninvasive ventilation; PaCO2, partial pressure of carbon dioxide, arterial; PaO2, partial pressure of arterial oxygen.
At baseline, median blood gas measures were a PaO2 of 82 mmHg and a partial pressure of carbon dioxide, arterial (PaCO2) of 41 mmHg. All patients performed the HCT. The median SpO2 was 95% at baseline. By the end of the test, the SpO2 of 11 patients had fallen to <90% (Fig. 2). Among these patients, the SpO2 of two had fallen to <85%. The median fall of SpO2 was 7 [5.5–8.5]% relative to the baseline SpO2 (p < 0.001). There was no significant change in the PetCO2 during spontaneous ventilation at the end of the HCT.
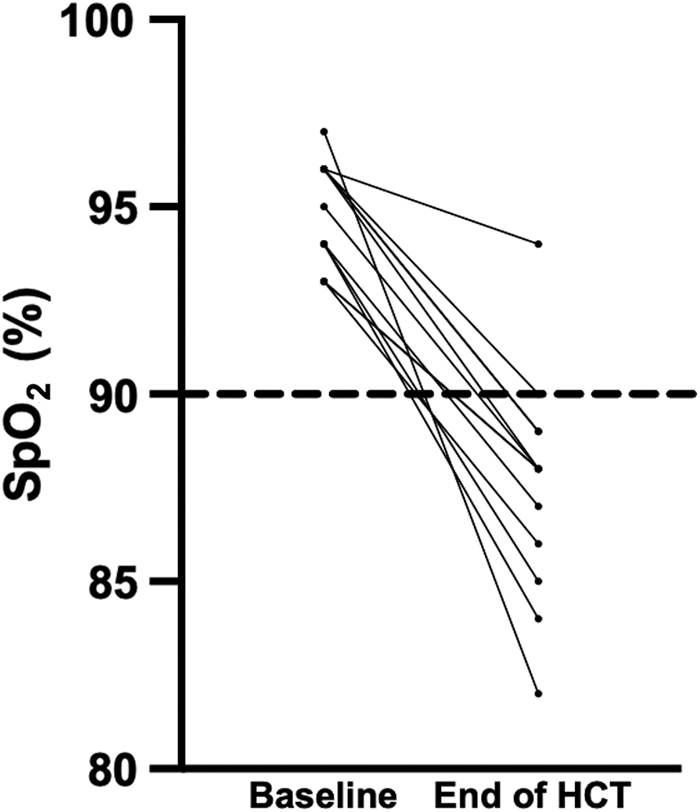
SpO2 at baseline and at the end of the HCT. Each line represents one patient (n = 13). Two patients shared lines from 96% to 89% and 93% to 88%. The dashed line indicates the positivity threshold of the test. SpO2, oxygen saturation.
An oxygen flow of 2 l/min allowed a correction of SpO2 to >90% for all positive HCT patients (+9 [6–12]%, p = 0.0029). In comparison, patient's home ventilator significantly increased the SpO2 by 8 [7–12]% (p = 0.016). Oxygen was not more effective than NIV for SpO2 correction during the HCT (Fig. 3). There was a significant decrease in PetCO2 only with NIV (−10 [−16 to −7.5] mmHg, p = 0.04). The HCT was not associated with a significant increase in the respiratory rate and the VAS score for dyspnea. Three tests were prematurely stopped: one because of dyspnea (at the end of HCT), one because of dyspnea and headache (at the end of HCT + O2 period), and one on request by the patient (at the end of HCT). No other patients reported a change in the VAS for dyspnea or headache.

Comparison of SpO2
Discussion
Our study shows that a preflight HCT is feasible under NIV in neuromuscular patients. The study also shows that SpO2 drops below 90% under a 15% FiO2 in majority of such patients (11 out of 13 in this study), and that NIV corrects hypoxemia in all cases.
HCT is achievable for patients using NIV under a canopy coupled to a hypoxia generator. In contrast to other already available methods using a Douglas bag or a Venturi mask, it is easily achievable directly at the patient's bedside, making it accessible to patients with motor disabilities or respiratory failure. Its speed of acquisition (45 min for a complete test) allows its routine use. Moreover, unlike conventional methods, it allows the evaluation of alternative therapies, such as mechanical ventilation. The order of different periods of the test was planned to avoid the necessity of re-establishing a stable hypoxia multiple times, which would have lengthened the experiment. However, a potential effect of the sequence cannot be excluded and the results could be different with another sequence.
NIV was always as effective as oxygen therapy in our group of patients. NIV appeared to be an acceptable alternative therapy, with physiological advantages like decreasing CO2 level. Furthermore, Winck et al. (2010) showed that a patient with a neuromuscular disease, who is correctly ventilated, without supplemental oxygen, can maintain SpO2 throughout a flight. In our study, the PetCO2 did not significantly decrease during the HCT because of a possible lack of ventilatory adaptation in this particular population. Indeed, hypoxemia normally induces a stimulation of the central respiratory drive leading to an augmentation of ventilation to maintain the oxygen level. In the case of normal respiratory mechanics, it should have led to a significant decrease in CO2 level. The interpretation of the PetCO2 is limited by the measurement method and should be considered with caution, given the potential for washout of this signal by NIV flows. However, the evolution of this parameter is in favor of the absence of hypercapnia during an HCT with oxygen or NIV.
We can assume that this favorable effect of NIV would be even more obvious for patients with more advanced respiratory failure. Even if not significant, probably because of the small number of subjects, the increase in respiratory rate at the initiation of hypoxia was well corrected by NIV. Importantly, this respiratory frequency was always higher than the minimum frequency set on the ventilator and therefore corresponded to the patients' “voluntary” frequency. These results suggest that the respiratory effort under NIV is reduced, and therefore the risk of respiratory exhaustion during longer exposure to hypoxemia, such as during air travel prolonged several hours, may decrease with NIV.
Conclusion
We conclude that performing an adapted HCT for home-ventilated patients with a neuromuscular pathology is useful to choose a personalized treatment for air travel. NIV allows sufficient hypoxemia correction for certain patients and can be used instead of oxygen therapy during air travel for this population. NIV can therefore be a new alternative for patients planning to take a flight.
Footnotes
Authors' Contributions
Concept and design: J.G.-B., T.S., C.M.-P., and C.S. Analysis and interpretation: B.R.B., G.B.M., T.S., and J.G.-B. Drafting the article for important intellectual content: B.R.B., M.F., G.B.M., C.S., C.M.-P., T.S., and J.G.-B. All authors have reviewed and approved the article before submission.
Acknowledgment
We thank Grégoire Justeau for proofreading this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study did not benefit from any private funding. Logistical support was provided by “Association pour le Développement et l'Organisation de la Recherche en Pneumologie et sur le Sommeil, ADOREPS,” a nonprofit organization devoted to the promotion of respiratory and sleep research. The study was supported by the program “Investissement d'Avenir ANR-10-AIHU 06” of the French Government.