
Abstract
Forrer, Aglaia, Philipp M. Scheiwiller, Maamed Mademilov, Mona Lichtblau, Ulan Sheraliev, Nuriddin H. Marazhapov, Stéphanie Saxer, Patrick Bader, Paula Appenzeller, Shoira Aydaralieva, Aybermet Muratbekova, Talant M. Sooronbaev, Silvia Ulrich, Konrad E. Bloch, and Michael Furian. Exercise performance in central Asian highlanders: A cross-sectional study. High Alt Med Biol. 22:386–394, 2021.
Introduction:
Life-long exposure to hypobaric hypoxia induces physiologic adaptations in highlanders that may modify exercise performance; however, reference data for altitude populations are scant.
Methods:
Life-long residents of the Tien Shan mountain range, 2,500 – 3,500 m, Kyrgyzstan, free of cardiopulmonary disease, underwent cardiopulmonary cycle exercise tests with a progressive ramp protocol to exhaustion at 3,250 m. ECG, breath-by-breath pulmonary gas exchange, and oxygen saturation by pulse oximetry (SpO2) were measured.
Results:
Among 81 highlanders, age (mean ± SD) 48 ± 10 years, 46% women, SpO2 at rest was 88% ± 2%, peak oxygen uptake (V′O2peak) was 21.6 ± 5.9 mL/kg/min (76% ± 15% predicted for a low-altitude reference population); peak work rate (Wpeak) was 117 ± 37 W (77% ± 17% predicted), SpO2 at peak was 84% ± 5%, heart rate reserve (220 − age − maximal heart rate) was 28 ± 17/min, ventilatory reserve (maximal voluntary ventilation − maximal minute ventilation) was 68 ± 32 l/min, and respiratory exchange ratio was 1.03 ± 0.09. Peak BORG-CR10 dyspnea and leg fatigue scores were 5.1 ± 2.0 and 6.3 ± 2.1. In multivariable linear regression analyses, age and sex were robust determinants of Wpeak, V′O2peak, and metabolic equivalent (MET) at peak, whereas body mass index, resting systolic blood pressure, and mean pulmonary artery pressure were not.
Conclusions:
The current study shows that V′O2peak and Wpeak of highlanders studied at 3,250 m, near their altitude of residence, were reduced by about one quarter compared with mean predicted values for lowlanders. The provided prediction models for V′O2peak, Wpeak, and METs in central Asian highlanders might be valuable for comparisons with other high altitude populations.
Introduction
When travelling to high altitude, environmental partial pressure of oxygen decreases causing hypoxemia. Associated physiological responses to maintain organ functions and mitigate hypoxemia and tissue hypoxia are an increase in minute ventilation and associated clearance of CO2, an increase in heart rate, a rise of hematocrit, and a left shift of the oxygen-binding curve of hemoglobin owing to hypoxia-related hyperventilation (Calbet and Lundby, 2009; West et al., 2012). However, physiological responses to acute hypoxemia remain incomplete, leading, among others, to sustained impairments in aerobic exercise performance. Proposed underlying exercise-limiting factors in healthy during short trips to high altitude (days to weeks) are pronounced hypoxemia (Latshang et al., 2013), alveolar-capillary diffusion limitations, reduced maximal heart rate and cardiac output (Grover et al., 1986; Fulco et al., 1998; Latshang et al., 2013; Mourot, 2018), and pronounced blood volume distribution toward respiratory muscles (Lenfant and Sullivan, 1971; Calbet et al., 2003).
Besides acute hypoxemia experienced by travelers during professional or recreational activities at high altitude, almost 140 million people permanently live at altitudes >2,500 m (Moore et al., 1998) and are exposed to chronic hypoxemia. However, the consequences of chronic hypoxemia on their exercise performance are not fully understood. It has been suggested that chronic hypoxemia might directly and indirectly limit exercise performance. Indirect mechanisms might be through development of chronic altitude illnesses by excessive increases in pulmonary artery pressure (PAP) and/or excessive red blood cell production resulting in high altitude pulmonary hypertension (HAPH) and/or chronic mountain sickness (CMS), respectively (León-Velarde et al., 2005). The optimal adaptation to chronic hypoxemia is unknown and depends on various factors including absolute altitude of residents, hypoxic ventilatory response, exposure time to chronic hypoxemia, and others. Furthermore, prediction equations for exercise performance have exclusively been validated at low altitudes and no information is available on high altitude populations, making the distinction between impaired exercise performances owing to chronic hypobaric hypoxia versus cardiorespiratory diseases almost impossible. Preliminary evidence emerged that some acute effects during hypobaric hypoxia persist, e.g., it has been proposed that maximal heart rate remains reduced in Han Chinese permanently living at high altitude, whereas this was not observed in Tibetans (Kayser et al., 2019). Underlying mechanisms might be hypoxia and increased parasympathetic activity owing to hypoxic pulmonary vasoconstriction with subsequent subclinical increase in PAP (Kayser et al., 2019). Further influencing factors altering exercise performance include erythrocytosis, or the increased minute ventilation owing to lower air density. However, quantitative assessment of exercise performance in high altitude populations are scarce, therefore, the purpose of this study was to quantify exercise performance, describe underlying physiological constraints, and provide prediction models for exercise performance in a representative sample of healthy central Asian highlanders permanently living at high altitude.
Methods
Setting
Data collection of this cross-sectional study took place between July 1 and August 31, 2017, at the Aksay health post located at 3,250 m (mean barometric pressure 519 mmHg), Tien Shan mountain range, Kyrgyzstan. Highlanders traveled by horse or car to the place of examination and stayed there overnight. The data on cardiopulmonary exercise testing (CPET) were collected within the framework of a large prospective cohort study investigating the progression of PAP in highlanders (Latshang et al., 2017). Results of the CPET examination have not been previously published.
Participants
Included were high altitude natives, born, raised, and currently living >2,500 m, of both sexes, older than 18 years, and permanently living in the Aksay area at an altitude of 2,500 – 3,500 m. Exclusion criteria were regular intake of medication, diagnosed or uncontrolled systemic hypertension, history of congenital heart disease, pulmonary diseases (e.g., chronic obstructive pulmonary disease), heavy smoking (>10 cigarettes/day, >20 pack-years), or excessive erythrocytosis (hemoglobin concentrations in men >21 g/dL; women >19 g/dL). Because of the various definitions of HAPH, highlanders with any PAP were included in this CPET study (Lichtblau et al., 2020). The majority of highlanders living at the Aksay plateau are nomadic herdsmen, hunters, or on military duty owing to the proximity to the border to China. Because of the lack of roads on the plateau, highlanders are highly skilled horse riders, however, rather inexperienced in running or cycling.
All participants gave their written informed consent. The study was approved by the ethics committee of the National Center of Cardiology and Internal Medicine in Bishkek, Kyrgyzstan (01-8/433), and all research was performed in accordance with relevant guidelines/regulations.
Assessments
Medical history and clinical examination
A medical history was obtained and a clinical examination including measurements of height, weight, blood pressure, heart rate, and pulse oximetry was performed on the day of arrival. Resting echocardiography of the right heart was performed to assess PAP and right heart function while participants rested in supine position in a heated, quiet, and darkened room. Detailed results of echocardiography have been published previously (Lichtblau et al., 2020).
Spirometry
Spirometry and maximal voluntary ventilation maneuvers were performed according to international guidelines (Miller et al., 2005).
Cardiopulmonary exercise testing
Incremental work-rate testing was performed on a stationary bicycle (Ergoselect 200; Ergoline GmbH, Bitz, Germany) with a progressive ramp protocol starting at 20 W and an increase by 10 W/min until exhaustion according to international guidelines (American Thoracic Society; American College of Chest Physicians, 2003). Throughout the exercise session, highlanders were vigorously encouraged to pedal as long as possible. Exercise was stopped when the revolutions per minute (RPM) fell <40 for more than 5 seconds. A tightly fitted face mask was individually adjusted for each highlander and respiratory gas concentrations, tidal volume, and respiratory rate (differential pressure transducer) were measured breath-by-breath by a metabolic unit (Ergostick; Geratherm Medical AG, Gschwenda, Germany) to compute minute ventilation (V′E), oxygen uptake (V′O2), carbon dioxide output (V′CO2), and derived variables (American Thoracic Society; American College of Chest Physicians, 2003). The metabolic measurement system has been validated by our laboratory at 2,048 m and showed good agreements over multiple point calibrations by medical gas mixtures at predefined levels of minute ventilation and gas flows (Metabolic calibration kit; VACUMED, CA) (data not published). Ambient barometric pressure, temperature, and relative humidity were continuously determined by the exercise system. Airflow and volume calibrations were performed by a calibrated 3-l syringe. The CO2 and O2 gas analyzer were calibrated by a two-point calibration using ambient air and gas mixture of 5%/16% CO2/O2. All calibrations were performed twice daily, in the morning and after lunch before the first exercise sessions. Bicycle ergometers were calibrated (Ergoline ergotest 550) for RPM and power before and after the study and remained within the acceptable deviation of <2 RPM/min and <3 W. SpO2 by finger pulse oximetry and a four-lead electrocardiogram were continuously recorded (Ergostick; Geratherm, Gschwenda, Germany). At rest on the bicycle and directly after the CPET, dyspnea and leg fatigue was assessed using the BORG CR10 scale (Borg, 1998). After the exercise, the stopping reasons were noted.
Normal reference values for Kyrgyz (a Turk ethnic group) were not available, therefore, we compared findings of this study with widely used normal values for V′O2max and maximal work rate (watts) from Hansen et al., 1984 and Koch et al. (2009) because they provide robust and well-assessed normal values for a healthy Caucasian population. To better express the metabolic requirements for the maximal work capacity during CPET, metabolic equivalents (METs) were calculated by dividing peak V′O2 by resting V′O2 (American Thoracic Society; American College of Chest Physicians, 2003). Breathing reserve was calculated by
Arterial blood gases
Resting arterial blood was drawn from the A. radialis on the nondominant forearm after awakening and a fasting period of 12 hours. The blood sample was immediately analyzed (Rapidpoint500; Siemens, Switzerland) to obtain pH, arterial partial pressure of CO2 (PaCO2), arterial partial pressure of O2 (PaO2), bicarbonate, hematocrit, hemoglobin, and oxygen saturation (SaO2). No arterial blood gases at peak exercise were assessed.
Statistical analysis
Normal distribution of data was verified by Shapiro–Wilk tests. Data are summarized by mean ± SD. Analyses were performed per-protocol, (1) including all participants completing the CPET assessment, and (2) including only highlanders fulfilling at least one criterion of maximal exhaustion as defined previously. To compare intra-individual changes from rest to peak exercise, linear mixed regression models including individual participants as random effects were applied. In the absence of a healthy low altitude control group, we defined the lower limit of normal for V′O2peak as 80% of the mean predicted value and by the lower 95% confidence interval of the mean predicted value calculated from Koch et al. (2009). To obtain normal values of peak V′O2 (L/min), work capacity (watts), and METs in this population, we performed multivariable regression analyses including baseline variables as potential predictors in highlanders fulfilling at least one criterion of maximal exhaustion as defined previously. p < 0.05 was considered as statistically significant.
Results
A total of 118 highlanders were screened for eligibility and 93 (79%) attended the CPET examination. From these, seven prematurely terminated exercise because of knee pain, four assessments were unusable owing to electrical power loss and one developed a panic attack during exercise because of the facemask. Therefore, 81 highlanders were included in the per-protocol analysis (Fig. 1). From these, 37 of 81 (46%) highlanders were women, and the population studied had a mean ± SD age of 48 ± 10 years (range 27 – 69), body mass index (BMI) of 27.0 ± 4.4 kg/m2, mean PAP of 29.9 ± 6.3 mmHg, and normal lung function (Table 1). Resting arterial blood gas analyses revealed normal pH, hypoxemia, mild hypocapnia, a lower than normal bicarbonate (normal range 22 – 26 mmol/L), and a higher than normal hemoglobin (normal range in men 13.8–18.0 g/dL and women 12.1 – 15.1 g/dL) concentration (Table 1).
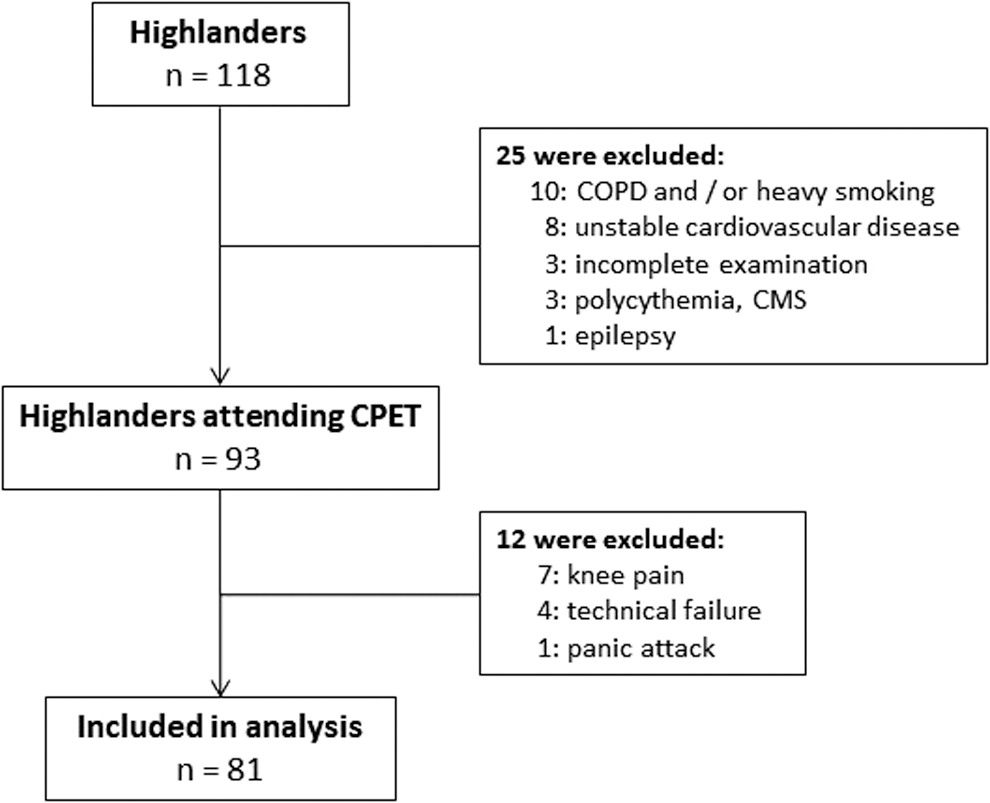
Participant flow. CMS, chronic mountain sickness; COPD, chronic obstructive pulmonary disease; CPET, cardiopulmonary exercise testing.
Demographic Characteristics of Highlanders
Values are presented as mean ± SD.
Maximal exhaustion criteria unadjusted for high altitude as outlined in Table 3.
BMI, body mass index; FEV1/FVC, forced expiratory volume in 1 second/forced vital capacity; PaCO2, arterial partial pressure of CO2; PaO2, arterial partial pressure of O2; PAP, pulmonary artery pressure; SaO2, arterial oxygen saturation.
Resting and peak-exercise values are summarized in Table 2.
Cardiopulmonary Exercise Testing
Values are presented in mean ± SD.
Maximal exhaustion criteria unadjusted for high altitude as outlined in Table 3.
Fulco et al. showed that in acute hypoxia, V′O2max decreases by 8% by every 1,000 m of altitude gain starting at 700 m, however, whether these corrections are applicable to Kyrgyz highlanders is unknown.
External work efficiency was calculated as the linear slope of ΔV′O2/ΔWork rate between 25% and 75% of maximal exercise performance.
Breathing reserve was calculated by
p < 0.05 peak exercise versus rest.
METs, metabolic equivalents, which were calculated by dividing V′O2peak by resting V′O2; V′CO2, carbon dioxide output; V′O2, oxygen uptake; MVV, maximal voluntary ventilation.
Before exercise, highlanders had normal systemic blood pressure, respiratory exchange ratio, low dyspnea and leg fatigue, and hypoxemia. Resting heart rate was normal and minute ventilation 11.3 ± 2.7 l/min associated with high ventilatory equivalents for O2 and CO2 and low end-tidal partial pressure of CO2 (Table 2).
With exercise, highlanders had worsening hypoxemia and increasing ventilatory equivalents for O2 but the ventilatory equivalent for CO2 was reduced compared with resting. Mean heart rate, minute ventilation, and respiratory exchange ratio at peak exercise did not reach predicted values (Table 2).
Overall, 63% of all highlanders fulfilled at least one criterion for maximal exhaustion (Table 3). The calculated median (95% confidence interval) of V′O2 at peak exercise based on Koch et al. in these highlanders was 28.8 (20.5 – 37.1) mL/kg/min. Measured V′O2peak was 21.6 ± 5.9 mL/kg/min and corresponded to 76% ± 15% of the predicted values proposed by Koch et al. (2009) and 77% ± 15% predicted values proposed by Hansen et al., 1984. The Wpeak was 117 ± 37 W, corresponding to 77% ± 17% of the predicted values of healthy lowlanders. The external work efficiency of highlanders was 11.84 ± 3.48 mL/min/W (Table 2). Main subjective stopping reasons were leg fatigue (81%) and dyspnea sensation (60%), which was in accordance with the higher rated BORG CR10 score for leg fatigue compared with dyspnea at peak exercise (Table 2).
Comparable results were achieved when performing subgroup analysis in highlanders fulfilling at least one criterion of maximal exhaustion (Tables 1 and 2).
Multivariable regression analyses in highlanders fulfilling at least one criterion for maximal exhaustion using baseline variables to predict exercise performance expressed as V′O2peak (L/min), Wpeak, and METs revealed that age and sex were robust predictors, whereas BMI, resting systolic blood pressure, and mean PAP were not (Table 4 and Fig. 2). These regression models can be used to calculate normal V′O2, Wpeak, and METs reference values for highlanders.

Individual and predicted values of maximal oxygen uptake (Panel
Proportion of Highlanders Fulfilling Objective Criteria for Maximal Exhaustion at Peak Exercise (n = 81)
Baseline Predictors of Exercise Performance in Highlanders Fulfilling at Least One Criterion of Maximal Exhaustion—Multivariable Linear Regression Analyses
n = 52.
BMI, body mass index; PAP, pulmonary artery pressure; BP, blood pressure.
Discussion
We studied exercise performance and associated physiological changes in life-long central Asian highlanders at altitude of residence (3,250 m) during CPET. Compared to sea level reference values, the V'O2peak and Wpeak of high altitude residents was reduced by about one quarter to 76% – 77% predicted. Exercise limitation was related to an exercise-induced worsening of hypoxemia, high ventilatory equivalents for oxygen uptake and carbon dioxide output, a reduced external work efficiency and a lower peak heart rate than predicted for age. Although performing a CPET until exhaustion accompanied by vigorous encouragement, only 63% of highlanders reached standard maximal effort criteria (American Thoracic Society; American College of Chest Physicians, 2003). Findings were confirmed by a sub-group analysis in highlanders fulfilling maximal exhaustion criteria established for lowlanders. Therefore, these findings indicate that predicted maximal physiological values and maximal effort criteria defined for exercise near sea level might not be applicable to high altitude populations tested at their altitude of residence. This study provides normal values for V'O2peak, Wpeak and METs in central Asian highlanders, which might be valuable for comparisons to other high altitude populations.
Acute exposure to hypobaric hypoxia leads to hypoxemia and increased heart rate at rest; however, maximum heart rate and stroke volume have been shown to be reduced and result in lower maximum cardiac output and V′O2peak values compared with sea-level conditions (Fukuda et al., 2010; Mourot, 2018). It has been suggested that V′O2max decreases approximately by 8% for each 1,000 m altitude gain starting from 700 m (Fulco et al., 1998). Despite the reduced V′O2peak at high altitudes, larger proportions of the blood volume are needed for respiratory muscles and the heart owing to the hypoxia-induced relative hyperventilation and increased heart rate (Lenfant and Sullivan, 1971; Calbet et al., 2003). Among others, these responses to acute hypobaric hypoxia lead to a lower exercise capacity in healthy unacclimatized persons exposed for days to several weeks to hypobaric hypoxic conditions. Whether these exercise-limiting factors persist during life-long exposure to high altitude remains to be elucidated. However, beneficial adaptations such as erythrocytosis and angiogenesis may improve oxygen carrying capacity and exercise performance. In contrast, increases in PAP might reduce exercise performance. Furthermore, genetic adaptations to high altitude play an important role in exercise performance (Kayser et al., 2019). However, whether central Asian highlanders are as well adapted as other high altitude natives or if their exercise-limiting factors are different from lowlanders acutely exposed to high altitude remains to be clarified.
Maximal work rate and its limiting factors in an otherwise healthy high altitude population are not well understood, and only little data are published so far. Reasons might be that most research in hypobaric hypoxia focused on exercise capacity in athletes or in healthy young acclimatized compared with unacclimatized men (Sun et al., 1990; Niu et al., 1995; Curran et al., 1998; Lundby et al., 2006; Calbet and Lundby, 2009). Some studies have also examined highlanders suffering from CMS (Groepenhoff et al., 2012). One previous study conducted by Niu et al. (1995) compared native Tibetan highlanders with a group of Han Chinese lowlanders exposed for 27 months to 3,690 m. They found no difference in V′O2peak (Tibetans: 41.5 ± 8.60 mL/kg/min and migrated Chinese: 39.7 ± 4.15 mL/kg/min), but Wpeak was higher in Tibetans interpreted as better gross mechanical efficiency compared with migrated Han Chinese. The higher work rate with similar V′O2peak in Tibetans suggest that life-long exposure or genetic background does — at least partially — play a role in exercise capacity at high altitude (Niu et al., 1995).
In comparison with Tibetans, Kyrgyz highlanders migrated more recently, i.e., a few hundred years ago, to high altitude. The reported higher prevalence of chronic altitude illnesses (CMS and HAPH) in Kyrgyz highlanders compared with Tibetans may indicate that they are genetically not as adapted to living at high altitude (MacInnis and Koehle, 2016; Lichtblau et al., 2020). In Kyrgyz highlanders, the V′O2peak reached by the subjects was 21.58 ± 5.90 mL/kg/min and is clearly lower compared with the findings from Niu et al. However, there is a large age discrepancy between the two studies (mean age in Kyrgyz: 48 years; in the cited study: 20 years). When comparing the V′O2peak % predicted, the populations are comparable (V′O2peak in Kyrgyz: 76% predicted, Tibetans: 74% and Han Chinese: 84%), suggesting that Tibetans, presumably one of the best acclimatized populations worldwide, reach values around the lower limit of normal of V′O2max reference values assessed at sea level. The observed reduction in V′O2peak of 24% in this study (and 26% in the cited trial conducted at 3,650 m) is similar to the calculated 20% (and 24%) reduction in V′O2max expected during acute hypobaric hypoxia at 3,250 and 3,650 m, respectively (Fulco et al., 1998). When applying altitude adjustments for HRmax maximal heart rate and V′O2peak, then highlanders of the current trial do reach 88% and 94% predicted for HRmax and V′O2peak suggesting that they were near their point of exhaustion when stopping exercise. These findings indicate that exercise performance remains impaired during chronic hypoxia in central Asian highlanders. Whether the underlying exercise-limiting factors are identical to the limiting factors during acute exposure, remains to be elucidated. The findings in Tibetans and now in Kyrgyz highlanders strengthen the evidence that normal reference values obtained in sea-level populations might not be applicable to high altitude populations, although, in one study, 15 Peruvian highlanders living at 4,350 m were able to achieve sea-level values for V′O2peak (Groepenhoff et al., 2012). Among others, altitude-related, subclinical changes in ventilatory efficiency, hypoxemia, erythropoiesis, maximum heart rate, subjective symptoms of exertion, and excessive rise in PAP might complicate the interpretation of CPET and associated normal values for V′O2peak and Wpeak.
Therefore, this study provides prediction equations for V′O2peak, Wpeak, and METs in central Asian highlanders, which might be of value for comparisons with other high altitude populations (Table 4 and Fig. 2). Furthermore, these predictions can be used to assess exercise performance in highlanders with preexisting morbidities. It is intriguing that resting mean PAP was not a predictor in these models; however, this finding is in accordance with a study performed in Peruvian highlanders with CMS, healthy highlanders, and lowland newcomers to 4,350 m. They showed that V′O2peak was similar between the groups, although highlanders with CMS had much higher mean PAP values and suffered from pronounced hypoxemia compared with healthy lowlanders and newcomers to high altitude (Groepenhoff et al., 2012). Moreover, the prediction models revealed that age and gender were consistent determinants of exercise performance, whereas BMI and resting blood pressure were not.
Limitations
Our study lacks a healthy low altitude Kyrgyz control group. However, Kyrgyz is a Turk ethnic group and by applying normal reference values from Koch et al. in Caucasians, we believe that we applied the most appropriate references for Turk and therefore, Kyrgyz ethnicity. Nevertheless, it would be desirable to have Kyrgyz low altitude reference values in the future. Furthermore, heart rate reserve, breathing reserve, and respiratory exchange ratio, according to sea-level guideline cutoff values, suggested that 37% of participants did not reach maximal exhaustion defined for CPET testing. Lactate was not measured at the end of exercise and we cannot rule out premature termination of exercise because of lack of motivation. However, this seems rather unlikely because the highlanders were highly motivated to participate in our study and were vigorously encouraged throughout the CPET. Furthermore, subgroup analysis in highlanders fulfilling criteria for maximal exhaustion achieved similar results. Assessing exercise performance in high altitude nomads is challenging, because they are used to horse riding and not to running or cycling. Therefore, we cannot rule out some degree of inefficiency because of the rather unusual type of exercise. The prediction models were derived from highlanders with an age range of 31 – 69 years and BMI of 18 – 38 kg/m2, therefore, derived normal values outside these boundaries should be interpreted with caution.
It would be of great interest to examine whether acute administration of oxygen can improve exercise performance in these highlanders by reversing some physiologic manifestations of chronic hypoxemia as seen in Peruvian highlanders breathing acute normoxia (Favier et al., 1995). Furthermore, in future studies it would be of high relevance to compare healthy Kyrgyz lowlanders acutely exposed to high altitude and compare their exercise performance and exercise-limiting factors to Kyrgyz highlanders permanently living at high altitude.
Conclusion
Our study is the first to investigate exercise performance of Central Asian highlanders at the altitude of their residence of 3,250 m. We found that peak oxygen uptake and work rate were ∼75% of corresponding values predicted for reference populations of lowlanders studied near sea level. Exercise-limiting factors included hypoxemia associated with a reduced ventilatory efficiency for V′O2 and V′CO2, a lower external work efficiency possibly related to an increase in oxygen demand of nonexercising muscles, and adaptation in control of ventilation and heart rate. This study provides reference values for V′O2peak, Wpeak, and METs in central Asian highlanders and may help to distinguish between altitude-related and disease-related exercise-limiting factors in highlanders affected by cardiopulmonary disease.
Footnotes
Authors' Contributions
A.F. and M.F. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. S.U., K.E.B., and M.F. have developed the study concept and design. All authors have contributed to the data acquisition, analysis, or interpretation. A.F. and M.F. wrote the article draft, whereas P.M.S., M.L., S.S., P.B., P.A., S.U., and K.E.B. critically revised the article for important intellectual content. Statistical analysis has been conducted by A.F., K.E.B. and M.F., M.M., U.S., N.H.M., S.A., A.M., and T.M.S. further provided administrative, technical, or material support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the OPO Foundation. Siemens Health Engineers and Philips Respironics provided some equipment for the study. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.